
Medicaid and Permanent Supportive Housing for Chronically Homeless Individuals: Emerging Practices From the Field
Martha Burt, Carol Wilkins, and Gretchen Locke Abt Associates
This is one of two reports examining the use of Medicaid to cover services for individuals experiencing chronic homelessness, particularly in Permanent Supportive Housing (PSH). It describes existing practices in the field of communities currently serving homelessness and formerly homeless individuals Medicaid beneficiaries.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This Report is available on the Internet at:
"Acknowledgments
The research team for this project, Carol Wilkins, Martha Burt and Gretchen Locke, acknowledge the assistance of a variety of individuals and organizations. First, we greatly appreciate the guidance and support of the Project Officer, Emily Rosenoff and Gavin Kennedy, both of the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services (HHS). We also appreciate the thoughtful review and comments on the report provided by staff at HHS, the Centers for Medicare and Medicaid Services (CMS), the Substance Abuse and Mental Health Services Administration (SAMHSA), the Health Resources and Services Administration (HRSA), the U. S. Department of Housing and Urban Development (HUD), and the U.S. Interagency Council on Homelessness (USICH). At Abt Associates, Dr. Jill Khadduri and Dr. Meryl Finkel provided thoughtful review throughout the project.
We also acknowledge the extensive assistance provided by policymakers and practitioners in the communities we visited for the research. We met with many people in some of these public agencies and nonprofit organizations, which are listed below alphabetically by case study location. The list identifies a few specific individuals who were extraordinarily helpful, including those who facilitated introductions, arranged meetings, and provided responses to follow-up questions.
Chicago, Illinois
AIDS Foundation of Chicago
Community Counseling of Chicago
Cook County Health and Hospitals System
Corporation for Supportive Housing
Illinois Department of Healthcare and Family Services: Julie Hamos and others
Illinois Department of Human Services, Division of Mental Health
Health and Disability Advocates
Heartland Health Outreach: Karen Batia and others
Michael Reese Health Trust
Office of the Governor, State of Illinois
Polk Brothers Foundation
Thresholds
Trilogy
Connecticut
Chrysalis Center: Sharon Castille
Columbus House: Allison Cunningham
Community Health Resources: Jill Benson and Heather Gates
Connecticut AIDS Resource Coalition: Shawn Lang
Connecticut Department of Corrections: Dan Bannish
Connecticut Department of Mental Health and Addiction Services: Barbara Geller, Steve Dilella, and others
Connecticut Department of Social Services: Mark Schaefer and others
Connecticut Legal Rights Project: Jan Vantassle
Connecticut Office of Policy and Management: Judy Dowd
Corporation for Supportive Housing: Richard Cho, Sarah Gallagher, and Kevin Irwin
National Alliance on Mental Illness: Shelia Amdur, Consultant
Partnership for Strong Communities: Mike Hanely, Alicia Woodsby, and others
Los Angeles, California
A Community of Friends
California Department of Health Care Services
California Pacific Medical Center
Clinica Oscar Romero
Corporation for Supportive Housing
Exodus Recovery, Inc.
Housing Authority of the City of Los Angeles
Housing Works
Insure the Uninsured Project/L.A. Health Action
JWCH Institute
L.A. Care Health Plan
Los Angeles Christian Health Centers
Los Angeles County Chief Executive Office: Libby Boyce and others
Los Angeles Department of Health Services: Marc Trotz, Cheri Todoroff, and others
Los Angeles Department of Mental Health: Maria Funk and others
Los Angeles Homeless Services Authority
Mental Health America of Los Angeles
Northeast Valley Health Corporation
OPCC
San Fernando Valley Community Mental Health Center
Skid Row Housing Trust
St. Joseph Center
Step Up on Second
To Help Everyone (T.H.E.) Clinic
United Homeless HealthCare Partners
Venice Family Clinic
Watts Health Center
Minnesota
Catholic Charities
Corporation for Supportive Housing
Guild, Inc.
Heading Home Hennepin
Heading Home Minnesota
Hearth Connection
Hennepin County Human Services and Public Health Department: Markus Klimenko and others
Hennepin Health: Jennifer DeCubelis and others
Medica
Mental Health Resources, Inc.
Minnesota Council of Health Plans
Minnesota Department of Human Services
People, Inc.
South Metro Human Services
Spectrum Mental Health
St. Stephen's Human Services
Touchstone Mental Health
New Orleans, LA
Alternatives Living, Inc.
Department of Health and Hospitals, Permanent Supportive Housing Program: Christine Rohrer
Department of Health and Hospitals, Office of Behavioral Health: Ann Darling
Department of Health and Hospitals: Medicaid Human Services District: Craig Coenson
Jefferson Parish Human Services Authority
Louisiana Office of Aging and Adult Services: Michell Brown and Craig Coenson
National Alliance on Mental Illness, New Orleans
NOLA AIDS Task Force
Northwest Human Services
Resources for Human Development
Start Corp.
Technical Assistance Collaborative: Marti Knisley
Unity of Greater New Orleans
Volunteers of America
Washington, DC
Community Connections
Community of Hope: Kelly Sweeney McShane
Department of Human Services, Homeless Programs
Department of Mental Health: Steve Baron
Department of Health Care Finance
Green Door
Pathways to Housing-DC: Christy Respress
So Others Might Eat
Unity Health Care: Janelle Goetcheus and others
Acronyms
The following acronyms are mentioned in this report.
| ACO | Accountable Care Organization |
|---|---|
| ACT | Assertive Community Treatment |
| ADA | Americans with Disabilities Act |
| AFC | AIDS Foundation of Chicago |
| AIDS | Acquired Immune Deficiency Syndrome |
| APM | Alternative Payment Methodology |
| AS | ACUTE Stabilization |
| ASO | Administrative Services Organization |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| B.E.S.T. | Los Angeles Behavioral and Educational Strategies and Training Program |
| CCE | Care Coordination Entity |
| CCHHS | Cook County Health and Hospital System |
| CDBG | Community Development Block Grant |
| CHIP | Children's Health Insurance Program |
| CMS | HHS Centers for Medicare and Medicaid Services |
| CNOM | Costs Not Otherwise Matchable |
| COHS | County-Operated Health System |
| DAH | Direct Access to Housing |
| DC | District of Columbia also known as Washington, D.C. |
| DHS | Los Angeles County Department of Health Services |
| DMH | District of Columbia Department of Mental Health |
| DOJ | U.S. Department of Justice |
| DSM | Diagnostic and Statistical Manual of Mental Disorders |
| DSM-IV-TR | Diagnostic and Statistical Manual of Mental Disorders, IV Version, Text Revision |
| FFS | Fee-For-Service |
| FPL | Federal Poverty Level |
| FQHC | Federally Qualified Health Center |
| FSP | Full Service Partnership |
| FUSE | Frequent Users Systems Engagement |
| GAF | Global Assessment of Functioning Scale |
| HCBS | Home and Community-Based Services |
| HCH | Health Care for the Homeless |
| HEARTH | Homeless Emergency Assistance and Rapid Transition to Housing Act |
| HFS | Illinois Department of Healthcare and Family Services |
| HHO | Heartland Health Outreach |
| HHS | U.S. Department of Health and Human Services |
| HIV | Human Immunodeficiency Virus |
| HMIS | Homeless Management Information System |
| HMO | Health Maintenance Organization |
| HRSA | HHS Health Resources and Services Administration |
| HUD | U.S. Department of Housing and Urban Development |
| ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
| ICM | Integrated Care Model |
| IDA | Interim Disability Assistance |
| IMD | Institution for Mental Disease |
| LA | Los Angeles |
| LBHP | Louisiana Behavioral Health Partnership |
| LIHP | Low Income Health Program |
| LIHTC | Low Income Housing Tax Credit |
| LOCUS | Level of Care Utilization System |
| MCCN | Managed Care Community Network |
| MCO | Managed Care Organization |
| MH | Mental Health |
| MHSA | Mental Health Services Act |
| MMD | Major Mental Disorder |
| PATH | Projects for Assistance in Transition from Homelessness |
| PHA | Public Housing Authority |
| POC | Plan of Care |
| PPS | Prospective Payment System |
| PSH | Permanent Supportive Housing |
| PSHP | Permanent Supportive Housing Program |
| SAGA | State Administered General Assistance |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SIF | Social Innovation Fund |
| SMI | Serious Mental Illness |
| SNAP | Supplemental Nutrition Assistance Program |
| SOAR | SSI/SSDI Outreach, Access, and Recovery |
| SPMI | Serious/Severe and Persistent Mental Illness |
| SRO | Single-Room Occupancy |
| SSA | Social Security Administration |
| SSDI | Social Security Disability Insurance |
| SSI | Supplemental Security Income |
| T4H | Together4Health |
| TCM | Targeted Case Management |
| UCLA | University of California, Los Angeles |
| USICH | U.S. Interagency Council on Homelessness |
| VA | U.S. Department of Veterans Affairs |
| VADD | Vulnerable Adults and People with Developmental Disabilities |
| VI-SPDAT | Vulnerability Index and Service Prioritization Decision Assistance Tool |
Executive Summary
Permanent supportive housing (PSH) offers subsidized housing for formerly homeless people with disabilities and chronic health conditions. It provides flexible and individualized support services that are offered to tenants, who can participate on a voluntary basis. PSH services focus on promoting long-term housing stability, recovery, and improved health. PSH service providers may deliver or coordinate access to treatment for health, mental health, and substance use disorders. PSH programs also directly provide case management services and supports to help people who are homeless obtain and retain housing. The housing component of PSH provides a platform for improving health and for changing patterns of health care utilization, with the appropriate use of health and behavioral health care replacing frequent use of emergency rooms and inpatient hospitalization. This in turn reduces the public cost burden of inappropriate use of crisis services.
When the Federal Government first committed to ending chronic homelessness in 2003, it was understood that PSH would be a big part of reaching that goal. Since then, federal and other resources have helped to add more than 140,000 PSH beds, bringing the PSH-bed total to 284,298 in January 2013.1 The impact of these new units is evident: The number of people with histories of chronic homelessness found in unsheltered locations decreased by 25 percent between 2007 and 2013 (HUD 2013).
PSH programs use multiple funding sources to ensure that supportive services are available to their tenants. Medicaid reimbursement has often been used to pay for some of the services provided to some PSH tenants. Some PSH tenants who were enrolled in Medicaid were eligible to have some aspects of their health and behavioral health care covered even before Medicaid expansion under the Affordable Care Act. As of January 1, 2014, 25 states and the District of Columbia expanded Medicaid coverage to adults aged 18-64 if their household income was at or below 133 percent of the federal poverty level, as allowed under provisions of the law. The expansion means that many more PSH tenants as well as people still experiencing chronic homelessness because they have very low incomes are now eligible for Medicaid. Thus, understanding Medicaid's potential as a funding source for the services needed by Medicaid beneficiaries living in PSH is even more important now, for those newly eligible as well as for those eligible under the rules that applied in 2013 and earlier.
In anticipation of changes stemming from the Affordable Care Act, the U.S. Department of Health and Human Services (HHS), Office of the Assistant Secretary for Planning and Evaluation (ASPE), contracted with Abt Associates in October 2010 to conduct a study to explore the roles that Medicaid, Health Centers, and other HHS programs might play in providing services for people who had experienced chronic homelessness before moving into PSH. This study examined the intersection of three pieces of a complex puzzle that if assembled correctly can end chronic homelessness: (1) chronic homelessness itself; (2) permanent supportive housing; and (3) Medicaid's potential to fund health-related services for people experiencing chronic homelessness or living in PSH. It looked at program innovations already in practice, because the best indicators of Medicaid's potential usefulness to people experiencing homelessness are the ways that today's providers are using Medicaid to cover some of the support in supportive housing. That support includes health and behavioral health care for people who have been chronically homeless and are now living in PSH.
Findings reported here are based on more than two years of observing developments in six communities.2 Each community had been pursuing at least one of several innovations, many of which are still evolving, including (1) early expansion of eligibility based on Affordable Care Act income rules (Connecticut, District of Columbia, and Minnesota); (2) Medicaid waivers to create coverage for low-income people through new types of health plans that offer a "bridge" to the expanded coverage available under the Affordable Care Act (Cook County, Illinois; Los Angeles County; and the State of California); (3) linking Medicaid-covered mental health and behavioral health services to housing assistance to create PSH; (4) expanding the types of services covered by Medicaid (Louisiana, Minnesota); (5) involving Health Centers (Chicago, Los Angeles); (6) expanding the role of managed care (District of Columbia, Louisiana, Minnesota, and Los Angeles); and (7) developing entirely new structures for integrating physical and behavioral health care with links to housing (Chicago, Minnesota).
This report focuses on the innovations that are primarily mechanisms for coordinating and integrating health care (for physical, mental, and substance use conditions and supports to help people get and keep housing. The impetus for these innovations is the increasingly widespread recognition that people with complex needs require integrated care and housing stability for better health outcomes, better patient and client experiences, and more cost-effective care. Our study leads us to the following conclusions:
Many useful approaches are being pioneered in study communities. Using Medicaid to fund services to serve PSH tenants is complicated, but it can be done.
Medicaid will not cover every service, but it can be a vital funding source for services needed by PSH tenants.
Many types of Medicaid providers--managed care organizations, Health Centers, behavioral health providers, and Accountable Care Organizations--are playing important roles.
Summary of Key Findings
1. Introduction
When the Federal Government first committed to ending chronic homelessness in 2003, it understood that permanent supportive housing (PSH) would be a big part of reaching that goal. Since then, federal and other resources have helped to add more than 140,000 PSH beds, bringing the PSH-bed total to 284,298 in January 2013.5 The impact of these new units is evident: the number of people with histories of chronic homelessness found in unsheltered locations decreased by about 25 percent between 2007 and 2013 (HUD 2013).
Going forward, an understanding of Medicaid's potential as a funding source for PSH services is especially important because eligibility for Medicaid expanded dramatically on January 1, 2014, in 25 states and the District of Columbia. Because they are very poor, most people experiencing homelessness are Medicaid-eligible as a result of the expansion, even if they were not eligible under the rules that applied in 2013 and earlier.
In anticipation of changes stemming from the Affordable Care Act, the U.S. Department of Health and Human Services (HHS), Office of the Assistant Secretary for Planning and Evaluation (ASPE), hired Abt Associates in October 2010 to conduct a study to explore the roles that Medicaid, Health Centers, and other HHS programs might play in providing services linked to housing for people who experienced chronic homelessness before moving into PSH. This study examined three pieces of a complex puzzle that if assembled correctly can end chronic homelessness: (1) chronic homelessness itself; (2) permanent supportive housing; and (3) Medicaid's potential to fund health-related supportive services. It looked at program innovations already in practice, because the best indicators of Medicaid's potential usefulness to people experiencing homelessness are the ways that today's providers are using Medicaid to cover some of the support in supportive housing; that is, health and behavioral health care for people who have been chronically homeless and are now living in PSH.
Findings reported here are based on more than two years of observing developments in six communities.6 Each community has been pursuing at least one of several innovations, many of which are still evolving, including (1) early expansion of eligibility based on Affordable Care Act income rules (Connecticut, District of Columbia, and Minnesota); (2) Medicaid waivers to create coverage for low-income people through new types of health plans that offer a "bridge" to the expanded coverage available under the Affordable Care Act (Cook County, Illinois; Los Angeles County; and the State of California); (3) linking Medicaid-covered mental health and behavioral health services to housing assistance to create PSH; (4) expanding the types of services covered by Medicaid (Louisiana, Minnesota); (5) involving Health Centers (Chicago, Los Angeles); (6) expanding the role of managed care (District of Columbia, Louisiana, Minnesota, and Los Angeles); and (7) developing entirely new structures for integrating physical and behavioral health care with links to housing (Chicago, Minnesota).
This report focuses on the innovations that are primarily mechanisms for coordinating and integrating health care (for physical, mental, and substance use conditions) and supports to help people get and keep housing. The impetus for these innovations is the increasingly widespread recognition that people with complex needs require integrated care for better health outcomes, better patient and client experiences, and more cost-effective care. Our study leads us to the following conclusions:
Many useful approaches are being pioneered in study communities. Using Medicaid to fund services needed by PSH tenants is complicated, but it can be done.
Medicaid will not cover every service, but it can be a vital funding source for some of the services needed by PSH tenants.
Many types of Medicaid providers--including Medicaid managed care organizations, Health Centers, behavioral health providers, and Accountable Care Organizations--are playing important roles.
Conditions are ripe for improving care coordination and services integration, but achieving these goals will take the work of many parties. Some communities are already experiencing the benefits from Medicaid expansion, both from Medicaid covering services for individuals who are homeless and from local and state resources being freed up to fund nonreimbursable PSH program costs.
1.1. Purpose and Audience for This Report
This report presents the results from six community case studies we conducted from early 2011 through early 2013. We observed as these communities designed and implemented service funding strategies such as Medicaid waivers, state plan amendments, health care delivery system reforms, and new programs and partnerships.
The report reviews these strategies and the progress communities are making. It describes innovations in accessing Medicaid to cover the care and care coordination needed to help people who have complex health and behavioral health conditions and who have been homeless a long time, with the ultimate goal of helping such people: (1) access and retain PSH; (2) improve their health; and (3) use health and behavioral health care more efficiently and effectively.
The primary audiences for this report are: (1) people who are actively engaged in or providing leadership in Medicaid administration and related programs and systems; and (2) homeless service system administrators and PSH providers and their partners who are preparing for and navigating change. The authors assume readers have a relatively advanced knowledge of the concepts and terminology used in this field.7
1.2. The Three Pieces of the Puzzle: Chronic Homelessness, Permanent Supportive Housing, and Medicaid
Before turning to the details of innovations in the use of Medicaid for PSH tenants and people continuing to experience chronic homelessness, we briefly describe the three pieces of the puzzle that comprise the focus of our work--chronic homelessness, PSH, and Medicaid. The remainder of the report explores different aspects of Medicaid for people who are chronically homeless and for PSH tenants, including eligibility and enrollment, the most common ways that Medicaid has been used, recent innovations, and developments in progress.
1.2.1. Chronic Homelessness
Before 2012, the U.S. Department of Housing and Urban Development's (HUD's) definition of chronic homelessness applied only to single adults (i.e., not to families). A person would be considered chronically homeless if he or she was currently homeless, had one or more disabling conditions, and had been homeless either continuously for at least a year or had four or more episodes of homelessness within the past three years. The Homeless Emergency Assistance and Rapid Transition to Housing (HEARTH) Act of 2009 (P.L. 112-141) extended the definition of chronic homelessness to include families. HUD rules that went into effect on January 4, 2012, now define either a single adult or a parent in a homeless family as chronically homeless if he or she has been continuously homeless for a year or more or has experienced a total of 12 months of homelessness during the previous three years.8
Many people experiencing chronic homelessness have been on the streets or in shelters for years. They often have complex physical, mental, and substance use conditions that can only be ameliorated if they have a safe, stable, and secure living environment. Their homelessness may exacerbate health difficulties, making it increasingly unlikely that they can get back into housing on their own. Further, many of them make frequent and avoidable use of emergency rooms and inpatient hospitalization. This use of expensive crisis health services has been a major motivator for PSH development. PSH support services have been shown to help tenants avoid actions and decisions that would cause them to lose their housing again and revert to homelessness and previous patterns of crisis health service use (Burt, Wilkins, and Mauch 2011; Caton, Wilkins, and Anderson 2007).
Among people experiencing chronic homelessness, some are more likely to have access to PSH and comprehensive care than others. People living with mental illness severe and chronic enough to qualify for Medicaid and for Medicaid-reimbursable mental health services are likely to get the most comprehensive array of services thanks to states' use of some Medicaid program options (rehabilitative services and targeted case management).
1.2.2. Permanent Supportive Housing
What Is Permanent Supportive Housing?
At its simplest, permanent supportive housing (PSH) is an approach to subsidized housing that provides voluntary services for people with disabilities and chronic conditions to promote long-term stability, recovery and improved health. PSH offers flexible and individualized services on-site or off-site, delivered either by the same provider that operates the housing or through partnerships with community-based service providers. Supportive housing takes three primary forms:
Single-site housing, in which the tenants receiving support services live in units in the same apartment building or a group of buildings that offer affordable housing; supportive services may be provided at the housing site, through home visits, or at other locations in the community.
Scattered-site housing, in which tenants live in apartments throughout the community, often leased from private owners with rental assistance provided through government subsidies; supportive services may be delivered through home visits or provided at other locations in the community.
Mixed housing, in which tenants live in developments, usually affordable housing, that contain a mix of supportive housing tenants and other tenants not part of the supportive housing program; supportive services may be delivered through home visits or provided at other locations in the community.
In PSH, housing is coupled with a broad array of supportive services--including treatment for health, mental health, and substance use disorders--to help people get and retain housing, with the services coordinated through case management or care coordination. The extent and intensity of services varies, but generally PSH is designed for people experiencing long-term homelessness and comes with varied and intensive service offerings. Over the past decade, PSH has increasingly moved to a housing-first approach, which has proven successful at bringing people in from the streets without requiring that active mental illness or substance use be controlled.9
Medicaid's IMD Exclusion
The discussion of Medicaid reimbursement for services in permanent supportive housing often raises questions about the Medicaid payment exclusion for Institutions for Mental Diseases (IMDs). Medicaid payment does not extend to services provided to individuals who reside in facilities that are over 16 beds that meet the definition of an IMD, except for services furnished pursuant to the state plan benefit, "inpatient psychiatric services for individuals under 21," or pursuant to an exclusion for individuals age 65 or older who reside in institutions that are IMDs. Medicaid defines an IMD as "a hospital, nursing facility, or other institution of more than 16 beds that is primarily engaged in providing diagnosis, treatment, or care of persons with mental diseases, including medical attention, nursing care, and related services. Regulations also indicate that an institution is an IMD if its "overall character" is that of a facility established and maintained primarily for the care and treatment of individuals with mental diseases.*
Unlike institutions, PSH offers housing in community settings, facilitating engagement and integration in the broader community. Regardless of whether the housing is scattered-site apartments or apartments in buildings that provide PSH for people with disabilities who have been homeless, PSH offers personcentered community-based support. The housing is subject to a lease or similar rental agreement. Tenants have privacy and autonomy in their own living units, and they are free to come and go when they wish. PSH generally meets the criteria CMS has established to define a home and community-based setting in which some Medicaid services can be provided. The supportive services that are available to persons with mental disorders who live in PSH may include diagnosis or treatment of medical or behavioral health conditions, but the primary purpose of PSH is housing, not treatment. People living in PSH can choose whether to get health care, treatment, and other supportive services from other providers in the community or from service providers who may be connected to the supportive housing program who may deliver some services on-site or through home visits. Continued tenancy in the housing is not contingent upon participation in supportive services offered by the PSH program.
* The IMD payment exclusion is in Section 1905(a) of the Social Security Act (the Act) in paragraph (B) following the list of Medicaid services. The definition of an IMD is in Section 1905(i) of the Act and in 42 CFR 435.1010 of the Code of Federal Regulations. The exclusion for individuals aged 65 and older is in Section 1905(a)(14) of the Act, and 42 CFR 440.140. The exception for individuals under age 21 is in Section 1905(a)(16) of the Act and 42 CFR 440.160. Medicaid guidance can be found at Section 4390 of the State Medicaid Manual.
Public Benefits of PSH
The housing component of PSH provides a platform for improving health and for changing patterns of health care utilization, with the appropriate use of health and behavioral health care replacing frequent use of emergency rooms and inpatient hospitalization. This in turn reduces the public cost burden of inappropriate use of crisis services. PSH accomplishes these changes through its service component, which includes health and behavioral health care coordination and recovery support services including support to remain in stable housing. Interest in accessing Medicaid funding for Medicaid-covered services stems from the services' proven potential to reduce Medicaid-covered hospitalizations and emergency room visits.
1.2.3. Medicaid
Medicaid is one of the top three sources of funding for services to PSH tenants (Burt 2008) and is used most frequently for people with serious mental illness (SMI). Medicaid is a health insurance program implemented through partnerships between states and the HHS Centers for Medicare and Medicaid Services (CMS). Although states develop their own Medicaid state plans within the basic parameters set by CMS in accordance with federal law, every state's Medicaid program is different. States must include a core set of benefits and may choose to offer additional benefits allowed by CMS. Through waivers and state plan amendments, states may add benefits for specific purposes or populations, establish structures for care delivery such as managed care organizations, and follow other approaches to fit their program to state needs and budget realities.
Before 2014, many PSH tenants were not eligible for Medicaid because they did not fall into one of the categories through which eligibility is established in their state. For most of our case study communities that situation changed between 2010 and 2013 through early expansion of Medicaid eligibility. The situation changed even more in 2014, when most people experiencing homelessness in many states, because of their low incomes, became Medicaid-eligible under the Affordable Care Act of 2010. Medicaid is only one of the strategies that communities have used to create and sustain permanent supportive housing. By statute, Medicaid cannot pay for housing or room and board in residential treatment facilities.
Three aspects of Medicaid are important to understand for the purposes of this study: (1) the types of services that are reimbursable under Medicaid; (2) who is eligible for Medicaid; and (3) what services are available only for persons with a particular level of need or disabling condition.
Medicaid gives persons who meet income and other eligibility requirements access to health care. Medicaid-eligible persons can receive the specific services for which they are determined to have a need, based on established medical necessity criteria. When looking at how Medicaid might be used to cover services for PSH tenants, it is critical to take into consideration the medical necessity criteria that apply to behavioral health or home and community-based services that may be delivered in conjunction with PSH. Many PSH tenants are likely to meet these criteria, which take into consideration diagnoses and functional impairments, while other PSH tenants who do not meet these criteria may not qualify to receive the same Medicaid-covered services.
As part of its Medicaid state plan, a state may choose to make community-based mental health services available to people with serious mental illness (SMI) by including optional benefits such as the Medicaid Rehabilitative services option or targeted case management. States may use a Medicaid Section 1915(c) waiver to offer home and community-based services (HCBS) for people whose disabilities are severe enough to qualify them for institutional placement, or add coverage for HCBS optional services under Section 1915(i) for people whose disabilities meet specified criteria. These HCBS benefits may cover some services and supports for people living in PSH. Chapters 2 through 7 describe these and other approaches in more detail.
Before full implementation of the Affordable Care Act, most Medicaid beneficiaries were eligible for Medicaid because: (1) they were disabled as defined by eligibility criteria for Supplemental Security Income (SSI); (2) they were children, pregnant, or members of family households that met Medicaid eligibility criteria; or (3) they were Medicare beneficiaries whose incomes were low enough to qualify them for Medicaid (known as dual-eligibles).
In the 25 states that are not going forward with Medicaid expansion at this time, these eligibility criteria will continue to apply in 2014 and beyond. But for the 25 states and the District of Columbia that have expanded Medicaid eligibility, most people experiencing homelessness and those living in PSH who were not Medicaid-eligible before 2014 will now qualify because they will meet income criteria (income lower than 133 percent of the federal poverty level).
Between 2011 and early 2013, the period during which the research team visited the six case study communities, states were pursuing ways to expand eligibility, types of care, care integration, or combinations thereof that benefited or were likely to benefit people with complex health care needs, including people experiencing chronic homelessness and PSH tenants. Well before 2014, some of these approaches brought significantly more people experiencing chronic homelessness and more PSH tenants into Medicaid or waiver coverage. These were people who previously would not have qualified because they did not have a qualifying disability and did not meet "categorical" eligibility criteria. However, it remains important to distinguish between the two groups of current or potential beneficiaries, those who do have a serious mental illness and those who do not, because the Medicaid-reimbursed services for which they qualify are often quite different. We therefore maintain this distinction in the following chapters.
1.3. The Context for Innovation
The approaches described in this report are being developed and implemented in a period of dramatic change and challenging circumstances. During the transitional period before the Affordable Care Act was fully implemented, stakeholders at all levels were attempting to sustain programs in a lean fiscal climate while designing new strategies that may work very differently in the future. Before proceeding to the details of our findings, we review some key elements of the federal, state, and local context influencing efforts to integrate care and link services with housing assistance for people with complex medical and behavioral health needs and extensive homeless histories.
1.3.1. State Priorities and Constraints
During the period covered by this research, late 2010 through 2012, state budgets were under tremendous pressure: unemployment rates were high; state tax revenues fell; and many state and local governments were forced to cut staff and reduce services. Funding for Medicaid benefits and funding for flexible services from other sources were among the cost areas under pressure. State officials were trying to manage existing programs and respond to new mandates with fewer staff. The U.S. Supreme Court's review and ruling on the Affordable Care Act and the 2012 presidential election contributed to the uncertainties experienced at the state and local level. Over the past several years in most of the states participating in this study, Medicaid program leaders and other state officials were consumed by the many tasks related to preparing for the full implementation of the Affordable Care Act in 2014, and they often talked about having "limited bandwidth" to pursue other program initiatives at the same time.
The commitment of state leadership to pursuing change is important to the progress we report in the six case study sites. For example, in Louisiana, the state's Department of Health and Hospitals was already committed to a complete redesign of its services for individuals with disabilities, including multiple waivers and state plan amendments. The state then made a commitment to HUD to guarantee that PSH services that received post-Hurricane Katrina Community Development Block Grant (CDBG) funding would be sustained. The state plays a key leadership role in Minnesota as well, where the Department of Human Services first designed and implemented a Health Care Delivery System demonstration that began in 2011, and recently designed a proposed Reform 2020 Section 1115 Medicaid waiver proposal that included many elements that could help pay for care coordination, housing stabilization, and integration of services. In other case study communities, philanthropic organizations, advocates, PSH providers, and representatives from local government have taken more prominent roles, working with state leadership to gain support for innovative approaches.
1.4. The Rest of This Report
The remaining chapters of this report describe existing and emerging service patterns and partnerships involving Medicaid providers aimed at moving toward more comprehensive and integrated health, behavioral health, and housing supports for people who are currently chronically homeless and for those now living in PSH. Most of the examples come from our six case studies. Each chapter begins with a summary of "highlights," capturing the key points in the chapter. Chapter 2 describes Medicaid eligibility and enrollment practices, including already-implemented changes and changes to come. Chapter 3 describes approaches to expanding coverage under waivers.
Chapter 4 discusses emerging models of coordinated care in Health Centers (including Federally Qualified Health Centers [FQHCs]) in partnerships that include behavioral health and housing. Chapter 5 reviews strategies implemented through public and nonprofit mental health agencies and programs to serve people with serious mental illness. Mechanisms include specialized Medicaid rules, covered services, and carve-outs. Chapter 6 presents mechanisms being implemented by managed care organizations, and Chapter 7 reviews innovative approaches to accountable care and coordination. Chapter 8 discusses challenges and opportunities related to linking Medicaid to PSH tenants, briefly describing issues and opportunities related to Olmstead, pending waivers, Health Home developments, and other current matters at our six case study sites. Chapter 9 summarizes our findings and offers conclusions. Throughout, we focus on evolving patterns of interagency cooperation that are helping to apply available support for integration of health and behavioral health care and housing.
2. Medicaid Eligibility, Services, and Enrollment Strategies
Chapter 2 Highlights
For decades, people have qualified for Medicaid benefits based on categorical eligibility. The two most common eligibility categories have been as follows:
The Covered Families and Children population--parents, children, and pregnant women whose household income is at or below the income eligibility levels established by states, which vary widely.
The Aged, Blind, and Disabled population--elderly and disabled individuals who qualify if they meet the age and disability criteria for receiving Supplemental Security Income (SSI) or the disability criteria for Social Security Disability Insurance (SSDI) and whose incomes are low enough to qualify for Medicaid.
In anticipation of the Affordable Care Act of 2010's expansion of Medicaid eligibility in 2014 to households with incomes below 133 percent of the federal poverty level, some states expanded Medicaid eligibility early in the two ways explained below:
Connecticut, Minnesota, and the District of Columbia used the Affordable Care Act's authority to implement early expansion of income-based Medicaid eligibility for some or all of the people who would become eligible in 2014 based on income.
California and Illinois used Section 1115 demonstration authority to waive certain Medicaid requirements in order to expand coverage. States have long been able to use Section 1115 Research and Demonstration waiver programs to define specific groups of Medicaid beneficiaries, who then receive a package of services appropriate to their needs even if they do not meet categorical eligibility criteria. Under these waiver programs, states receive federal Medicaid funds to match their own outlays at the Federal Medical Assistance Percentage assigned to their state. California and Illinois took advantage of Section 1115 authority to create low-income health plans to serve all or most of the low-income population that would become eligible for Medicaid in 2014 and create a "bridge to reform" for public health and "safety net" hospital systems.
For people experiencing chronic homelessness or living in permanent supportive housing, the importance of Medicaid eligibility based on income cannot be overstated. Expansion offers health insurance coverage to thousands in this population who have not otherwise met categorical eligibility criteria.
Services available under Medicaid include the Medicaid state plan (the array of services that anyone qualifying for Medicaid on a categorical basis would be able to receive) and Alternative Benefit Plans (the basic array of covered services that states must provide to those newly eligible for Medicaid based on income alone). These plans may be different than the Medicaid state plan but must include the ten essential health benefits specified in the Affordable Care Act.
2.1. Introduction
Eligibility is one thing; getting newly eligible people enrolled in Medicaid and maintaining enrollment is another. In the course of eligibility expansion, states and localities have had to develop a range of outreach and engagement strategies for identifying eligible people, helping them enroll, and helping them maintain or re-establish their eligibility when it comes time for recertification. Assistance to establish eligibility for SSI has also been a priority.
Using Medicaid-funded services to support people who live in permanent supportive housing requires that these PSH residents establish eligibility for and enroll in Medicaid or a program whose services are Medicaid-financed. This chapter reviews how eligibility has been established historically and what has changed since the Affordable Care Act became law in March 2010.
Before the enactment of the Affordable Care Act, Medicaid eligibility was based on categorical requirements; the only way for a state to expand eligibility was through a Section 1115 demonstration program. With an 1115 Medicaid demonstration, states could use matching federal funds to provide Medicaid eligibility or some form of coverage to people who did not meet categorical eligibility criteria.
This chapter first describes how people become Medicaid recipients under rules for categorical eligibility, which have been in place for decades and will continue to be applied into the foreseeable future. Second, we examine eligibility expansions that occurred in our six case study sites since the Affordable Care Act became law in 2010. The sites took different approaches to expanding coverage to people with histories of chronic homelessness and extensive service needs.
Connecticut, Minnesota, and the District of Columbia used the Affordable Care Act's authority to implement early expansion of Medicaid eligibility for some or all of the people who would become eligible in 2014 based on income.
California and Illinois are examples of states that used Section 1115 waivers to expand coverage. California's waiver allowed (but did not require) all counties to implement low-income health programs and most did, while the waiver for Illinois pertained only to Cook County. Waiver approval for Illinois came in late 2012, near the end of our study period. In California and Chicago, the waivers were intended to be a "bridge to reform," helping health care providers prepare for changes that were coming in 2014 with the implementation of the Affordable Care Act.
After discussing eligibility, this chapter briefly outlines Medicaid services and how the basis of an individual's eligibility might affect the array of services that individual can receive. The chapter concludes with descriptions of practices that case study sites have used to engage people experiencing homelessness in health care, to help them establish Medicaid eligibility, and to ensure that they maintain that eligibility consistently over time. Later chapters provide extended discussions of mental health services, case management, and care coordination, which are particularly important for people experiencing chronic homelessness or living in PSH. Our discussions include how eligibility for these specific activities is determined.
2.2. Establishing Eligibility
2.2.1. Categorical Eligibility for Medicaid
For decades, people have qualified for Medicaid benefits based on categorical eligibility. The two most common eligibility categories have been as follows:
The Covered Families and Children population--parents, children, and pregnant women whose household income is at or below the income eligibility levels established by states, which vary widely.10
The Aged, Blind, and Disabled population--elderly and disabled individuals who qualify if they meet the age and disability criteria for receiving Supplemental Security Income (SSI) or the disability criteria for Social Security Disability Insurance (SSDI) and whose incomes are low enough to qualify for Medicaid.
During the period covered by the case studies (2011-2013), most people experiencing chronic homelessness in the United States who became Medicaid beneficiaries did so on the basis of disability (usually mental illness) by first establishing their eligibility for SSI. Qualifying for either of these two categories is still an important way for people to establish Medicaid eligibility, and will be most important in the 25 states that are not going forward with eligibility expansion in 2014.
2.2.2. Income-Based Eligibility for Medicaid
The Affordable Care Act added an important new basis of eligibility to the two long-standing categories. The Act allows states to expand coverage to households with incomes up to 133 percent of the federal poverty level (FPL) without other "categorical" eligibility criteria. The intent is to provide all poor households with health insurance coverage by having them enroll directly into the state's Medicaid program. The Act's expanded eligibility provisions offer people experiencing homelessness or living in PSH an important opportunity to obtain coverage for health care that was difficult or impossible for them to obtain before 2014.11
When the Affordable Care Act became law, it allowed states to opt for "early implementation" of the income-based Medicaid expansion. Three jurisdictions selected for this study--Connecticut, the District of Columbia, and Minnesota--used the Affordable Care Act's authority to expand Medicaid eligibility based on income in 2010 or 2011 for some or all of those who would become eligible in 2014.12
For example, Connecticut was one of the three case study sites that expanded Medicaid eligibility early. In April 2011, Connecticut expanded Medicaid eligibility to adults without children with incomes of up to 56 percent of the poverty level, a population previously served in the state's State Administered General Assistance (SAGA) program. The number of newly enrolled Medicaid members was much greater than expected--roughly twice the SAGA enrollment.
Services for new enrollees were sometimes less than the full Medicaid state plan, as in the District of Columbia where the expansion population qualified for a basic level of Medicaid through health maintenance organizations (HMOs). Known as Childless Adult Medicaid, this plan came close to full Medicaid in that it included long-term care and mental health coverage, but it did not cover the full range of services that might be needed by someone with a disability.13
The Affordable Care Act also specified January 1, 2014, as the date when all states would expand Medicaid eligibility to households with incomes up to 133 percent of poverty, with full federal funding for newly eligible people provided during the first few years. Following the Supreme Court decision of June 2012 that ruled against mandating the expansion, 25 states and the District of Columbia made the decision to expand and 25 states are not going forward at this time, though they may decide to do so at a later date. Exhibit 2.1 shows which of our six case study sites did early expansion and which have gone forward with full expansion as of January 1, 2014.
EXHIBIT 2.1. Eligibility Expansion Approaches of the Six Case Study Sites
| State | Early Implementation, Enrolling Income-Eligible People into State Medicaid Plan | Section 1115 Waiver to Expand Coverage Through Plan with Limited Services and Providers | Going Forward with Full Expansion in 2014 |
|---|---|---|---|
| California | X | X | |
| Connecticut | X | X | |
| District of Columbia | X | X | |
| Illinois (Cook County only) | X | X | |
| Louisiana | |||
| Minnesota | X | X |
2.2.3. Expanded Eligibility Through Section 1115 Demonstration Programs
Another important way that states are able to extend Medicaid coverage to more households is through a Section 1115 demonstration program. These programs, which have been available for many years, allow states to use matching federal funds to provide some form of coverage to people who do not meet categorical eligibility criteria. Under these programs, states are allowed to waive certain federal requirements and may define specific populations and services to be covered. Some states have used these programs to expand coverage in ways that include people experiencing chronic homelessness or living in PSH.
California and Illinois sought Section 1115 demonstration authority to extend Medicaid-financed services to some part of the low-income population, including many people who were experiencing chronic homelessness. Counties designed and provided the nonfederal funding to implement Low Income Health Programs that were authorized under these waivers. The health plans established by the counties included more limits on services and providers than would be the case starting in 2014, and participation in these plans did not constitute enrollment in the state's Medicaid program. Rather, these two jurisdictions used their Section 1115 demonstration programs as a "bridge to reform," helping health care providers prepare for changes happening with full implementation of the Affordable Care Act.
In California, the Section 1115 program allowed counties to establish Low Income Health Plans that greatly extended eligibility for a package of basic health care services. Los Angeles County enrolled almost 200,000 newly covered persons in its plan by the end of 2012, and close to another 100,000 by the end of 2013.
Illinois received approval for a similar Section 1115 program in late 2012 that is active only in Cook County. This waiver provided new opportunities for coverage for income-qualifying adults in the year before they became eligible for Medicaid in 2014. CountyCare offered health care services through Cook County Health and Hospital Services and its community partners. The Cook County Health and Hospital System was expecting that enrollment of newly covered persons would total over 100,000 by the end of 2013.
2.3. Medicaid Eligibility for People Who Are Chronically Homeless
Many adults who are disabled and homeless have a serious mental illness (SMI). Some homeless adults have other disabling health conditions, including physical disabilities, serious medical conditions, brain injuries, or cognitive impairments. They may also have co-occurring substance use disorders.
As adults not living with children and therefore not part of the Covered Families and Children population, many people experiencing chronic homelessness have had a difficult time establishing categorical eligibility for Medicaid. Those who have been able to establish eligibility have done so through SSI based on disability. This will still be the primary route to Medicaid eligibility available to this population after January 2014 in states not expanding their Medicaid programs based on the income criterion available through the Affordable Care Act.
In some states, people who are homeless but whose health conditions do not meet the level of functional impairment required by SSI, or those whose disabilities are attributable to substance use disorders and therefore not eligible for SSI, have been eligible to enroll in Medicaid under the terms of a Medicaid 1115 waiver that predates the Affordable Care Act.14 Likewise, since passage of the Act and before 2014, people living in the six states that opted for early expansion of Medicaid eligibility have been able to enroll if they met the criteria for their state's expansion.
2.4. Medicaid-Covered Health Services
As described in Chapter 1, Medicaid is implemented through partnerships between states and the Federal Government. Each state must develop a Medicaid state plan that describes the health care benefits its program will provide. The plan and plan amendments must be approved by the HHS Centers for Medicare and Medicaid Services (CMS).
We include a discussion of covered services in this chapter on eligibility because it is easy to confuse eligibility for Medicaid per se with eligibility for the types of services most useful and important to people who are or have been chronically homeless. These include services and supports that can be delivered in a person's home or in other settings outside of an office, clinic, or treatment program, as well as case management and care coordination services. Not all Medicaid beneficiaries qualify to receive these types of services. Later chapters, which focus specifically on these types of services, describe the eligibility criteria for receiving them, which are established in terms of medical necessity.
Federal law and CMS regulations prescribe a set of core benefits that each state must include in its Medicaid state plan.15 States may decide to cover additional optional services and may limit eligibility for additional services to specific groups of people.16 Medicaid state plan provisions specify many program details, including provider qualifications, definitions of covered services, target populations, criteria of medical necessity for each specific service, and payment mechanisms for covered benefits. States must obtain CMS approval for optional services and other program details through state plan amendments.
While the expanded eligibility discussed above (Section 2.2.1) is a hugely important change affecting many poor people, including those experiencing homelessness, it is important to recognize that the types of care available through Medicaid may differ depending on certain characteristics of the beneficiaries. Both the basis for enrollment (categorical or income) and the health conditions of the beneficiary will affect eligibility for specific Medicaid-covered services.
In the post-2014 environment we can distinguish two general configurations of covered services, which are described below:
Medicaid State Plan: This is the array of services that anyone qualifying for Medicaid on a categorical basis would be able to receive. Federal law and CMS regulations stipulate the benefits a state must provide (mandatory benefits) and also allow states to cover a number of optional benefits (see footnote 16 and footnote 17).
Alternative Benefit Plans: This is the basic array of covered services that states must provide to the expansion population (those who qualify based on income alone). These plans may be different than the Medicaid state plan, with states defining benchmark coverage, but plans must include the essential health benefits specified by the Affordable Care Act.17 In 2014, many states have established Alternative Benefit Plans based on their Medicaid state plan, offering the same services that are offered in the state including long-term (nursing home) care.
The Affordable Care Act stipulates that the "essential health benefits" offered by Alternative Benefit Plans must include treatment services for mental health and substance use disorders, as well as rehabilitation and "habilitative" services and devices.18 Behavioral health treatment cannot be more limited than treatment for physical conditions. Because of these "parity" requirements, an Alternative Benefit Plan might offer better coverage for treatment of substance use disorders than the state's Medicaid state plan but less coverage for some of the types of mental health services covered through other current mechanisms, such as optional rehabilitative services option or waiver programs.19
While federal rules describe the minimum set of benefits that must be provided through Alternative Benefit Plans, states also have some flexibility to cover a more robust package of benefits tailored to the particular needs of population subgroups.20 A package of tailored benefits could potentially be designed to meet the needs of people with histories of chronic conditions that may contribute to chronic homelessness. States will determine the design of benefit plans available to people who become eligible for Medicaid in 2014, and states will decide whether Medicaid will cover many of the services that are most often delivered in PSH models. States will also decide on the provider qualifications required for Medicaid reimbursement. As shown in Exhibit 2.2, the five case study sites that have gone forward with expansion have established Alternative Benefit Plans that are equal to the Medicaid state plan with no exclusions. Some states that are going forward with expansion are adopting more limited Alternative Benefit Plans.
EXHIBIT 2.2. Alternative Benefit Plans of the Six Case Study Sites
| State | Alternative Benefit Plan |
|---|---|
| California | Medicaid state plan |
| Connecticut | Medicaid state plan |
| District of Columbia | Medicaid state plan |
| Illinois | Medicaid state plan |
| Louisiana | Not going forward at this time |
| Minnesota | Medicaid state plan |
2.4.1. Who Can Get What?
Medicaid is fundamentally a benefit program that provides health care coverage in much the same way that private health insurance programs do. Some services may be available to everyone, such as physical exams, but most services will only be provided if the beneficiary's health condition justifies them. Thus, only people with advanced heart disease will get heart surgery and only pregnant women will get prenatal care.
Most chronically homeless people and those living in PSH who reside in states that implemented expansion became newly eligible for Medicaid in 2014 on the basis of income. Once enrolled in Medicaid, they will qualify for their state's Alternative Benefit Plan. Most states have chosen to enroll the expansion population in Alternative Benefit Plans that are based on the state's approved Medicaid state plan.
Several subsequent chapters describe in detail the services that are particularly important for people experiencing chronic homelessness or living in PSH. Chapter 5 discusses mental/behavioral health services, and Chapter 7 examines emerging models of care coordination. In addition to describing our findings with respect to the services themselves, each of these chapters also discusses the medical necessity criteria that an individual would have to meet to be eligible to receive the services.
2.5. Outreach and Enrollment Strategies: Challenges and Solutions
When any new public benefit becomes available, it takes time for people to understand what it offers and how its provisions apply to them. All potential beneficiaries of new or expanded programs have this problem, which they often share with case managers and others who have the responsibility of helping newly eligible people to access all of the benefits for which they qualify. Medicaid eligibility expansion is no exception.
States that have expanded Medicaid eligibility through early implementation of the Affordable Care Act or provided Medicaid-financed coverage through waivers have developed many useful strategies to disseminate information about eligibility and stimulate interest among newly eligible people in the opportunities that have become available to them.
Early outreach and enrollment efforts have generally started with people who are already receiving health care services from hospitals and clinics that have been using state or local funding, grants, or other resources to pay for services.
The six communities studied intensively for this report were pursuing various enrollment strategies, described below. These include finding and engaging the newly eligible people and helping them through the Medicaid enrollment processes, helping people qualify for SSI, and helping people avoid being dropped from Medicaid.
2.5.1. Strategies for Enrolling Newly Eligible Members
Whether expanded eligibility occurred through early implementation or 1115 waivers, jurisdictions faced the challenge of enrolling thousands of people as quickly as possible. Some of the strategies used in this process include the following:
Starting with people already enrolled in state-only health insurance programs.
Starting with people using health services and engaging them at the time of treatment at clinics and hospitals.
Hiring and training specialized staff to handle the volume and the potential complexities of enrollment, and to help people obtain documents needed to complete the enrollment process.
Going to streets, shelters, and other locations to engage and enroll people who were likely to be eligible but not already connected to care.
Using new technologies to enable completion of an application in one encounter.
Automatically enrolling people based on information and documentation previously submitted to the county or state to establish eligibility for other benefits.
Starting With Existing Enrollees and Those Using Health Services
All five of the case study sites that pursued either early implementation of income-based eligibility or expansion through 1115 waivers began recruiting new enrollees from among people already enrolled in state-only health insurance programs or people already using safety net providers. Recognizing that enrollment would depend on the full understanding and cooperation of personnel in the agencies in contact with patients, these states clearly articulated the new eligibility criteria, pursued major informational and training strategies for people serving the target population, established enrollment procedures and forms, clarified the differences between old eligibility criteria (in jurisdictions with stateonly programs) and the new, and updated websites and other access points.
These jurisdictions assumed from the start that one of the best ways to reach people was to tell them about the new program when they came in for treatment. New procedures were established at safety net provider clinics and hospitals, including Health Centers. In outpatient settings, patients were notified as they signed in for appointments or during walk-in times. In hospitals, they were contacted in the emergency department or, if admitted, once they were established in a bed.
Hospital staff was encouraged to identify the people they saw most often and whose use of health care could become more rational and effective if they received proper case management. Special attention was focused on bringing these frequent users not only into Medicaid or the waiver plan, but also into case management and, if appropriate, housing. In Los Angeles, hospital staff reported almost immediate declines in hospital use after people in this group were connected with care and housing, which made them increasingly enthusiastic participants in strategies to engage this population.
Hiring Additional Staff and Focusing Them Solely on Enrollment
Health Centers in case study sites described the lengths they went to help their patients get enrolled into newly available coverage. Many hired staff for the sole purpose of processing applications and helping people get identification cards and other documents needed to establish eligibility. They then set up intake procedures at their appointment desk to refer all people coming in for care to the enrollment specialists first, before going to their medical appointment. The enrollment staff received specialized training in eligibility requirements and enrollment procedures. Many other safety net providers took similar steps to get people enrolled and connected to a primary care provider.
Going to the Streets and Using New Technologies
An important strategy for finding people who did not make frequent use of health care facilities was outreach to the streets. This strategy is important for addressing two barriers that often keep people experiencing chronic homelessness from enrolling in programs to which they are entitled--trust and difficulty navigating application processes. People experiencing chronic homelessness often have had negative interactions with public and safety net agencies, including health care providers, and have chosen largely to avoid them. Street outreach teams often include people who have had extensive contact with the people they want to enroll and have established a level of trust that makes it possible to start a conversation about enrollment.
Mobile technology can help turn those conversations into completed applications. The most successful outreach teams use mobile devices that allow them to connect to application websites wirelessly. They visit meal sites, shelters, and street locations, "going where they are" to work with people to establish eligibility "on the spot," preferably within the same single encounter as finding people again can be a challenge. Team members can complete an application on-line while talking to the applicant, photograph and convey documents (e.g., Social Security card, birth certificate) and an image of the applicant, get needed signatures on their mobile devices, and so on. These strategies have proved to be successful in enrolling some of the hardest-to-find eligible people.
Auto-Enrollment
Los Angeles County pursued an auto-enrollment strategy for newly eligible people to be covered through Healthy Way LA, basing eligibility on information and documentation that had been submitted when applying for other benefits. This information, which included documentation of residency, citizenship, age, and income, could be used to verify eligibility for coverage through the waiver program. The County also auto-enrolled people who were on the General Relief rolls into Healthy Way LA. Through autoenrollment, many people who were experiencing homelessness obtained coverage. However, enrollment alone did not connect people to health care, because many people did not know they had been enrolled into Healthy Way LA and did not know they had been assigned to a primary care provider or clinic. Their care-seeking behavior did not change until they connected in person with an outreach worker or with someone at a clinic or hospital. Funding from local foundations allowed the County Department of Health Services and several Health Centers to add outreach workers and case managers who actively worked to enroll people experiencing homelessness into coverage through Healthy Way LA and Medicaid, and to get those who were enrolled connected to a primary care provider or clinic that would best meet their needs.
After January 1, 2014, both case study sites that used 1115 authority to expand coverage automatically transitioned eligible beneficiaries from their waiver programs (Healthy Way LA and CountyCare) into enrollment in the state's traditional Medicaid program with full access to the entire Medicaid state plan. In the transition, most participants were assigned to a primary care provider and Medicaid managed care plan based on information about each person's primary care assignment and service use through the waiver program.
In 2014, California also implemented "Express Lane" enrollment into Medicaid for people receiving benefits through the Supplemental Nutrition Assistance Program (SNAP, formerly food stamps). This process uses the information provided by applicants for SNAP benefits to determine eligibility for Medicaid enrollment, without the need to complete a new application or submit additional documents.21
2.5.2. SSI Eligibility
Even in states that implement the expansion of Medicaid eligibility permitted under the Affordable Care Act, enrolling people who are chronically homeless in Supplemental Security Income will continue to be important. The categorical eligibility for Medicaid that comes with enrollment in SSI may provide access to a broader array of services available in a Medicaid state plan than in the benefit package available under an Alternative Benefit Plan. Access to full Medicaid state plan benefits can help cover more of the costs that PSH providers incur for the care they offer clients who are currently or formerly homeless. In addition, SSI provides these clients with a reliable income source to help pay for rent and other essential items.
There are, however, many barriers to qualifying for SSI, so it is very important for people experiencing chronic homelessness or those already living in PSH who are not yet enrolled in SSI to work with knowledgeable people who can guide them through the process. Applicants must document that their disability meets requirements of the Social Security Administration's (SSA's) requirements for diagnosis type, duration, and severity or functional impairment. As the process can be long and complicated, very few applicants experiencing chronic homelessness are approved on their first application attempt unless they have support from well-trained case managers, legal assistance, or help from other advocates.22
The case study sites examined in this study used a number of strategies to support SSI outreach and enrollment in SSI.
In Louisiana, persons displaced by Hurricanes Katrina and Rita in 2005 and other more recent hurricanes could gain access to federally funded PSH services. The source of these funds was timelimited disaster-related Community Development Block Grant funding. Beginning in 2008, the state's Permanent Supportive Housing Program (PSHP) used its homeless outreach teams to facilitate SSI enrollment for its clients. In PSHP, clients are assigned to the community support teams, so the issue of finding clients has not been as acute as in some other communities. PSHP caseworkers did have to work on engaging those clients, helping them understand the importance of obtaining SSI, and assisting them in obtaining documentation, completing the application, and continuing to pursue enrollment when an initial application was denied, which happened frequently. In cases where clients once had been SSI beneficiaries but enrollment had lapsed, sometimes for many years, PSHP staff helped with reinstatement. By 2011, at least 80 percent of current PSHP clients were SSI recipients and thus qualified for Medicaid, up from no more than 25 percent at the time the program was initiated.
In Los Angeles, the county-funded B.E.S.T. program, housed at JWCH's Center for Community Health (a Health Center), has achieved excellent results in helping people establish eligibility for SSI. On average, B.E.S.T. clients are approved for SSI within four months of enrollment in B.E.S.T., and more than 90 percent are approved with their first application. B.E.S.T. attributes its success to experienced staff who have support from upper management, do whatever it takes for clients, have excellent relationships with local SSA offices, and have highly developed and efficient records retrieval and standardized forms and procedures. In addition, the program focuses on clients who are likely to be approved; the program takes fewer than 20 percent of the people it screens, but is able to help almost all of its participants obtain SSI. Such screening is fairly common among agencies that work with clients to establish SSI eligibility since this is the most efficient way to deploy their specialized knowledge.
In the District of Columbia, the Medicaid enrollment process (both before and after expansion) includes a screen for homelessness and disability. Enrollment staff are expected to refer someone who is experiencing homelessness or is highly likely to be found disabled to Interim Disability Assistance (IDA), a special section within the department that assesses them for likely SSI eligibility. If SSI eligibility is likely, the person is enrolled in IDA while applying independently for SSI. IDA staff help the applicant to assemble the documentation needed for IDA eligibility. IDA pays a monthly stipend as well as qualifying the applicant for full fee-for-service Medicaid. IDA stops as soon as SSI receipt is approved. With SSI, full fee-for-service Medicaid continues.
If a person experiencing homelessness already has a caseworker from any of several agencies, that caseworker will assist with this process. The contracts for case management in its PSHP (see below) include the requirement that caseworkers assist with IDA/SSI applications. All of these caseworkers are trained in the HHS Substance Abuse and mental health Services Administration's (SAMHSA's) SSI/SSDI Outreach, Access and Recovery (SOAR) techniques, which staff say has helped facilitate access to IDA/SSI.23 In previous years, the Los Angeles County Department of Health Services (DHS) recovered between $2.3 and $2.4 million in health care costs from Medicaid; since the SOAR training, that amount increased to $3.5 million in 2011 and was expected to go up even further for 2012.
For more information on these and other examples of strategies for improving access to SSI for homeless and formerly homeless people, see Burt and Wilkins 2012b.
2.5.3. Maintaining Medicaid Enrollment Over Time
Organizations intending to provide comprehensive and coordinated care for populations with complex health conditions usually make financial calculations based on a set of assumptions. One essential assumption is that once someone is enrolled in Medicaid, that individual will remain enrolled and the provider can count on receiving a given amount of money from Medicaid every month to cover the cost of care.
Provider experiences during the first year or two of operating in the new mode has shown that this assumption is not borne out by reality. An important but not initially fully appreciated reason is the attitudes and care-seeking habits of the newly eligible population. Many newly enrolled beneficiaries have never had health insurance, and have difficulty understanding the need to maintain coverage when they do not need care. They are accustomed to going to the doctor, emergency room, or hospital when they are sick, usually very sick as they wait too long to seek care, and do not see why they should worry about maintaining insurance coverage when they can always get re-enrolled on the spot when they need care again.
Thus enrolling people in Medicaid is only the first challenge; keeping them enrolled can be equally challenging. Some providers reported that almost as many patients drop off their rolls every month, due to loss of Medicaid eligibility attributable to difficulties with recertification, as they are able to enroll. Before full implementation of the Affordable Care Act, states often required their beneficiaries to re-establish eligibility every six months, and sometimes more often.24 Beneficiaries had to submit paperwork to document their continued eligibility. In recent years, state policymakers in several of the case study sites enacted requirements for frequent eligibility redetermination as a strategy for achieving budget savings. If beneficiaries did not submit the paperwork on time they were dropped from Medicaid and had to go through a full reapplication process to get reinstated. These requirements are quite difficult for people experiencing homelessness to comply with, putting them at great risk of losing eligibility not only because they have more difficulty assembling the documentation required, but also because their unstable housing situations mean they may not receive reminders of pending deadlines.
For example, people experiencing homelessness often face gaps in eligibility for California's Medicaid program because they do not receive notifications or are unable to complete the paperwork required to maintain their enrollment. Service providers find it difficult to communicate with the county and the state to verify that the people they serve are currently enrolled in Medicaid, and county and state records have been known to differ.
Because Medicaid providers may experience disallowances if they bill for services delivered while a client is off the rolls, they invest considerable staff time in verifying enrollment and documenting eligibility.
Hennepin County, Minnesota, is one case study site finding that its assumptions about stable enrollment have not been borne out. Hennepin County is developing an Accountable Care Organization called Hennepin Health, which began enrolling people who were newly eligible for Medicaid shortly after Minnesota implemented its early expansion of income-based Medicaid eligibility in March 2011.
Hennepin Health has faced challenges maintaining and increasing the number of people enrolled in the plan because many people lose coverage when they fail to submit their eligibility paperwork every six months. In December 2012, enrollment stood at 6,000 people. Although the plan enrolls about 1,000 members every month, it also loses 800 members whose coverage is dropped because they have not submitted the required documentation.
The State of Minnesota recently approved a process for sharing eligibility redetermination dates with Hennepin County, but in December 2012, Hennepin Health was still working with paper lists. Staff hope to integrate the information about eligibility redetermination dates into state data systems so that clinic workers can monitor upcoming deadlines and encourage clients to submit required documentation on time. This could include providing reminders when patients visit the clinic or contacting members whose eligibility ends.
Hennepin Health contracted with a vendor to track and facilitate eligibility redeterminations, but this did not have a significant impact on reducing the rate at which members lost coverage. Hennepin Health has found that many of the very low-income adults enrolled in the plan had not established strong connections to primary care providers in the past, instead relying on emergency rooms for care when needed. It is taking time and ongoing efforts to help previously uninsured adults build relationships with care providers and recognize the value of having year-round coverage with ongoing access to a primary care provider.
Minnesota's broader experience with enrollment churning in the Medicaid expansion population has been similar to the experience with plan enrollment at Hennepin Health. However, state agency staff expect that changes in 2014 will reduce churning. Factors such as simplifying eligibility and income verification and a change from 6 months to 12 months for redetermination should significantly reduce the number of people who lose eligibility or experience gaps in enrollment.
2.5.4. Shifts to Managed Care Enrollment
In some of the case study sites, the state Medicaid program is requiring that recipients be enrolled in a Medicaid managed care plan. This reflects a nationwide trend. In 2012, the Kaiser Family Foundation reported that more than half of all Medicaid beneficiaries were already enrolled in managed care plans.25 Until recently, seniors and people with disabilities were less likely to be enrolled in managed care arrangements than children and their parents, but an increasing number of states are expanding mandatory managed care enrollment to include people in this group. States are likely to use Medicaid managed care plans to provide coverage to people who are newly eligible for Medicaid. When the District of Columbia established income-based eligibility in April 2010, for example, it assigned all new Medicaid beneficiaries to a managed care plan. Those who had been enrolled in its self-financed health insurance program (Alliance Health Care) were assigned to one health plan (United), and all other enrollees were assigned to either United or another health plan (Chartered).
Enrolling people with histories of homelessness and complex needs has posed challenges for managed care plans. For example, the enrollment process often requires that Medicaid beneficiaries select a managed care plan from among two or more choices and designate a primary care provider, or get assigned by default if they do not make a choice. The selection of (or assignment to) a plan and provider usually limits where people can receive Medicaid-reimbursed health care services, or which providers can get reimbursed if they deliver care. These issues are discussed in more detail in Chapter 6.
2.6. Summary
Many of the challenges that people experiencing homelessness, living in PSH, and other people with extremely low incomes had with enrolling in Medicaid were lessened after full implementation of the Affordable Care Act in 2014. On January 1, 2014, individuals with incomes lower than 133 percent of the federal poverty level, including those who are or were experiencing homelessness, became eligible for Medicaid for the first time on the basis of income in 25 states and the District of Columbia. About 64 percent of people experiencing homelessness reside in the states currently going forward with expanded eligibility (HUD 2012, p.5), increasing the likelihood that people experiencing homelessness or living in PSH will be able to access the services they need. A high percentage of people experiencing chronic homelessness have a serious mental illness, usually coupled with co-occurring behavioral and physical health conditions. Alternative Benefit Plans, in which they are likely to be enrolled, include behavioral health services as part of the essential benefits required by the Affordable Care Act, which will make these services available for the first time to many of the new beneficiaries. Further, streamlining of eligibility determination and recertification should make enrollment easier and greatly simplify maintaining eligibility, which should reduce the problem of enrollment churning. Reaching and engaging people experiencing homelessness or living in PSH and keeping them enrolled will always be challenging, but new options for covering the costs of care coordination under the Affordable Care Act, plus increased provider experience over time, should begin to address these issues. Given the importance of Medicaid coverage for people with complex health and behavioral health conditions, the changes evolving under the Affordable Care Act show the promise of bringing more people into care, providing more appropriate and coordinated care, and helping them remain in care.
3. Using Medicaid Waivers to Expand Coverage
Chapter 3 Highlights
Some states have used Medicaid waivers authorized under Section 1115 of the Social Security Act to expand health coverage for low-income people, which gives them the ability to reach many people experiencing homelessness or who were once homeless and now live in PSH.
Among case study sites, California and Illinois used 1115 waivers as a "bridge to reform," helping them establish low-income health plans in advance of 2014 that offered access to health care for many people who became eligible for Medicaid upon full implementation of the Affordable Care Act.
Under these waivers, jurisdictions receive federal Medicaid funds to match state and county spending on health care services delivered to qualifying low-income people.
As many people who enrolled in the health plans developed under the waivers had previously had no insurance and were being served at county facilities as uncompensated care patients, the availability of the federal match freed up some county funds for reassignment to other uses. These funds have helped many of the safety net hospitals and other health care providers to prepare for service, billing, and payment systems that needed to be in place for 2014.
Under California's 1115 waiver, each county could establish a low-income health plan, which in Los Angeles is called Healthy Way LA. Providers include the county's own extensive network of hospitals and clinics, plus Health Centers that operate as community partners under contract to the county. During its first year, 2012, Healthy Way LA enrolled almost 200,000 people, and enrolled almost 100,000 more by the end of 2013.
The Illinois waiver was approved more than a year after California's and applied only to Cook County. Enrollment began late in 2012, giving Cook County only a year to expand enrollment through the low-income health plan it developed, called CountyCare. In addition to the county's own health and hospital system facilities, CountyCare partners with Health Centers to serve as primary care providers for many CountyCare members, as required by the waiver.
Most of the people enrolled in the health programs developed under the California and Illinois waivers were automatically switched over to Medicaid enrollment on January 1, 2014.
3.1. Introduction
As described in the previous chapter, some states have used Medicaid waivers authorized under Section 1115 of the Social Security Act to expand health coverage for low-income people, and that expansion has been able to reach many people experiencing homelessness or who were formerly homeless. Section 1115 authorizes demonstration programs, which give states flexibility to test approaches to financing and delivering health care services while sharing costs with the Federal Government through the Medicaid program. These waivers must be budget neutral to the federal Medicaid program, meaning that the waiver programs, over a five-year period, must result in less federal expenditure than if the demonstration program were not implemented. Often the expansion of mandatory enrollment of other current Medicaid beneficiaries into managed care plans is a state strategy for achieving savings. Chapter 6 takes a closer look at these managed care strategies.
Coverage expansion programs approved since the enactment of the Affordable Care Act were often intended to provide a "bridge to reform," meaning that the program offered an opportunity to provide some form of coverage and access to health care for many people who would become eligible for Medicaid enrollment in January 2014 in states that chose to implement the Affordable Care Act's incomebased eligibility expansion. While the specific provisions of each state's Medicaid waiver differed in important ways, often the same income limit was used to define eligibility under the waiver.
The eligibility criteria, enrollment process, and benefits package specified in the terms of a state's Medicaid waiver for newly eligible program participants could differ in some ways from that of the state's Medicaid program for people who are categorically eligible. For example, people eligible for enrollment through the waiver could have been limited to a smaller network of hospitals and other health care providers than were available to the entire Medicaid population. To put this differently, jurisdictions operating under the 1115 waiver selected a limited number of hospitals and health care providers that could receive Medicaid reimbursement for care they provided to people enrolled under the waiver. Providers participating in the waiver usually included county hospitals and clinics and other community clinics and teaching hospitals affiliated with county health departments that were part of the health care "safety net." Those providers serve a disproportionately large number of indigent and uninsured patients, which is the population these 1115 waivers were designed to reach.
As noted in Chapter 2, two case study communities, Los Angeles and Cook counties, used waivers to expand coverage. In 2011, under the terms of California's 1115 waiver allowing its counties to develop such plans, Los Angeles County established a Low Income Health Program, Healthy Way LA. To expand Medicaid coverage to uninsured low-income adults in Cook County starting in January 2013, the state of Illinois received approval in late 2012 for a similar 1115 waiver targeted specifically to Cook County/Chicago.
3.2. Building Safety Net Capacity
In addition to providing coverage for health benefits for many uninsured low-income people who would not otherwise qualify for Medicaid until 2014, the waivers expanded the base of financing for providers who are part of the health care safety net. This financing took the form of federal Medicaid funds that match state and county spending on health care services delivered to qualifying low-income people.
This new source of financing offered short-term help to some hospitals and other safety net health care providers at a time when state and local budgets were severely strained by the combination of declining tax revenues and rising demands for free or low-cost health care as a result of the recession. Perhaps more important, the payment mechanisms established through the waivers helped many of these hospitals and other health care providers prepare for the billing and payment systems they would need to have in place by 2014, when many of their currently uninsured patients would become eligible for Medicaid enrollment or for subsidized health insurance under the Affordable Care Act.
To reinforce the role of the waivers in building safety net capacity as a "bridge to reform," the waiver terms often required that newly covered patients receive many of the benefits that are generally associated with health insurance coverage. This often included assignment to a primary care provider to allow some level of trust and mutual knowledge to develop, to assure some level of care continuity, and to improve timely access to care.
Safety net health care providers face both opportunities and risks with full implementation of coverage expansions and other reform provisions of the Affordable Care Act. Many public hospitals and clinics serving people experiencing homelessness have relied on public funding through state or county budget appropriations and grants to cover the costs of serving these patients, who have typically lacked insurance in the past. These hospitals may also serve Medicaid beneficiaries and have systems in place for seeking Medicaid reimbursement, but it is likely that some safety net providers that deliver health care to indigent patients will have to augment existing systems. In addition, as states are most likely to place the newly eligible population into managed care, including most or all people who are or were experiencing homelessness, providers serving these populations may face the need to make substantial investments in administrative systems to support billing insurance companies, contracting with managed care plans, or obtaining Medicaid reimbursement on a fee-for-service basis as their patients obtain coverage through Medicaid or other insurance in 2014.
Another challenge to safety net health care providers is retaining their patient base when currently uninsured patients have a broader range of choices starting in 2014. Hospitals, clinics, and other safety net providers recognize that they will need to make improvements to become "providers of choice." If many newly insured patients choose to go elsewhere for care, some health care providers will find themselves in even worse financial shape, with continued responsibility for serving patients who remain uninsured and those who are too troubled or disabled to navigate other available options. These remaining patients will be more expensive to serve on average, and sources of funding for indigent, uninsured patients are likely to be reduced.
All of these changes are significant for both patients and the health care providers and systems that deliver health care services to low-income people. Los Angeles County's experience implementing its Low Income Health Program, Healthy Way LA, highlights some of the challenges and lessons learned during coverage expansion. In Cook County, Illinois, planning and start-up activities for CountyCare were just getting under way during our final visit to that community in December 2012. Leaders in this process were anticipating making some significant changes in Cook County's health care delivery system during 2013.
3.3. California's Waiver
California's "Bridge to Reform" 1115 waiver authorized counties to create Low Income Health Programs (LIHPs) to prepare for the expansion of health coverage in 2014 under the Affordable Care Act. The waiver allowed each California county to decide whether to establish an LIHP, and most counties chose to do so.26 California's counties were responsible for providing or paying for basic health care services to indigent, uninsured residents and also for paying the nonfederal share of costs for the LIHPs. Counties had significant flexibility in setting eligibility criteria for LIHP enrollment. Some counties set enrollment caps (with waiting lists for enrollment); others limited eligibility to people with extremely low incomes (as low as 25 percent of the federal poverty level); and still others made LIHP enrollment available to anyone who would become eligible for Medicaid in 2014.27 Counties had to provide a minimum set of covered benefits and meet specified standards for providing access to care for enrolled patients. These standards were intended to move county health care delivery systems for indigent patients toward readiness to deliver care through managed care arrangements in 2014.
3.3.1. Expanding Coverage Through Healthy Way LA
Healthy Way LA, the Low Income Health Program established by the Los Angeles Department of Health Services under the state's 1115 waiver, had two components. The first, called the "matched" program, was for people who met the eligibility criteria established under the waiver for the county to receive Medicaid funding to match its own investment of general funds to pay the cost of care. The second component ("unmatched") provided care for people who remained uninsured because they did not meet eligibility requirements related to citizenship or length of permanent residency. This component was 100 percent county-funded.
Healthy Way LA covered both health care services delivered through the Department of Health Services' county hospitals and clinics and through a network of contracted community partner clinics that provide outpatient services.28 Healthy Way LA also provided coverage for some mental health services.
The county's share of mental health costs is provided by the Los Angeles County Department of Mental Health. Mental Health services were delivered to Healthy Way LA members through providers that are part of the county mental health system. County LIHPs were not required to cover substance use disorder services under the California waiver, and Healthy Way LA did not do so.29
Starting in 2011, coverage for uninsured people in Los Angeles County through enrollment in Healthy Way LA expanded rapidly. The county had earlier set a conservative enrollment target because of concerns about the availability of county funding to match federal reimbursement. In 2011 a new director of the Los Angeles Department of Health Services persuaded the county not to cap enrollment and instead to make an aggressive push to enroll all indigent people who were patients of Department of Health Services' hospitals, clinics, and community partner clinics. Full enrollment meant that the department would receive federal Medicaid funds to match county spending. The department launched Operation Full Enrollment in July 2011. Enrollment in the Healthy Way LA matched program expanded to more than 200,000 patients by the end of 2012--more than half of the Los Angeles County residents who became newly eligible for Medicaid (Medi-Cal) in 2014. By the end of 2013, enrollment was nearing 300,000.
With eligibility expansion for Medicaid in 2014, financing was expected to shift in ways that could change the incentives facing the Department of Health Services and its partners. The approach active under the 1115 waiver involved using county spending (certified public expenditures) for health care and mental health services provided to Healthy Way LA members to obtain matching federal funds. Therefore, the department had few incentives to enroll people who were not already receiving or seeking health care from providers who are part of the Healthy Way LA provider network.
Beginning in 2014, however, newly eligible people, including those transitioning from Healthy Way LA to Medicaid (Medi-Cal), are being enrolled into managed care plans, and Medicaid financing for the plans is in the form of capitated, per-member per-month payments.30 In Los Angeles, the managed care health plans make capitated per-member per-month payments to the Department of Health Services for all members who have been assigned to one of the department's clinics for primary care. Anticipating this change, the Department of Health Services began pushing to enroll into Healthy Way LA many more of the eligible people who were not currently receiving care from department facilities or contract agencies, and added another 100,000 members by the end of 2013.
3.3.2. Changes in the Health Care System
The terms of California's 1115 waiver required Healthy Way LA to provide enrollees with timely access to primary care and other covered services. This requirement was intended to ensure that each LIHP would provide meaningful coverage for its members, rather than being only a mechanism to draw down federal match funding.
This statewide requirement was bolstered by Los Angeles County officials' recognition that the county health care delivery system needed major improvements to be ready for the opportunities and risks coming in 2014 with the shift to managed care financing.
Leaders at the Department of Health Services and its community partners hoped that significant changes in its hospitals, clinics, and other programs would induce patients who enrolled through Healthy Way LA to stay with their health care providers after their enrollment in Medicaid gives them other choices.
Providing better, more personalized care was one of Healthy Way LA's most significant changes. People who enrolled in Healthy Way LA were empaneled, meaning that they were assigned to a designated primary care provider or medical home at a county clinic or community partner clinic. Healthy Way members got priority for scheduling clinic appointments at their designated medical home, while people who had not enrolled in Healthy Way LA could still spend hours in crowded waiting rooms to get urgent care. Department of Health Services' clinicians were expected to serve a panel of enrolled Healthy Way LA patients. In addition, many of the physicians with administrative jobs in the department began spending at least part of their time delivering primary care. Patients began to see the same doctor or medical team each time they sought care--a situation that continues in the 2014 environment.
Electronic health records were another major focus. The Department of Health Services and its community partner clinics began working to develop and implement electronic health records and patient registries to better manage chronic illnesses. Efforts also began to better coordinate electronic data systems to facilitate information sharing among the county's hospitals and clinics. Electronic records and tools, such as patient registries, were expected to make it easier for providers to see a client's case history, medications, and other information needed to help the provider prepare for a visit and proactively manage all aspects of a client's care. It was expected that the data would also be used for quality assurance and outcome measurement.
These changes began significantly improving services in ways that benefit people experiencing homelessness or living in PSH. The county and community clinics that serve many people experiencing homelessness made substantial investments during 2011 and 2012 in helping them get enrolled into Healthy Way LA and connected to a primary care provider. These efforts continued in 2013 with additional support from philanthropy, including grants from the Conrad N. Hilton and Unihealth foundations.
During 2011 and much of 2012, the rapid increase in applications for enrollment in Healthy Way LA created significant backlogs in the county's processing systems. Requirements for applicants to submit documentation of citizenship or legal residency status contributed significantly to enrollment barriers and delays in application processing. Community partner clinics, including clinics that serve many patients experiencing homelessness and PSH residents, encountered major enrollment challenges. Thousands of applications submitted by clinics were stalled, creating significant cash flow problems for some clinics.31 By late 2012, application backlogs were finally being reduced and the clinics were receiving more of the revenues that had been promised for enrolling and serving Healthy Way LA members.
As one of the ways to improve the health care system, the Department of Health Services would like to create a more robust approach to providing home health services, particularly for people with complex medical and behavioral health needs. Whether these services can be Medicaid-reimbursed depends on whether California pursues an amendment to the Medicaid state plan to offer optional home health services authorized by the Affordable Care Act.
Department of Health Services' hospitals also have renewed their focus on reducing avoidable hospital admissions and shortening patient lengths of stay. The county hospital system has been widely perceived to be inefficient. Despite years of effort to switch access to care to outpatient settings, many people are admitted for unnecessary hospital stays. Furthermore, homeless patients often stay in the hospital longer than would be needed if better options for care were available upon their release. The department's leaders believe they can make significant improvements in the quality of health care if they can use the system's capacity more efficiently, moving resources around to achieve savings and provide better options for people who do not really need to be in a hospital or nursing home.
Changes for Previously Uninsured People
Being included in a health care insurance program under California's 1115 waiver is a big change for uninsured people who have been receiving care from the health care safety net. Uninsured people with extremely low incomes and no insurance coverage seek care only when they need it, and often later than desirable, when they are sicker. They often rely on hospital emergency rooms because they do not have an ongoing connection to a regular source of primary care. The tasks associated with enrolling in coverage, selecting and having an ongoing connection to a primary care provider, and following up to maintain coverage when required to submit paperwork to verify continued eligibility may be unfamiliar or a low priority for a person who is experiencing homelessness.
Despite the efforts of the Department of Health Services to expand coverage, individuals accustomed to relying on free clinics or uncompensated charity care in hospitals may have been reluctant to enroll in Healthy Way LA, expecting that they would still have access to free or low-cost care when they needed it. The resulting gaps in coverage disrupt both continuity of care for patients and payments for care providers. The department and its partner clinics put a lot of effort into working with patients to ensure that they would not only enroll in Healthy Way LA but also comply with requirements to submit the documentation needed to verify their continued eligibility for enrollment.32
To reach and serve more people who are homeless in LA, the Department of Health Services is opening a clinic in Skid Row, where the county already contracts with two community partner clinics, JWCH and LA Christian Health Center. The new clinic is located in a storefront on the ground floor of a new PSH project, the Star Apartments, developed by the Skid Row Housing Trust.
The two existing Skid Row clinics already serve hundreds of people experiencing homelessness, but the Department of Health Services believes there is a need for a county clinic because many of the patients who are homeless and who visit the emergency room at the nearby LA County University of Southern California hospital are not connected to ongoing care at JWCH or LA Christian Health Center. Department leaders also believe that planning and implementing service delivery at a clinic located in a PSH site (the Star Apartments) will give them a better understanding of some of the challenges facing the other clinics in the Skid Row area. This will help to drive decisions about what the county is willing to pay its partners to deliver care.
One goal of the county's new Skid Row clinic is to better connect patients experiencing homelessness to ongoing health care so they will come to the clinic instead of going to the hospital emergency room. The Department of Health Services' clinic, which opened in June 2013, serves as a hub for providing services to formerly homeless tenants who live in nearby PSH. It provides a base for nurses and other clinic staff who can deliver care through home visits to PSH tenants, and also for street outreach in the Skid Row area. Team models are being used to make care available in a convenient and accessible way. Team members "walk the streets of Skid Row" to establish ongoing, face-to-face connections with people needing care and other providers the community.
The department is also working to implement an e-consult system to provide much more timely access to consultation by a specialist, often while a patient is at a visit with a primary care provider. Instead of offering a patient an appointment with a specialist, which might take weeks or months to get, the primary care provider can share information electronically with the specialist and get a speedy response. It may even be possible to use webcams for a videoconference involving the patient, primary care provider, and specialist or for the primary care provider to send a picture to the specialist. The primary care provider can get advice about how to manage the patient's care without the need for a visit to the specialist, or the information shared by the providers may support a decision to offer the patient an appointment with the specialist immediately to address an urgent condition. If the specialist determines that additional tests are needed, the patient can get them done before going to see the specialist. At the time of our final site visit, e-consult implementation was beginning with patients in the county jail, for whom arranging visits with health care specialists is often difficult and costly. The expansion of e-consult services to other LA Department of Health Services' clinics was planned for 2013.
3.4. CountyCare: Cook County's Approach to Expanding Coverage
Cook County, Illinois, is another community that used a Medicaid waiver as a "bridge to reform." At the end of October 2012, Illinois received federal approval for an 1115 waiver to use Medicaid financing to expand coverage through CountyCare, a program operated by the State of Illinois and the Cook County Health and Hospital System (CCHHS). CCHHS moved quickly to launch implementation in 2013.
CountyCare offered coverage to uninsured adults between the ages of 19 and 64 who had incomes below 133 percent of the federal poverty level, were United States citizens or had been permanent legal residents for more than five years, and were not otherwise eligible for coverage through Medicaid or Medicare. CountyCare intended to enroll people in 2013 who would became newly eligible for Medicaid in 2014.
Similar to Healthy Way LA, two major goals of CountyCare were to: (1) obtain Medicaid financing to match Cook County spending for inpatient and outpatient services provided by the hospitals and clinics that are part of CCHHS; and (2) help CCHHS make changes that would allow it to remain a viable part of the health care delivery system when many of its patients enrolled in Medicaid or subsidized health insurance coverage with Affordable Care Act implementation in 2014.
The terms of the waiver required CCHHS to partner with Health Centers (Federally Qualified Health Centers or FQHCs) to serve as primary care providers for many CountyCare members. Soon after the state's Medicaid waiver was approved, CCHHS selected 13 Health Center partners, including Heartland Health Outreach (Chicago's Health Care for the Homeless program) and other Health Centers that have been involved in serving people experiencing homelessness and PSH tenants. Selection criteria included the following:
The number of uninsured patients currently served by the Health Center.
Geographic location, with the goal of filling gaps not already covered by CCHHS clinics.
Experience serving particularly needy populations, including people experiencing homelessness and people with HIV/AIDS.
Some capacity to provide behavioral health services.
Capacity to offer pharmacy, wellness and nutrition, and other services.
The package of benefits available to CountyCare members included inpatient and outpatient hospital services, physician and clinic services, lab and X-ray, adult dental, subacute substance use disorder services, mental health, and targeted case management services, as well as other services including up to 30 days of nursing facility care after a hospitalization.33
The implementation of CountyCare was expected to strengthen connections between CCHHS and partnering Health Centers and other providers of community-based services for low-income uninsured people, including many people who are experiencing homelessness. Partner Health Centers collaborated with CCHHS to enroll eligible people in CountyCare, helping their patients complete the application and gathering and scanning copies of the required documentation (including proof of identity, citizenship or permanent residency status, income, and residency in Cook County). CCHHS established a web portal for partner Health Centers to submit applications for enrollment. CountyCare members were expected to have enhanced access to specialists who work in CCHHS hospitals and specialty care clinics. Coordination was expected to improve among those specialists and the Health Centers that are part of the CountyCare provider network.
Some of the leaders at CCHHS perceived that the success of CountyCare would depend in part upon building stronger partnerships to co-manage care for shared patients, particularly those who are homeless and have both medical and behavioral health needs that require integrated and coordinated care and connections to housing. Linkages to community-based providers of behavioral health services were seen as critical, but important decisions about how these services would be implemented as part of CountyCare were still pending at the time of our final visit.
CCHHS also expected to establish partnerships with other local hospitals to make them part of the CountyCare provider network. At the time of our final visit, discussions and initial negotiations with other hospitals were just getting under way, starting with the hospitals already serving many of the patients who receive care from the Health Centers selected as part of the CountyCare provider network. For CountyCare members, coverage for nonemergency hospital care was to be available only at network hospitals.
CCHHS provides health care services at the county jail, and early in 2013 it began enrolling eligible people in CountyCare as they prepared for discharge from jail. The expectation was that connecting people to CountyCare would facilitate continuity of care as they returned to the community, particularly for people with HIV/AIDS or other complex health care needs.
CCHHS also offers patients some assistance with applying for Supplemental Security Income (SSI) benefits. It uses a vendor to review information about people who enroll in CountyCare to determine whether they are potentially eligible for SSI. Health and Disability Advocates provides a social worker and lawyer at Cook County's Stroger Hospital to assist with SSI applications and appeals.
3.5. Summary
Our case study sites illustrate how Medicaid waivers have helped strengthen the health safety net and provide a bridge to reform. California and Illinois have 1115 waivers for coverage expansion (LIHP/Healthy Way LA, and CountyCare); both states used their waivers to expand care to previously uninsured people and strengthen the capacity of the health care system in advance of full implementation of the Affordable Care Act.
Under California's 1115 waiver and with support from philanthropy, Los Angeles County pursued aggressive enrollment targets for Health Way LA while building connections that are benefitting people who are homeless or living in PSH. By providing coverage that offered a "bridge to reform" for people who became eligible for Medicaid in January 2014, California's waiver gave the Department of Health Services matching federal funding for costs of care provided in county hospitals and clinics, and an opportunity to make investments in improving the quality and efficiency of health care in the safety net delivery system. As described later in this report (Chapter 7), this allowed the department to make investments in strategies to target housing to people with long histories of homelessness and high levels of vulnerability, as well as to decrease avoidable hospitalizations and crisis care.
Cook County, Illinois, is addressing the needs of uninsured people with a broad package of benefits and improved connections among Health Centers and other providers serving low-income people, including people experiencing homelessness.
In both states, providers hoped the efforts they were undertaking to connect people to providers would build client loyalty so clients will stay with those providers later, even if they have other choices for obtaining care.
4. Health Centers, Health CARE for the Homeless Programs and Federally Qualified Health Centers
Chapter 4 Highlights
Health Centers, including Health Care for the Homeless programs generally receive federal grants from HHS's Health Resources and Services Administration to provide comprehensive primary care and preventive services to low-income people in underserved communities. These Health Centers can also receive Medicaid reimbursements as Federally Qualified Health Centers. Among case study sites, FQHCs in Chicago, Los Angeles, and Washington are significant providers of health care and other services and supports to people with histories of chronic homelessness and to PSH tenants. They offer models of possible strategies that other communities could adopt.
Health Centers, including Health Care for the Homeless programs, face considerable changes as the Affordable Care Act moves into full implementation. Until 2014, over a third of their patients had no private or public insurance; many of the uninsured will now be Medicaid-eligible in states that expand Medicaid. The Affordable Care Act provided $11 billion in federal funding over five years to expand the Health Center program, with the goal of expanding access to health care services as more people in low-income communities obtain coverage. The volume of Health Center visits increased from 38 million in 2000 to 80 million in 2011, with more than one in six low-income people nationally receiving their care from these centers (Kaiser Commission 2013). Federal funding has expanded the number of Health Center medical staff, as well as staff who provide dental and mental health services.
Most patients of Health Care for the Homeless programs will become eligible for Medicaid coverage based on their low incomes if they live in states that expanded eligibility based on income in 2014. But barriers to Medicaid enrollment will likely persist for some people with histories of chronic homelessness because they lack reliable contact information or required identification documents, or find it difficult to navigate the application and eligibility determination process. In Los Angeles, PSH and homeless assistance providers have worked closely with Health Centers to help uninsured people access Health Center services and, if eligible, to enroll in Medicaid.
FQHCs are paid an "all-inclusive" rate for each visit a Medicaid patient makes with qualified staff. These pervisit rates often appear higher than Medicaid reimbursement fee-for-service rates paid to other types of providers who serve Medicaid beneficiaries, however, because the reimbursement is a bundled rate direct comparisons are not possible.
As many states increasingly rely on Medicaid managed care plans to provide health care for their beneficiaries, many Health Centers have joined these health plans' provider networks.
A growing number of Health Care for the Homeless programs and a few other Health Centers have developed programs to engage and provide ongoing health care and supportive services linked to permanent housing for people with histories of chronic homelessness. To do so they collaborate with numerous partners, including community-based mental health and housing support service providers and sometimes agencies providing rental assistance or PSH units.
Integration of primary and behavioral health care is an important goal, as is consideration of housing status and recognition of the importance of housing stability for health outcomes.
Best practices for serving people experiencing chronic homelessness or living in PSH often do not align with payment structures and requirements for FQHCs. Challenges include obtaining reimbursement for working "outside the four walls," offering "whatever it takes" wraparound services, using techniques such as motivational interviewing to address substance use issues, incorporating unlicensed staff such as peer support specialists into patient care teams, operating in a multidisciplinary team structure, and work aimed at assuring housing stability.
4.1. Introduction
Health Centers, including Health Care for the Homeless (HCH) Programs, generally receive federal grants from HHS's Health Resources and Services Administration (HRSA) to provide comprehensive primary care and preventive services to low-income people in underserved communities. These Health Centers generally also receive Medicaid and Medicare reimbursements as Federally Qualified Health Centers.34
In some case study communities, Health Centers are significant providers of health care and other services and supports to people with histories of chronic homelessness and to PSH tenants, often working in partnership with providers of mental health services and housing assistance. They offer models of possible strategies that other communities could adopt. For example:
In Chicago, Heartland Health Outreach (HHO) is a Health Care for the Homeless program with clinic, satellite, and outreach components, as well as a provider of PSH, mental health, and substance use disorder treatment, and an array of services for people who are homeless. HHO has developed innovative models of integrated care linked to housing for people who are chronically homeless, including Together4Health, an emerging Care Coordination Entity that we describe in more detail in Chapter 7.
In Los Angeles, JWCH operates the Center for Community Health, which integrates the delivery of primary care with dental, clinical pharmacy, mental health, and substance use services for people who are homeless in Skid Row. For more than a decade JWCH has been providing health services linked to housing for people experiencing chronic homelessness, and it operates part-time "satellite" centers in some PSH buildings. In the past few years, other Health Centers in LA County have gotten involved in PSH partnerships.
In the District of Columbia, Unity Health Care was founded as a Health Care for the Homeless program and operates as a Health Center serving low-income and underserved people and communities. Unity partners with Pathways to Housing DC to provide primary care services that are integrated with behavioral health services and linked to housing assistance for people who are homeless and have serious mental illness (SMI).
4.2. Understanding Health Centers and Federally Qualified Health Centers Medicaid Reimbursement
Nationwide, over 1,100 federally funded Health Centers served over 21 million patients in 2012.35 The majority of Health Center patients have incomes below the federal poverty level. Before 2014, more than one-third of Health Center patients were uninsured, and 40 percent of health center patients were Medicaid beneficiaries. Many patients who were uninsured were expected to qualify for Medicaid as of 2014 (if they live in states expanding coverage) or for federally subsidized insurance coverage through the exchanges.
While Health Centers play a large and important role delivering health care to millions of low-income people, and many Health Centers are now actively engaged in helping people enroll in coverage, they also face significant uncertainty about the ramifications of full implementation of the Affordable Care Act. In expansion states, many of their uninsured patients may gain coverage through Medicaid, and this will increase Medicaid revenues if these patients continue to receive care from the Health Centers. However, these patients are likely to have other choices about where to go for primary care when they gain coverage, and some may select other providers when they get the opportunity to do so. Health Centers are likely to continue to provide care for many people who will remain uninsured because of their immigration status, because of other barriers to enrollment and eligibility, or because they live in states that choose not to expand Medicaid eligibility. In addition, Health Centers' active role in helping people try to enroll in coverage has raised their visibility among uninsured residents in their service areas, which is expected to lead to an increasing number of those who are unable to obtain coverage seeking care at Health Centers.
The Affordable Care Act provided $11 billion in federal funding over five years to expand the Health Center program, with the goal of expanding access to health care services as more people in low-income communities obtain coverage. The volume of visits provided by Health Centers increased from 38 million in 2000 to 80 million in 2011, and Health Centers serve more than one in six low-income people nationally. Federal funding has expanded the number of Health Center medical staff, as well as staff who provide dental and mental health services. The number of Health Centers that offer some mental health services has grown significantly, from about 40 percent of health centers in 2000 to 75 percent in 2011 (Kaiser Commission 2013).36 While only 20 percent of Health Centers offer substance use disorder treatment services, all Health Centers that receive federal grants to work with homeless individuals are required to provide these services.
Health Centers vary widely in their capacity for delivering health care services connected to PSH or in tailoring their services to meet the needs of people experiencing homelessness. Some Health Centers are very engaged in delivering services to people who are homeless and to people with significant behavioral health challenges, and may receive federal grant funding targeted for this purpose. In contrast, other Health Centers have been much less engaged in serving these groups of patients. Leaders of some of the centers in the latter group say they face competing priorities as they prepare to respond to the challenges and opportunities related to implementing the Affordable Care Act and other changes in health care delivery systems. They say that they do not have the capacity to deliver the specialized, intensive, and time-consuming care needed by people experiencing chronic homelessness who have SMI or active substance use disorders. Nor do they feel they have the capacity to see people in their homes at a time when they are also seeking to greatly expand capacity in their centers to meet the increased demands for care and provide quality customer service to other newly insured patients. Other Health Centers have strengthened their commitment to serving the most vulnerable people, who are unlikely to receive care that addresses their complex health and social needs in other settings.
Health Care for the Homeless programs receive 8.7 percent of total federal funding for the Health Center Program. The more than 200 Health Care for the Homeless programs include grantees operating in all 50 states, the District of Columbia, and Puerto Rico. In addition to basic health services, HCH programs must also offer substance use disorder treatment services (directly or through referrals), establish referral linkages for mental health treatment, offer case management services and services that enable people to use other Health Center services (e.g., outreach, transportation, and translation services), and conduct patient education regarding the availability and proper use of health services. In 2012, HCH programs served more than 836,000 patients, almost 90 percent of whom had incomes below the federal poverty level.37
HCH programs are required to bill Medicaid for covered services provided to Medicaid enrollees, but currently most HCH patients are uninsured. In 2012, 61 percent of HCH adult patients in the United States did not have any public or private health insurance, and 28 percent were covered by Medicaid.38 In states that choose to implement the expansion of Medicaid eligibility under the provisions of the Affordable Care Act, most HCH patients are likely to become eligible for Medicaid coverage based on their low incomes, but barriers to Medicaid enrollment will likely persist for some people with histories of chronic homelessness who lack reliable contact information or required identification documents, or who find it difficult to navigate the application and eligibility determination process.39
Consistent with national data, HCH providers in the case study communities often reported that, until recently, the vast majority of their patients have been uninsured. As some states expanded Medicaid eligibility and others expanded coverage through Medicaid waivers in the years before the full expansion of Medicaid eligibility in 2014, HCH programs in these states experienced a significant decline in the percentage of uninsured patients, and they are increasingly receiving Medicaid reimbursement for covered services.
4.2.1. FQHC Medicaid Reimbursement
Since 2001, federal law has required State Medicaid agencies to pay Health Centers that are recognized as Federally Qualified Health Centers based on a prospective payment system (PPS). Under this system, FQHCs are paid an "all-inclusive" rate for each visit a Medicaid patient makes with certain types of health care providers, including physicians, mid-level practitioners (nurse-practitioners and physicians' assistants), licensed clinical social workers, and clinical psychologists. The rates also include all services and supplies that are "incident to" the services provided by covered providers. Each FQHC's rate is calculated by taking their reasonable costs for Medicaid-covered services during a base period and dividing them by the total number of visits. The PPS per-visit rates that are paid to Health Centers for visits provided to Medicaid patients often appear higher than Medicaid reimbursement rates paid to other types of providers that care for Medicaid beneficiaries; however, the fact that the PPS is a bundled rate precludes making direct comparisons.
Instead of paying FQHCs under a PPS, state Medicaid programs have the option to pay them using an alternative payment methodology (APM). By law, an APM must result in total payments being at least as high as they would be under a PPS, and each FQHC must agree to receive the APM.
The intent of the Medicaid FQHC payment methodology is to ensure that the costs of providing covered services to Medicaid patients are not shifted to federal grant funding from the Health Resources and Services Administration. Federal grants and other funding sources cover uninsured patients and activities not covered by reimbursement from Medicaid, Medicare, or private insurance.
Since 2001 the baseline PPS rate, which was established based on documented costs incurred during 1999 and 2000, is adjusted annually by a standard medical inflation factor. States must also adjust the PPS rate to take into account any increase or decrease in the scope of services provided by the Health Center. When Health Centers establish or expand services, such as when they establish a new team serving people who are homeless or a service site connected to PSH, this change in scope can trigger an adjustment to the Health Center's per-visit rate.
As many states are relying on Medicaid managed care plans to provide health care for a growing number of people, many Health Centers have become part of these health plans' provider networks. In many cases, the health plans make payments to the Health Centers on a capitated basis, meaning that the Health Centers receive a fixed amount of funding per-member per-month for health plan members who have selected or been assigned to the Health Center for receiving their primary care. States are required by federal law to give Health Centers additional "wraparound" Medicaid payments based on the gap between the health plans' per-member per-month payments and the revenues that would otherwise have been received by the Health Center using the FQHC prospective payment methodology based on the number of FQHC encounters.
Note that beginning in October 2014, FQHCs will begin receiving payments under a PPS system from Medicare for care provided to Medicare beneficiaries. There are substantial differences between how the Medicaid and Medicare PPS systems will function.
4.3. Health Centers, Chronically Homeless People, and Permanent Supportive Housing
In recent years a growing number of Health Care for the Homeless programs and a small number of other Health Centers have developed programs designed to engage and provide ongoing health care and supportive services linked to permanent housing for people with histories of chronic homelessness. To implement these programs, Health Centers work in collaboration with numerous partners, including providers of community-based mental health services and housing support services. They may also partner with providers of housing assistance that may be administered by public housing authorities (PHAs) or available in PSH operated by nonprofit housing organizations.40
4.3.1. Examples of PSH/Health Center Partnerships
In several case study communities, a few Health Centers were very actively engaged in expanding their roles in providing services linked to PSH, and other Health Centers were considering or planning to do so.
In Los Angeles, expanding the role of Health Centers as service delivery partners in PSH builds on the experience of Skid Row's Center for Community Health run by JWCH, the largest Health Center serving a predominantly homeless population. JWCH has a decade of experience providing services in PSH. Other Health Centers that serve a large number of people experiencing homelessness include LA Christian Health Center in Skid Row and Venice Family Clinic, both of which are now collaborating with providers of mental health and homeless services linked to site-based or scattered-site PSH. Several additional Health Centers have more recently participated in partnerships to engage and link housing and services for some of Los Angeles County's most vulnerable people, including people who are chronically homeless.
Los Angeles County's Department of Health Services designates most of the Health Centers that serve people who are homeless as "community partner clinics."41 This designation allowed the centers to receive reimbursement at the FQHC rate when they serve people enrolled in coverage through Healthy Way LA, the Low Income Health Plan established under the terms of California's Medicaid waiver.42
These Health Centers played a significant role in assisting thousands of uninsured people who have experienced homelessness to get enrolled into coverage through Healthy Way LA before 2014, and are playing a similar role to encourage enrollment into Medicaid now. The Health Centers hired staff to help people obtain documentation and complete the application and to navigate the eligibility redetermination processes. Although it has been a bumpy road, the Health Centers are now receiving reimbursement for a much larger share of their previously uninsured patients, including a larger share of the tenants in PSH.
For at least a decade, JWCH has been delivering services in PSH for people who are chronically homeless. Initial involvement came through JWCH's partnership with the Skid Row Housing Trust in the Skid Row Collaborative that was funded from 2003 through 2007 under the federal HUD/HHS/VA Chronic Homelessness Initiative.43 Project 50, which Los Angeles County launched in 2008, built on relationships begun during the Skid Row Collaborative, including a satellite clinic in a site-based PSH project developed by Skid Row Housing Trust. A JWCH primary care provider works in partnership with Skid Row Housing Trust case managers to deliver services to PSH tenants, many of whom were chronically homeless and prioritized for access to available housing units because of their vulnerability.
To obtain Medicaid reimbursement for health services provided by clinicians who go to streets or encampments to see people experiencing homelessness, make home visits in scattered-site PSH, or staff satellite clinics that operate for a few hours each week in shelters and in site-based PSH, JWCH and other Health Centers include a description of these services and locations in the project scope information they provide to HRSA in conjunction with their federal grant funding. The clinic location is used as the billing code for these services.
In addition to receiving HRSA Health Center grant funding and Medicaid payments as an FQHC, JWCH's multidisciplinary teams often rely on other sources of funding, including grants or contracts from Los Angeles County and other sources to provide some mental health and substance abuse services. JWCH also has become certified to provide some Medicaid-covered mental health and substance use treatment services outside of the FQHC Medicaid reimbursement. During the case study period, JWCH also began receiving Medicaid reimbursement for Medicaid-covered services provided in a residential treatment setting that serves some women who are homeless. Medicaid reimbursement is also available for some outpatient substance use treatment services, but JWCH has found it challenging to use this as a funding source for services to people who are chronically homeless and for PSH tenants.44
In Minnesota, Catholic Charities of St. Paul and Minneapolis developed Higher Ground, a seven-story building that combines overnight emergency shelter on the first two floors, 74 single-room occupancy (SRO) supportive housing units, and 11 affordable efficiency units on the top floor. The Higher Ground Clinic located on the ground floor of the building, staffed by the Hennepin County Human Services and Public Health Department's Health Care for the Homeless program, opened in June 2012.
The clinic operates three days a week, mostly during evening hours when people are at the shelter. It serves people using shelter services at Higher Ground or other nearby facilities, as well as the PSH tenants living in the SRO and efficiency units on the upper floors of the Higher Ground building.
The Higher Ground Clinic is the first site where Hennepin County's HCH program is delivering services to PSH tenants. It was designed to accommodate and offer assistance to the most vulnerable people in the community, including people who are chronically homeless. When selecting people to move into the PSH units, Catholic Charities prioritized those who had been homeless the longest, including those who had made the greatest use of shelter services and people engaged through street outreach efforts that focused on serving the most vulnerable people experiencing homelessness. The clinic manager reports that the tenants at Higher Ground are "the sickest people we serve" and that many tenants have serious and complex health needs, including people in wheelchairs and those recovering from a heart attack or stroke.
4.3.2. Models for Integrating Primary Care and Behavioral Health
In two case study communities, Health Centers partner with other providers to integrate primary care and behavioral health services.
Unity Health Care/Pathways to Housing Partnership in the District of Columbia
With funding from a SAMHSA grant to support the integration of primary medical care and behavioral health services, Pathways to Housing-DC and Unity Health Care have formed a partnership. Pathways-DC operates a scattered-site PSH program for people experiencing homelessness who have SMI. HUD Shelter + Care certificates subsidize most tenant rents for the privately owned apartments that program participants occupy throughout the community. Unity Health Care is a Health Center that began as a Health Care for the Homeless program and retains that focus within its now-expanded role as a Health Center.
For the service integration partnership serving formerly homeless PSH tenants, Unity Health Care added primary care providers to the Pathways Assertive Community Treatment teams that deliver services for PSH tenants. Unity clinicians deliver services at the Pathways office, where PSH program participants may come to meet with their case managers. In addition, a Unity nurse-practitioner accompanies Assertive Community Treatment teams during home visits and street outreach. Unity Health Care has a homeless outreach component to which this nurse-practitioner is formally attached, so the services he or she delivers can be billed under Unity's FQHC auspices.
Virtually all of Pathways-DC clients are Medicaid beneficiaries, mostly because their mental illness qualifies them for SSI. Some people contacted through outreach who are not yet beneficiaries would qualify for Medicaid because the District of Columbia expanded coverage in 2010 to people with incomes below 200 percent of the federal poverty level, and the enrollment process is relatively easy and quick. In the past year the more than 500 clients of Pathways-DC have made almost 1,000 Unity clinic visits, increasing the health care engagement of this very vulnerable population. Most of these people used health care infrequently before the Pathways-Unity partnership was established.
Integrated Mobile Health Teams in Los Angeles County
The Los Angeles County Department of Mental Health has funded five Integrated Mobile Health Teams using funds set aside by California's Mental Health Services Act for testing innovative care models. The team model is designed to serve people with SMI who also have other vulnerabilities, including advanced age, many years of homelessness, co-occurring substance use, or other physical health conditions that require ongoing primary care such as diabetes, hypertension, cardiovascular disease, asthma or other respiratory illnesses, obesity, cancer, arthritis, and chronic pain.
Each multidisciplinary team is staffed from 1-2 mental health service providers and a Health Center. As specified in Department of Mental Health contracts, the vision is for staff from these partnering organizations to work together "as one integrated team to provide mental health, physical health, and substance use services" and "operate with one set of administrative and operational policies and procedures and use an integrated medical record/chart to ensure integrated and coordinated services." Team services are intended to increase immediate access to housing by using a housing-first approach that incorporates harm reduction, motivational interviewing, and access to housing without requirements for treatment, sobriety, or "housing readiness." Each team partners with a PSH developer(s) to have housing units dedicated to the team's clients. Except for a few administrative activities and medical procedures that require an established setting, virtually all team services are delivered in the field, including engaging people experiencing homelessness on the streets and making home visits to people in PSH.
For outreach and engagement work, the team's mental health and medical staff go together to the streets, encampments, and other "hot spots" to engage potential clients and talk to social workers at shelters and hospitals. The team tries to find highly vulnerable people who have not been well-connected to mental health services. Providers report that the people they serve through these Integrated Mobile Health Teams are sicker, more vulnerable, and have more severe and untreated mental illness and/or substance use problems than the people their agencies usually serve. Nearly all have co-occurring substance use disorders and most are uninsured at the time of enrollment.
Medicaid and Integrated Mental Health Team Services
Although many of the people served by the teams were uninsured when they first became clients, the teams have helped about half of their clients to enroll in Medicaid. Before 2014, the remaining clients were either enrolled in Healthy Way LA, the county's program offering coverage under California's Medicaid waiver, or uninsured. The teams worked to help their uninsured clients to enroll in Healthy Way LA, often doing so in conjunction with helping them gather the documentation needed to complete applications for housing assistance. Much of the documentation needed to establish eligibility (identification, proof of citizenship or residency, proof of income) was the same for both housing assistance and health coverage under the waiver. Thus, the teams worked with a client to gather the documentation once and used it for multiple applications. Most people who enrolled in Healthy Way LA became eligible for Medicaid in 2014.
Mental Health Services Act funding administered by the Los Angeles County Department of Mental Health for the Integrated Mobile Health Teams provides the nonfederal matching funds to leverage reimbursement through Medicaid. The service funding for the teams also leverages other resources for program participants, including housing assistance funded by other programs. The service providers are expected to use the Mental Health Services Act funds for costs that cannot be reimbursed through other funding sources. As of early 2013, only a fraction of the teams' costs were being covered through Medicaid reimbursement--usually half or less. The Department of Mental Health expects that Medicaid reimbursement will cover an increasing portion of project costs and contribute to the financial sustainability of these program models in the future. In addition to the flexible Mental Health Services Act funding administered by the county, several of the teams have also received grant funding from foundations to build their capacity and cover a portion of staff salaries and other costs for services that are not covered by Medicaid.
The vision of fully integrated teams, with shared procedures and records, is ideal for people who experience chronic homelessness. Payment mechanisms and bureaucratic procedures, however, still have some catching up to do, as the providers working to implement the model must still meet separate state and county agency requirements for documenting and billing for Medicaid reimbursement. Service providers reported that the billing mechanisms for FQHC and mental health services are completely separate and different, and that the separate payment mechanisms were not designed or modified to support or accommodate integrated care. This has created some frustration for team members and a learning curve for their organizations as they build collaborative partnerships without being able to fully integrate record-keeping and billing systems.
Example: The Exodus Recovery/LA Christian Health Center Team45
This Integrated Mobile Health Team partners with Skid Row Housing Trust for the PSH that its clients use. The trust set aside 50 apartments in one of its new PSH projects to provide permanent housing for people experiencing homelessness who are eligible to receive mental health services, including tenants who are served by this team (other units in the building are for low-income residents but are not designated for people experiencing homelessness or people with disabilities). Skid Row Housing Trust case managers work with building tenants and are integrated into the team's activities.
Because a PSH unit may not be immediately available when the team has a client willing to accept housing, the team tries to get people into interim "safe harbor" housing on the same day that they complete the assessment and enrollment process. Providing interim housing if needed reduces the chances that the team will lose the client while gathering the documentation needed to complete the application process for a housing subsidy and finding or waiting for a permanent housing unit. Arrangements to move into a permanent unit are made as soon as a unit becomes available and the client has been approved for a housing subsidy. The team establishes a coordination plan with each client from day one, which it updates after 3-6 months. The plan is flexible and can be adjusted based on new information and new goals.
Formal and informal opportunities for team members and clients to interact are plentiful. Health Center medical staff hold clinic hours every Thursday on-site at the PSH building, and also come to the building every day to participate in a morning meeting with other team members. Each day one of the team's case managers "patrols" the building, making the rounds, knocking on doors, and checking on tenants to ask how they are doing. This provides a chance to ask people if they are taking their medications and if they have any complaints or concerns. There is a cooking group and, at the end of the group meeting, an "ask the doctor" session with the team's medical provider and a mental health clinician from Exodus Recovery.
Exodus has long been a Medicaid provider through its contracts with the county's Department of Mental Health. Its primary care partner on the team, the LA Christian Health Center, became a Healthy Way LA provider in late 2012, qualifying it for the first time to receive reimbursement for care provided to Healthy Way LA members. The Exodus/LA Christian Health Center team reported that about 20 percent of its clients had Medicaid at the time of enrollment in services; the team was able to increase this proportion to about 50 percent over a period of eight months. The team includes a staff position that focuses on benefits, filled by a couple of people who are familiar with the SSI application process. The team also asked the state to designate staff for processing SSI applications from program participants to increase the speed and success of the application process and thereby also qualify more people for Medicaid by reason of being SSI recipients.
4.3.3. Models for Serving Frequent Users of High-Cost Care
In both Los Angeles and Chicago, Health Centers participate in collaborative partnerships that work to identify, engage, and deliver services and housing to people who are chronically homeless and have frequent and avoidable hospitalizations and emergency room visits. These projects seek to improve health outcomes and housing stability for program participants while also significantly reducing the high costs associated with the avoidable use of crisis services.
In Chicago, Heartland Health Outreach and the AIDS Foundation of Chicago (AFC) are partnering in a Medicaid Supportive Housing Project that uses HUD grant funding for 48 units of scattered-site supportive housing and intensive case management services, and leverages Medicaid reimbursement and other funding obtained by Heartland Health Outreach for services it provides to program participants.
The project serves people experiencing homelessness who have been identified as high users of Medicaid-reimbursed services. The Illinois Medicaid agency analyzed service use and cost patterns of its Medicaid beneficiaries and divided the population into deciles representing shares of Medicaid service costs. The state has calculated the average Medicaid costs for each decile and found that the top three cost deciles (accounting for 30 percent of the costs) include only about 1 percent of people enrolled in Medicaid.
The project targets people experiencing homelessness whose Medicaid use falls in the top six deciles.46 As project staff identifies homeless individuals at hospitals and other locations, they conduct initial assessments and then submit prospective client names to the state Medicaid office to see which cost decile the person is in. This allows AFC to estimate participants' presupportive housing Medicaid costs (based on the average for persons in that decile) without obtaining the details of each person's actual service utilization history or costs. Using average annual costs for the deciles of the first 49 people served by the program, AFC estimates that their total annual presupportive housing Medicaid costs were more than $50,000 per person per year, or at least $2.5 million for the group.
Nearly all the project's clients were chronically homeless, and nearly all have a serious mental illness or substance use disorder--usually both. Most have spent time in jail or prison, usually as a result of drug-related charges. As program implementation continues, the project will give its partners the opportunity to better understand the differences among Medicaid users with the highest costs, and between that group and those with costs that are still significant but in lower deciles, including differences in needs, characteristics, and success in supportive housing.
Case managers funded by the project's HUD grant devote most of their time to helping clients get and keep housing. This often includes working with clients to address substance use issues. Case managers coordinate with primary care providers at Heartland Health Outreach and with other health care services, and they help program participants keep appointments and follow through on the medications and recommendations they receive from their health care providers. For PSH tenants who receive care from Heartland Health Outreach, the case managers have access to electronic health records, with client consent, and this makes care coordination easier and more effective.
In Los Angeles, the Corporation for Supportive Housing and the Economic Roundtable are collaborating to support the implementation of partnerships that involve 17 hospitals, seven Health Centers, and more than a dozen organizations that provide housing and social services navigators, permanent supportive housing, interim housing, benefits advocacy, and other supports. Seven collaborative projects have been developed through the Corporation for Supportive Housing's Frequent Users Systems Engagement (FUSE) Program, funded through several foundations and federal grants, and a Social Innovation Fund (SIF) grant from the Corporation for National and Community Service. Each project seeks to engage high-need people experiencing homelessness who have been identified by participating hospitals as "frequent users."
When potential participants are identified--usually when a person who is homeless is receiving inpatient care at the hospital or making repeated visits to the emergency room--hospital social workers contact FUSE project staff to determine whether the person is likely to be among the most costly 10 percent of people experiencing homelessness and using crisis services. FUSE staff make this determination using a triage tool developed by the Economic Roundtable that identifies homeless people likely to be in the tenth cost decile. In 2012 the Economic Roundtable revised the triage tool to use data that is likely to be available in hospital settings, using diagnostic information, demographic characteristics, and other information that people experiencing homelessness themselves can provide.47
Most of the direct services offered by the FUSE/SIF projects are delivered by the partner organizations in each collaborative that take responsibility for social services and housing navigation. These providers (known as navigators) use grant funds to pay for a team that delivers an array of flexible services, including case management; assistance with applications, including those for SSI, Medicaid, and housing assistance; and interim housing and connections to permanent supportive housing. The navigators also facilitate rapid connections to medical care at the partnering Health Center as well as mental health and other behavioral health services as needed.
The navigators help program participants get to their appointments at the clinics and work to solve problems related to engagement in and access to health care and other services. Sometimes the offer of temporary or interim housing and help to access permanent housing makes the FUSE project very attractive to people who might not otherwise be willing to engage in services, while other people may be ready to try a residential treatment program after a serious health crisis serves as a "wake-up call" about the health consequences of alcohol or drug use and life on the streets.
In most cases the Health Center partner in these collaborative projects is receiving little or no grant funding to support FUSE or SIF project implementation, and many of the participating Health Centers have not made significant changes in their approach to delivering medical care to the people experiencing homelessness served by these projects.
Instead, the navigator is responsible for helping FUSE project participants get connected to care at the Health Center and may help the participant get to appointments and communicate with medical providers. While some of these Health Centers have a long history of serving people experiencing homelessness, others have little such experience, and even less experience serving chronically homeless people with challenging behavioral health issues. Participation in a FUSE project is increasing awareness at these Health Centers of the needs of frequent user patients with behavioral health problems and those who are experiencing chronic homelessness, but in general these centers have not changed their practices to deliver care through home visits or in other settings, or to assign Health Center clinicians to work as members of interdisciplinary teams.
4.4. Sustaining and Expanding Innovative Programs: Addressing Challenges for Health Centers and Their Partners
As part of this case study project, we visited many Health Centers, including some that began as Health Care for the Homeless programs. Among the Health Centers that have been most engaged in serving people experiencing chronic homelessness and delivering services in PSH, innovative programs and integrated services have often been launched with support from time-limited grant funding provided by local governments, foundations, or federal grants. Health Centers involved in these innovations have incorporated some or all of the practices described below:
They deliver health services "outside of the four walls" of a Health Center, by sending clinicians or teams to visit people in their apartments or where they are living on the streets or in encampments, and by co-locating satellite clinics in supportive housing buildings, shelters, and treatment programs.48
They do "whatever it takes" to engage, listen to, and establish trusting relationships with clients who have multiple medical and behavioral health disorders but who may not trust health care providers or seek treatment.
They use techniques such as motivational interviewing to help clients recognize and reduce harms associated with substance use, reduce or eliminate problem behaviors that could lead to the loss of housing, and take steps toward recovery, even if the clients are unable or unwilling to enter more structured treatment programs or to make and sustain a commitment to sobriety.49
They use nurses to make frequent face-to-face visits, to monitor and help clients understand and manage their chronic health conditions, to encourage them to take medications and follow through on recommendations from doctors, and to provide coaching for healthier behavior.
They build multidisciplinary teams and collaborations that can integrate the delivery of different types of Medicaid-covered medical and behavioral health services and supports, often using different types of Medicaid payment mechanisms.
They include community health workers, peer support workers, and other unlicensed workers as members of multidisciplinary teams.
They ensure access to care and continuity of care as people experiencing homelessness and supportive housing tenants are enrolled in Medicaid managed care.
They recognize housing as a social determinant of health, and help clients get and keep stable housing as a foundation for accessing and making effective use of health care services.
The Health Centers involved in these innovations generally have been expected to use Medicaid financing to sustain promising programs and activities that were often initiated with grant funding. Health Centers sometimes encounter challenges when they seek to use Medicaid to sustain and replicate promising practices for delivering services in supportive housing and to integrate primary care and behavioral health care.
As Health Centers have worked to obtain Medicaid reimbursement using the FQHC payment mechanism, some have reached agreement with state policymakers and Medicaid program officials to ensure that ongoing funding is available to cover the costs of reaching, engaging, and serving people who are living in PSH, as well as those who are still experiencing chronic homelessness. In some cases, however, it has been more challenging to use Medicaid to sustain, expand, and replicate promising practices and programs that include Health Centers.
The practices just detailed--while important for effectively serving people experiencing chronic homelessness and other high-need Medicaid beneficiaries with complex medical and behavioral health conditions--are not easy to finance using the FQHC payment mechanism. Some Health Centers have found it difficult to cover some of the costs associated with these practices using the FQHC PPS payment mechanism.
To sustain and expand some of the innovative programs that have been created in recent years, Health Centers, Medicaid program officials, state primary care associations, and other stakeholders are working to clarify policies, to explore payment reform ideas, to continue using grant funding to fill gaps, or to find other solutions. For states, housing and service providers, and other stakeholders seeking to expand the role of Health Centers as providers of integrated primary care and behavioral health services for people who are experiencing homelessness or living in PSH, it will be important to anticipate and recognize these challenges and to collaborate with state Medicaid program leaders in seeking solutions. This may include considering these activities when determining reasonable costs for FQHC services, including services "incident to" care provided by physicians or other clinicians, or exploring alternative payment mechanisms for some promising programs.
4.4.1. Delivering Health Services "Outside the Four Walls": Addressing Concerns About Productivity
While states take varying approaches, they may scrutinize some Health Centers that seek Medicaid reimbursement for care delivered "outside the four walls" of a Health Center.
Generally, the care provided outside of a Health Center must be clearly part of the comprehensive primary care delivered by the Health Center operating under the oversight of the Health Center's medical director. Some Health Center leaders are wary of seeking Medicaid reimbursement for visits provided by their clinical staff when they see clients outside of a Health Center. It is often helpful to clarify state policies and to correct inaccurate information about the availability of Medicaid reimbursement for these visits.
Even when it is clear that Medicaid reimbursement can be available for visits outside of a Health Center, program administrators and Medicaid officials often have concerns about the productivity of clinical staff members who work on mobile teams or deliver care in satellite Health Center sites in PSH buildings or through home visits. Some Health Centers that have been engaged in delivering health care and other services in PSH have encountered challenges in delivering enough "billable encounters" to produce enough revenue to make these services financially viable and sustainable. Clinicians who work with people who are chronically homeless generally have lower rates of productivity, as measured by the number of visits per hour or day, compared with clinicians who work in busy clinic settings. In part this is because it often takes extra time to establish trust and to communicate with people who have experienced chronic homelessness. They may be distrustful of health care providers, or their thinking and ability to communicate may be impaired by mental illness, substance use, brain injuries, or other disorders. Many people who are experiencing chronic homelessness, and particularly those who have been prioritized for PSH because of their vulnerability, have multiple serious medical and behavioral health conditions, including chronic medical conditions such as hypertension or diabetes, cancer, HIV/AIDS, or the consequences of a stroke or traumatic brain injury. It takes extra time to assess and treat these multiple conditions, and to address complications that may arise when patients are taking medications for both medical and mental health conditions.
Health Center clinicians who work on teams doing outreach and delivering care to people who are chronically homeless and living on the streets or in encampments cannot complete and document as many reimbursable visits as they might provide in a clinic setting. Teams spend time trying to locate people experiencing homelessness, and with some people who are very reluctant to accept care, the process of engagement may take weeks or months. As Health Center workers seek to establish a person's trust so they can deliver much-needed medical care, they often must take time to listen to the person's story and may need to offer help with immediate practical concerns, such as meals, dry socks or warm clothes, or a bus pass. Eventually after trust is established, the client is often willing to consent to receive medical care and treatment, but the time spent on these relationship-building efforts is usually not reflected in billable encounters.
Even in site-based PSH settings, it can be challenging to make the best use of clinicians assigned to satellite Health Center sites on a regular part-time schedule. Several Health Centers reported that the volume of billable encounters provided in these settings was less than they had anticipated. This is particularly challenging in buildings with a small number of PSH units, but even in larger PSH buildings a large volume of billable encounters may be difficult to achieve because some tenants are reluctant to manage chronic illness and change behaviors associated with health risks.
Even if PSH tenants have significant health needs at the time they first move into housing, after a year or two they often need less medical care. Many tenants appreciate the accessibility of on-site health services in PSH or home visits by medical providers, and this access may be critically important for PSH tenants who are unwilling to visit a Health Center or find it difficult to use services in clinics or doctors' offices because of the symptoms of their mental illness. Other people may no longer prefer to see their primary care provider at home and may instead prefer to see the same provider at a Health Center site that serves other community residents, if it is nearby and welcoming. To use Health Center staff more efficiently and to meet revenue targets, satellite Health Center sites located in or close to PSH may also serve other patients from the surrounding neighborhood or former PSH tenants who have moved out to other housing. Health Centers and their partners will need to continue to evaluate the approach to delivering services and the mix of services that are based in Health Center sites or delivered in other settings.
In some collaborations, Health Center clinical staff accompany teams of service providers on home visits to previously homeless people who live in scattered-site PSH, while in other partnerships the Health Center has determined that home visits are not financially feasible because of productivity concerns. If a scattered-site PSH program also uses an office location where some tenants come to see their case managers or participate in group activities, the Health Center's primary care provider may see clients at that location and also coordinate with other team members without making visits to clients in their own apartments.
In some states Medicaid officials have raised concern about the productivity of Health Center clinicians and the impact of productivity on the rates established using the FQHC PPS payment methodology. The Federal Government does not provide much formal guidance to states regarding FQHC payment methodology for Medicaid services, and there have been lawsuits and appeals by Health Centers in some states challenging efforts by states to use productivity "screens" or standards to determine whether the per-visit costs reported by Health Centers reflect reasonable costs, and to reduce rates for Health Centers if clinicians have lower levels of productivity. Given the complex needs of people who have experienced chronic homelessness, and the experiences of promising programs that deliver comprehensive health care linked to housing for this group of people, Health Centers interested in serving this population and delivering care linked to PSH might want to open discussions with their state Medicaid office about the costs for these programs and the productivity of clinicians working in these settings.
4.4.2. Covering the Costs of Unlicensed Members of Interdisciplinary Teams
When teams do outreach to deliver care to people experiencing chronic homelessness, paraprofessional outreach workers and peers who know where hard-to-serve people sleep or spend time can help to find people, establish trust, and motivate change. By making introductions and a "warm handoff" they can help to make the best use of clinicians' time in the field. Site-based PSH case managers are often very helpful in scheduling appointments and reminding tenants about when health care services will be on-site in their building. Ongoing communication and collaboration among Health Center clinicians and the staff members or partner organizations providing outreach and case management services can help to boost the productivity of clinical team members and to focus their attention on individuals with the greatest unmet needs for care.
| JWCH's Center for Community Health is in the heart of Skid Row. The center is designed to support the delivery of integrated services including medical, mental health, substance abuse, clinical pharmacy, dental, and other services and supports. The building is designed to support interdisciplinary teams working in "pods," so that a primary care provider can walk a client over to a mental health provider for assessment on the same day, and team members can consult with one another. Each team (i.e., each pod) is responsible for a group of patients and uses weekly case conferencing to coordinate care for those with the most-intensive needs. Because California does not provide FQHC payment for more than one visit on the same day, JWCH receives payment for only one visit, even if a patient is seen by two different medical providers or by both a medical and mental health provider on the same day. |
|---|
Community health workers, case managers, peer recovery specialists, and other unlicensed staff are frequently essential members of interdisciplinary teams, helping to engage vulnerable people in care and provide the health education, coaching, and case management services that help people reduce risks and better manage their own health. Costs for these staff members are sometimes excluded from the calculation of FQHC payment rates if states do not consider these to be reasonable costs associated with FQHC services. It may be difficult for Health Centers to find sustainable sources of funding for these staff positions.
Even when multidisciplinary services are delivered by licensed clinicians, many states, including some with sites in this study, do not permit FQHC reimbursement for two or more visits by the same patient on the same day for the same condition. This has the effect of limiting Medicaid revenues for more comprehensive or integrated care provided by teams in some Health Centers. Particularly for people experiencing chronic homelessness and for other people who are distrustful or hard to engage in needed health care services because of symptoms of mental illness or other challenges, "warm handoffs" from one clinician or team member to another are an important strategy for delivering effective care.
4.4.3. Services for People With Substance Use Disorders
For residents who have serious substance use disorders and do not seek treatment, motivational interviewing techniques can be effective. Having a member of the service team who focuses on substance use and recovery--or "peer" team members who have personal experience with homelessness, mental illness, addiction, and recovery--can have a big impact on successfully engaging tenants in the services they need. These service interventions can be critically important, helping to solve problems that might otherwise result in serious medical complications, hospitalization because of a mental health crisis, arrest, or eviction and a return to homelessness. In most states, these services are not part of the Medicaid benefits that cover treatment for substance use disorders.
While Health Centers recognize that substance use has a significant impact on health, and HCH providers are required to deliver services to address substance use, Medicaid reimbursement for services related to substance use problems was limited in the communities described in this report during the study period. Many states had a limited set of optional Medicaid benefits to treat substance use disorders, although some states are expanding coverage for these services as they implement changes required by the Affordable Care Act. For example, California is expanding Medicaid coverage of substance use treatment services that were previously covered only for pregnant and post-partum women; starting in 2014 these services were be covered for all adults.
State policies may limit the settings in which these covered services can be delivered. In Illinois and California, for example, Medicaid reimbursement for substance use disorder services is available only in designated sites that have obtained certification as treatment facilities. This limitation makes it virtually impossible to use Medicaid to pay for services delivered through integrated, multidisciplinary teams that serve people experiencing homelessness on the streets, in satellite clinics in PSH buildings or program offices, or through home visits. State policies regarding benefit design often require that Medicaid-covered substance use disorder treatment services must be delivered in settings that are certified as treatment facilities, such as residential programs or intensive outpatient programs that require regular participation for a minimum number of structured hours each day or week. States may require Health Centers to exclude the costs of these programs from the FQHC payment methodology, and to operate them as completely separate programs in separate facilities, making it difficult to fully integrate services that address medical, mental health, and substance use disorders.
Many Health Centers offer some services to address substance use disorders, including screening and brief intervention or counseling services provided by primary care providers or licensed clinical social workers, which may be reimbursed through the FQHC payment mechanism. Some Health Centers offer other substance use disorder services as part of grant-funded programs. Relatively few Health Centers visited as part of this research also operate substance use disorder programs that qualify for Medicaid reimbursement.
Health Centers that participated in this case study reported that many of the people who are experiencing chronic homelessness or living in PSH are uninterested or unable to participate in highly structured treatment programs. While treatment can be successful, offering a path to recovery for some PSH tenants, others have been through treatment programs several times without being successful in achieving or maintaining sobriety. As a result, some Health Centers that serve many people experiencing chronic homelessness have found it difficult to use Medicaid-covered substance use treatment benefits to finance the engagement and motivational interviewing services that are often most needed to reduce their clients' substance use and related health problems, particularly when the use of alcohol or drugs is a threat to the client's health, safety, or housing stability.
4.4.4. The Role of Nurses
The Health Centers and HCH programs that deliver services in PSH and their housing partners often noted that many of the most vulnerable PSH tenants can benefit from services that may be provided by registered nurses in home visits. Registered nurses who work as members of interdisciplinary teams can assess and monitor health needs, educate people about managing chronic medical conditions, help people follow up on doctors' recommendations, and answer questions about medications.
While the costs of registered nurses are likely to be included in the calculation of Health Center costs and used to set the rate paid for FQHC visits with other medical providers, registered nurses do not provide "billable encounters" that directly produce revenue for the Health Center.50 This can make it difficult for a Health Center to add nurses to provide additional services for PSH tenants, because the Health Center does not receive additional revenues from Medicaid reimbursement to cover the added costs for these staff. In several sites we were told that there is significant demand for home visits by registered nurses to PSH tenants, but it is difficult for Health Centers to provide these services without additional, flexible funding.
Similarly, medical respite services, often staffed by registered nurses, may be a critical link to PSH, providing interim housing for people who are chronically homeless and get engaged in services at the time they are being discharged or diverted from a hospital stay. However, the FQHC payment methodology does not reimburse most of the costs associated with the respite model, per federal regulations.
4.4.5. Strengthening Partnerships To Deliver Multidisciplinary Care
Building and sustaining partnerships among PSH providers, other service providers, and Health Centers is not easy. Each partner in these collaborations speaks a slightly different language and responds to the requirements and incentives of different funding streams and government agencies that provide oversight. Billing systems and electronic health records used by Health Centers usually do not integrate or share data with the record-keeping systems used for mental health or other supportive housing services.51 In part this is because these systems have been designed to meet the requirements of separate systems that manage Medicaid health and behavioral health benefits, and the requirements of these systems have not been aligned.
Even when the Health Center has made a commitment to assign staff to a satellite clinic, there may be a tendency to pull the clinician from the PSH site when staff vacancies produce uncovered time in the Health Center's busy clinic. Relationships can get strained, particularly when funders have arranged "marriages" between Health Centers and their partners. Regular structures for ongoing collaboration, including frequent meetings to coordinate the delivery of services to shared clients, to plan for improving and sustaining programs, and to share training and learning opportunities can strengthen partnerships and enhance the integration of services.
4.4.6. Managing Transitions to Managed Care
In some of the case study communities, Medicaid managed care plans are increasingly responsible for coordinating and paying for health care services for seniors and people with disabilities who are enrolled in Medicaid. When people become enrolled in managed care plans, some Health Centers that serve people who are chronically homeless and those that deliver health services connected to PSH have encountered difficulties.
We summarize those difficulties and the potential solutions here because many states either already require or are anticipating requiring that this population be served by managed care plans. With appropriate forward planning, other communities may be able to avoid some of the complications we observed and promote the greatest degree of patient continuity of care during transition periods.
Know what is coming. Awareness of the nature and timing of state plan requirements to enroll in managed care is critical. During transitions to managed care, people experiencing homelessness and many of those who were recently homeless do not receive or understand notices regarding health plan and provider selection. If they do not respond to these notices, they may be "auto-assigned" to an unfamiliar health care provider instead of being assigned to the Health Center that delivers care attached to a shelter, drop-in center, mental health clinic, or PSH program where the person has been getting care. This can limit access to health care or disrupt the continuity of care, while also making it difficult to sustain partnerships that link Health Centers to PSH or other services for people experiencing homelessness.
With advance help, service providers in PSH and homelessness assistance or mental health programs can assure that their Medicaid clients know their options and the time frame for exercising their right to choose a provider. It is important for states to make their plans clear in a timely manner and to engage community partners who can reach groups of beneficiaries who lack a permanent address or may have difficulty understanding written notices. It is also important for community-based service providers to have a clear idea of how the managed care enrollment process will likely impact their clients, and what might work best to avoid disruptions in care that occur when someone is assigned to a new and unfamiliar primary care provider and health organization instead of the one the patient knows and trusts.
Have a good data system. The data system used by the states and managed care organizations responsible for assigning patients to primary care providers and provider networks needs to have timely and up-to-date information about each Medicaid beneficiary's existing care arrangements. This information would reduce inappropriate provider assignments in the event that people do not make their own choice of provider. In addition, Health Center staff and other care providers need to have a way to see whether their patients have been assigned to them or to another provider or network because if they deliver care to a person who is not assigned to them, the Health Center may not receive payment for these services.
Have a good system for switching health plans and/or primary care provider assignments. If inappropriate assignments that disrupt care are made, having a system that makes switching assignment easy would be helpful. To facilitate the efforts by Health Centers to engage and provide easy access to care for some of the most vulnerable and hard-to-serve people experiencing homelessness or living in PSH, health plans and provider networks may need to negotiate arrangements to make these changes effective immediately, rather than having to wait until the next month for them to become effective.
4.4.7. Competing Demands and Opportunities--and Limited Capacity
Many Health Centers are not engaged in serving people who are chronically homeless and may not see this population as relevant to their role in the community or consistent with their mission, particularly if the Health Center does not receive federal funding as a Health Care for the Homeless program. During the months leading up to and following full implementation of the Affordable Care Act, Health Centers have been facing many competing demands to expand their capacity to enroll and serve new patients and improve customer service for many existing patients who have other choices once they become Medicaid beneficiaries or recipients of subsidized insurance coverage. At the same time, they must also work to adopt electronic health records and participate in Medicaid managed care arrangements, which often involve multiple plans with different payment systems and procedures for coordinating specialty care and other health services with separate provider networks. Faced with all of this, as well as the impact of state budget reductions, some Health Center leaders are reluctant to focus their limited resources and staff time on people who are chronically homeless--a relatively small group among the many low-income people in their communities--and on unfamiliar potential partners from homelessness assistance, housing, and behavioral health systems.
As described earlier, Mental Health Services Act funding and additional support from philanthropy have provided critical funding in Los Angeles to cover the activities of integrated mental health teams that cannot be reimbursed by Medicaid. This funding has helped to launch or expand and strengthen collaborations among Health Centers and providers of behavioral health care services. In other communities, these or similar sources of flexible funding have not always been available. Without targeted grant funding or other sources of funding to expand their capacity to provide additional behavioral health services to persons with serious mental illness and co-occurring substance use disorders, many Health Centers have little or no capacity to serve people who do not show up for their clinic appointments, or those who may be disruptive or unable to sit quietly in crowded waiting rooms.
4.5. Summary
Given their mission to serve low-income people and, in some cases, their Health Care for the Homeless resources, Health Centers can be critical players in linking primary care, behavioral health, and other services and supports to people with histories of chronic homelessness and to PSH tenants. Promising models are emerging, including co-locating clinics in PSH or using multidisciplinary mobile outreach teams, such as those in Los Angeles, as well as special initiatives targeted to frequent users of crisis care, such as those in Los Angeles and Chicago. All require "working outside the walls" of the Health Center.
Health Centers face uncertainties about the full implementation of the Affordable Care Act. Most of their clients were uninsured before 2014. Some clients may no longer seek care at Health Centers once they become eligible for Medicaid and have other choices for care. Some will still be uninsured because they are undocumented or are in the five-year blackout period after getting residency and before becoming eligible for benefits. Clients may also have trouble successfully completing the Medicaid application/eligibility process.
As implementation progresses under the Affordable Care Act, discussions among state Medicaid officials and representatives of Health Centers will be vital. It will take good communications for all parties to understand each other's opportunities and constraints, and for strategic frameworks to develop that facilitate the goals of patients, the Health Centers, and state Medicaid interests.
5. Mental Health Services and Medicaid as of 2013
Chapter 5 Highlights
Among people experiencing chronic homelessness, those with a diagnosis of serious mental illness may be the most likely to benefit from supports funded in part through Medicaid. This is because they are likely be eligible for Supplemental Security Income (SSI) and be Medicaid-eligible; to come under the aegis of state and county mental health departments, which have responsibilities for their well-being; and to qualify to receive the most effective models of community-based treatment and supports for recovery as identified by extensive research.
Serious mental illness is usually determined by a person's diagnosis, history, and functional impairments. States specify qualifying diagnoses in their Medicaid state plan, virtually always including psychoses, bipolar disorder, and major clinical depression, and sometimes including other diagnoses. In addition, a person's mental illness must "result in functional impairment that substantially interferes with or limits one or more major life activities." Activity areas may include feeling, mood, and affect; thinking; family relationships; interpersonal relationships/social isolation; role/work performance; socio-legal conduct; and self-care/activities of daily living.
Medicaid state plans usually specify how eligibility for mental health services is to be determined. Standardized rating scales are often used, as is consideration of previous psychiatric inpatient admission and utilization. States may also take into consideration other risk factors such as chronic homelessness, repeated arrests and incarcerations, lack of follow-through taking medications, failure to achieve stable housing, ongoing inappropriate public behavior, excessive use of crisis or emergency services with failed linkages, and similar indicators of functional impairments.
Persons with a serious mental illness who are in the public system will most likely qualify to receive community-based mental health services, which usually include services and coordination covered in Medicaid state plans under the rehabilitative and targeted case management options. These approaches are intended to support people who need some level of ongoing assistance beyond what they can get through standard outpatient care in a clinic but who do not need residential treatment or hospitalization, or for whom residential treatment or hospitalization can be averted with appropriate supports delivered in a community setting.
Case study sites used a number of different terms to describe the community-based mental health services that are linked with PSH, including Assertive Community Treatment in Illinois, the District of Columbia, and Minnesota; Full Service Partnerships in California; Field Capable Clinical Services in Los Angeles; Community Support Services or Community Support Teams in Illinois and the District of Columbia; Community Psychiatric Support and Treatment in Louisiana; and Adult Rehabilitative Mental Health Services in Minnesota.
Minnesota makes extensive use of Medicaid targeted case management benefits to provide support and linkages to other services for people living in PSH. Targeted case management benefits are well-suited to helping people who are experiencing homelessness access housing, as covered services include assessment, service plan development, and the referral, monitoring, and follow-up often used to help people get and keep housing.
Public mental health agencies in the case study sites support housing for people experiencing homelessness in several ways: funding the development of housing units (Connecticut, Los Angeles, the District of Columbia); subsidizing rents (Connecticut, Minnesota, the District of Columbia); and participating in partnerships to expand rental subsidy resources (Los Angeles, the District of Columbia).
Several models exist at the provider level for linking health and behavioral health care, supportive services, and housing, starting with outreach and engagement to initiate connections with people experiencing homelessness. Thereafter, models include: (1) one agency that provides housing and services; (2) partnerships in which one agency provides the housing and another provides the behavioral health and other supportive services; and (3) one agency that provides the housing and each tenant is linked to his or her own primary service provider.
Many issues related to payment were common across case study sites. These involved mainly which aspects of the supports needed by people experiencing chronic homelessness and PSH tenants the Medicaid arrangements available during the study period (2010-2012) would and would not pay for.
Medicaid reimbursement often covered community-based rehabilitative services, including services provided in the consumer's home or other community settings, that focus on the individual's recovery and resiliency goals.
Covered services included support for the development of interpersonal and community coping skills, assisting consumers in self-monitoring and managing symptoms of mental illness, and developing strategies and supports to prevent relapse and avoid hospitalizations or the use of crisis public services.
Some services that are important elements of programs that serve people who have experienced chronic homelessness often are not included in definitions of Medicaid-covered mental health services. These may include finding the client, collateral contacts done without the client present and other care coordination activities, teaching people new things (as opposed to restoring previous capabilities), care not specifically related to the mental illness (e.g., wound care, managing diabetes), transporting the client to appointments or to search for housing, and travel time.
5.1. Introduction
Among the individuals experiencing chronic homelessness, people with a diagnosis of serious mental illness (SMI) may be the most likely to benefit from supports funded in part through Medicaid. This is true for at least these four reasons:52
Public Agency Responsibility: State and local mental health authorities are charged with ensuring the well-being of this group of people. These agencies have historically been responsible for arranging mental health services and long-term residential care for their SMI clients, so it has been possible for the agencies to extend those responsibilities to include people with SMI who are chronically homeless and to develop or contract for services in PSH. People with disabling physical conditions or substance use disorders do not have a public agency with similar responsibilities for their well-being.
SSI Income: Mental illness that falls within specified diagnoses and creates a significant level of functional disability qualifies people for Supplemental Security Income (SSI)--a critical source of financial support.53 SSI provides an income from the federal program, as well as supplements for certain types of housing arrangements in some states. With SSI income, people with mental illness who are chronically homeless can help pay for their own housing, making it more financially feasible for mental health service agencies to offer housing.
Medicaid Eligibility: SSI beneficiaries are categorically eligible for Medicaid and often for specialty mental health services available through different components of a state's Medicaid plan. In turn, Medicaid provides a funding source for services that supplement state or county mental health contracts and federal grants, if the service providers already are or are able to become certified as Medicaid providers.
Research Evidence and Evidence-Based Practices: Since the early 1990s, the National Institute of Mental Health, Robert Wood Johnson Foundation, Conrad N. Hilton Foundation, and other funders have invested in research to document what works to end homelessness for people with mental illness. The results are a body of knowledge that can guide practice and reassure potential funders of likely success.
This chapter describes the ways that Medicaid helps pay for mental health service arrangements connected to PSH in four of our case study sites: California, Illinois, Minnesota, and the District of Columbia.54 It looks first at who qualifies to receive these services and then at the array of services they qualify for. Understanding who qualifies and what they qualify for is important because different levels of functional impairment are needed to qualify for different levels of service. After a brief general description of the factors that go into determining who qualifies, we examine the most common levels of care and the level of impairment they are designed to address.
5.2. Who Qualifies for Medicaid Mental Health Services?
Community-based mental health services, as used in this report, are a range of services that are part of a system of treatment and support for people with mental health disorders that enable them to live stably in the community.55 Given our focus on services for people living in PSH, this most often means services that are included in Medicaid state plans under the rehabilitative services and targeted case management options. In addition, some states cover some of these services as optional state plan home and community-based services, which may include habilitation, psychosocial rehabilitation, case management/service coordination, housing locator services, and other services and supports for community integration.
| Level of Care Utilization System (LOCUS) |
|---|
The LOCUS assesses 7 domains, using 5point scales for which a higher score indicates greater need for assistance:
The assessor rates a person on each domain and then adds up the scores to get a global score. States that use rating scales vary in the number of levels of care they define and how they match LOCUS or GAF scores to those levels. Levels may be called "tiers," "levels," or states may simply associate a global LOCUS score or range of scores with particular services. |
In Minnesota, the LOCUS score is converted to a level of care recommendation. Assertive Community Treatment services may be authorized for a person whose needs are at level 4, while less-intensive Adult Rehabilitative Mental Health Services can be authorized for a person whose needs are at level 3 or level 2.
- Multiple and frequent psychiatric inpatient re-admissions, including long-term hospitalizations.
- Excessive use of crisis/emergency services with failed linkages.
- Chronic homelessness.
- Repeated arrest and incarceration.
- History of inadequate follow-through with elements of a treatment plan related to risk factors, including lack of follow-through taking medications, following a crisis plan, or achieving stable housing.
- High use of detoxification services (e.g., two or more episodes per year).
- Medication resistance due to intolerable side effects or illness that interferes with consistent selfmanagement of medications.
- Clinical evidence of suicidal ideation or gesture within the last three months.
- Ongoing inappropriate public behavior within the last three months, such as public intoxication, indecency, disturbing the peace, and delinquent behavior.
- Self-harm or threats of harm to others within the last three months.
- Evidence of significant complications, such as cognitive impairment, behavioral problems, or medical problems.57
These criteria and others used in defining eligibility for Medicaid-covered mental health services in Illinois incorporate some of the characteristics of the most vulnerable people experiencing chronic homelessness and help to target intensive, team-based clinical and rehabilitative services to this group of people.
5.3. What Services Do They Qualify For?
- Services providers have frequent face-to-face contact with clients, and mental health workers or teams have relatively small caseloads. Service providers often meet with clients several times a month, and can see clients more frequently if needed.
- Services are often delivered in a range of community settings outside of clinics or program offices, including home visits.
- Service providers reach out assertively to engage with clients, particularly during a crisis, relapse, or transition (e.g., from homelessness into housing, or after a hospitalization).
- Services are individualized and flexible, based on the needs, strengths, and goals of the client.
- Services are expected to continue for many months, or for years, to support ongoing recovery and stability, while the frequency of contact and the client's goals or focus of service interventions may change over time.
- State and local mental health systems use different terms to describe these models of service, which are generally more-intensive than other community-based mental health services.59 The five case study sites that used Medicaid to cover community-based mental health services for people experiencing homelessness or living in PSH during the study period gave the following names to their program or service models that are most often linked to PSH:
- Assertive Community Treatment teams in Illinois, the District of Columbia, Louisiana, and Minnesota.
- Full Service Partnerships in California.
- Field Capable Clinical Services in Los Angeles.
- Community Support Services or Community Support Teams in Illinois and the District of Columbia.
- Adult Rehabilitative Mental Health Services in Minnesota.
- Community Psychiatric Support and Treatment in Louisiana.
The states of interest in this chapter all provide coverage for some or most of the costs associated with these service models using state or county funding. For Medicaid recipients, the states have used the Medicaid Rehabilitative services option to a greater or lesser extent to cover part of the cost, depending on the alignment between the service models and covered services in the state's Medicaid plan.60 Some states may also cover targeted case management services under their Medicaid state plan.
- Treatment includes psychopharmacologic treatment, including new atypical anti-psychotic and antidepressant medications; individual supportive therapy, mobile crisis intervention, and substance use disorder treatment for those with a co-occurring disorder.
- Rehabilitation includes behaviorally oriented skill-teaching, including structuring time and handling activities of daily living, and support for employment or resuming education.
- Support services include support, education, and skill-teaching to family members; collaboration with families and assistance to clients with children; and direct support to help clients obtain legal and advocacy services, financial support, supportive housing, money-management services, and transportation.
- Comprehensive assessment and periodic reassessment of individual needs, to determine the need for any medical, educational, social or other services. These assessment activities include:
- taking client history;
- identifying the individual's needs and completing related documentation; and
- gathering information from other sources, such as family members, medical providers, social workers, and educators (if necessary), to form a complete assessment of the eligible individual.
- Development (and periodic revision) of a specific care plan that is based on the information collected through the assessment that:
- specifies the goals and actions to address the medical, social, educational, and other services needed by the individual;
- includes activities such as ensuring the active participation of the eligible individual, and working with the individual (or the individual's authorized health care decision maker) and others to develop those goals; and
- identifies a course of action to respond to the assessed needs of the eligible individual.
- Referral and related activities (such as scheduling appointments for the individual) to help the eligible individual obtain needed services, including:
- activities that help link the individual with medical, social, educational providers, or other programs and services that are capable of providing needed services to address identified needs and achieve goals specified in the care plan.
- Monitoring and follow-up activities, including:
- activities and contacts that are necessary to ensure the care plan is implemented and adequately addresses the eligible individual's needs, and which may be with the individual, family members, service providers, or other entities or individuals and conducted as frequently as necessary, and including at least one annual monitoring, to determine whether the following conditions are met:
- Services are being furnished in accordance with the individual's care plan.
- Services in the care plan are adequate.
- Changes in the needs or status of the individual are reflected in the care plan.
- Monitoring and follow-up activities include making necessary adjustments in the care plan and service arrangements with providers.
- activities and contacts that are necessary to ensure the care plan is implemented and adequately addresses the eligible individual's needs, and which may be with the individual, family members, service providers, or other entities or individuals and conducted as frequently as necessary, and including at least one annual monitoring, to determine whether the following conditions are met:
5.4. How Are Services Linked to Housing?
In our case study sites, the agencies providing community-based mental health care (described in Section 5.3 of this chapter) to people who are chronically homeless with mental illness are involved with housing in several ways. The agencies themselves may offer the housing as well as the service component of PSH, they may partner with housing developers and providers so that together they offer the mix of housing and supports needed for PSH tenants, or they may provide mental health services to people residing in PSH without having formal, ongoing partnership arrangements with the agency offering the housing. Likewise, the state departments of mental health for these sites play various roles, which we describe here.
5.4.1. State Department of Mental Health Contributions to the Housing Component of PSH
In our case study sites, state departments with responsibilities for people with mental illness are involved in the housing component of PSH in several ways. They may pay the capital costs of developing the housing, cover part of the operating costs through rent subsidies, and/or develop partnerships with other public agencies to facilitate housing development and operations or to link services with tenant-based rent subsidies administered by public housing authorities. Most of the housing units that serve mental health agency clients who have experienced homelessness operate as PSH and include supportive services that help people retain their housing.
Creating the Housing
In some of our case study sites, state mental health agencies have been developing PSH for their clients, using funds under their control for the capital outlays. In the District of Columbia, the Department of Mental Health has partnered with the Department of Housing and Community Development to participate in the latter agency's semi-annual requests for proposals to develop affordable housing. The Department of Mental Health has assigned several million dollars to these requests, which are producing hundreds of PSH units mixed with other units in affordable housing developments.
In Los Angeles, the Los Angeles County Department of Mental Health has used funds made available through the state's Mental Health Services Act (MHSA) to help pay for more than 1,300 units of PSH for people experiencing homelessness who have a serious mental illness. The county's Mental Health Services Housing Trust Fund provides funding for services in PSH, and the county also assigns MHSA Housing Program funds to the California Housing Finance Agency, which administers those funds for capital and operating costs in affordable housing projects that include PSH units.68 All of the PSH tenants are linked to Department of Mental Health services, and most participate in Full Service Partnership or Field Capable Clinical Services.
One of our other case study sites, Connecticut, is not otherwise being discussed in this chapter because it does not use Medicaid to support the services component of PSH, but this is because the state has paid for a comprehensive PSH program since 1994 that uses state dollars to cover all three PSH cost components--capital, operating, and services. Capital funding comes through the state housing finance agency, while operating and service funding come through the Department of Mental Health and Addiction Services, with additional support from the federal Shelter + Care rental subsidy program. An important difference with the Connecticut PSH tied to early waves of the state program is that tenants do not have to be Department of Mental Health and Addiction Services clients or have SMI or SPMI--they just have to be homeless or at risk of homelessness.
Subsidizing Rents
The way that Connecticut's Department of Mental Health and Addiction Services covers rent subsidies and other operating costs under the state's PSH programs is described above. In the District of Columbia, the Department of Mental Health commits its own funds to subsidize housing for its clients and also negotiates with other agencies for rent subsidies, as described below.
Minnesota's Department of Human Services administers a state-funded program called Group Residential Housing, which provides an income supplement program to pay room and board costs for low-income adults who reside in designated types of settings. The program serves people with mental illness and also includes people with physical disabilities or substance use disorders. The funds can be used to subsidize rents or operating costs for PSH and for some other types of group housing. Some housing settings, including many site-based PSH programs, are registered Housing with Services programs, and these receive a supplemental service rate to cover the costs of supportive services. The program we have been studying in Louisiana, the state's post-Katrina Permanent Supportive Housing Program, also provides rent subsidies using special federal appropriations of Shelter + Care certificates and Housing Choice Vouchers that can be used only for program clients. In addition to these post-Katrina rent subsidies, the program is incorporating other rent subsidy opportunities as they arise.
Partnering to Expand Resources
The District of Columbia Department of Mental Health's collaboration with the Department of Housing and Community Development to create PSH was described earlier in this section. The Department of Mental Health also works with the DC Housing Authority to obtain rent subsidy resources for its clients, including an allocation of tenant-based Housing Choice Vouchers as well as local rent subsidies from the Local Rent Subsidy Program managed by the DC Housing Authority.
In Los Angeles, the County Department of Mental Health partners with the Housing Authority of the City of Los Angeles and the Housing Authority of the County of Los Angeles to use Housing Choice Vouchers that those agencies have set aside through limited preferences and made available to people experiencing homelessness who are clients of the County Department of Mental Health and its contract providers. To achieve the goal of reducing chronic homelessness in Los Angeles County, eligibility for most of these vouchers is now limited to persons experiencing chronic homelessness. The City of Los Angeles Housing Department created a program that funds both capital and operating costs for PSH development through a single application.
The collapse of the housing market and freeze on capital financing that started in about 2008 threatened continuing development of PSH funded through various public funding streams. City and county housing and mental health agencies have worked together to save several projects, applying funds from one or another agency as needed and available to keep construction or renovation going--even if some of the funds were originally allocated to operations--and committing to provide the operating funds once the projects were open and occupied.
5.4.2. Models of Housing-Service Connection at the Provider Level
This section describes the ways that Medicaid-reimbursable supportive services and housing come together to help people experiencing chronic homelessness obtain and keep housing and access the health and behavioral health services they need. We organize this section by type of housing-service arrangement, noting specific instances from our case study sites where the various alternatives for Medicaid payments are being used. We start with what is available for people who are still homeless, followed by arrangements available once people are in housing.
Outreach and Engagement
An activity most needed early on but least likely to come within the Medicaid purview is finding people; working to develop their trust; completing the procedures that will ultimately qualify them for housing, such as landlord and housing authority applications; and working with them to find, lease, and move into a housing unit.
At the time of the outreach staff's initial encounter, the people experiencing chronic homelessness are not enrolled in Medicaid. The process of helping them enroll can be long and arduous, involving as it did in most states during the years of our case studies first becoming an SSI beneficiary. Our sites covered the expense of conducting these activities in various ways, including through contracts with public agencies that use state or county general funds or other tax revenues, SAMHSA's Projects for Assistance in Transition from Homelessness (PATH) program, federal block grants or other federal grant programs, foundation grants, and agency direct fundraising. In Chicago, for example, Heartland Health Outreach's staff is supported by a PATH grant, and they perform a lot of the agency's outreach and engagement work with people experiencing homelessness, remaining with a client until the client qualifies for Medicaid. In past years, the Illinois Department of Mental Health provided flexible state funds that could cover the costs of outreach and engagement while mental health providers worked to help people establish eligibility for Medicaid, but these state funds had just been eliminated when our project began in 2010.
One Agency Provides Both Housing and Services
Sometimes the same agency offers both housing and the voluntary Medicaid-reimbursable services. For project-based PSH, that agency operates the housing directly and the operations staff are agency employees. With scattered-site PSH, the agency controls the rent subsidies (usually Shelter + Care or Housing Choice Vouchers) and works with many different private landlords to assure that its clients can obtain housing and remain stably housed.
Many mental health service providers in Los Angeles County, Chicago, Hennepin County, and elsewhere in the country have developed project-based PSH to serve their homeless clients, all of whom are people with serious or severe and persistent mental illness. In Chicago, most behavioral health agencies that provide PSH have begun requiring that new clients already be eligible for mental health services, which the agencies couple with housing placement to provide the complete PSH package. In Los Angeles, these clients do not need to be Medicaid beneficiaries to receive the services, thanks to California's Mental Health Services Act funding.
But providers of both housing and services increasingly are focused on serving people who are already Medicaid recipients. Minnesota's early eligibility expansion has made it much easier for people experiencing homelessness to qualify for Medicaid and hence for PSH from providers of this type.
Mental health providers may also have control over tenant-based rent subsidies that they use to help their clients who are already Medicaid recipients to find apartments in the community. The District of Columbia's Pathways to Housing program operates in this way, providing Medicaid-reimbursed Assertive Community Treatment services to chronically homeless clients of the Department of Mental Health and using Shelter + Care and other rent subsidies to move clients into housing. Under Louisiana's Permanent Supportive Housing Program as it operated before the Louisiana Behavioral Health Partnership (see Chapter 6), federal Community Development Block Grant funds were used to pay for the services of Housing Support Teams and Assertive Community Treatment, which helped the program's clients. All became Medicaid providers by 2013, after extensive training and organizational development to meet state Medicaid provider standards. In 2013, these providers began to receive Medicaid reimbursement for eligible services to homeless and formerly homeless clients living in PSH that are included in the state's 1915(i) state plan amendment.
Some PSH Service Providers Are Not Medicaid Providers--and Some People Experiencing Chronic Homelessness Are Not Eligible for the Medicaid Services Most Often Provided in PSH
Some of the PSH providers that have been most active in creating and delivering services in PSH for people experiencing chronic homelessness are not Medicaid service providers. Intending to serve the most vulnerable and chronically homeless people in their communities, many of these PSH providers have not limited eligibility for housing to persons who have a severe mental illness that would qualify them for Medicaid-covered community-based mental health services, which are the PSH services most often covered by Medicaid. As a result, a substantial number of their PSH tenants are probably not currently eligible to receive Medicaid-covered mental health services, although many of these tenants have substance use disorders, cognitive impairments, and histories of trauma that result in similar functional impairments, and they could benefit from individualized and flexible services that are similar to those that Medicaid covers as mental health benefits for persons with SMI.
A 2011 survey of Minnesota's PSH providers found that of 43 PSH providers responding, 32 receive no Medicaid reimbursement for any services for their residents. The remaining 11 agencies are Medicaid providers, but only two reported billing Medicaid for home and community-based services; seven for MH-targeted case management; and eight for Adult Rehabilitative Mental Health Services. Some receive reimbursement for more than one type of care. Only about one in four of the PSH providers responding to the survey in Minnesota seek Medicaid reimbursement directly, and many PSH providers reported that they did not contract or otherwise partner with agencies that are certified to provide Medicaid-reimbursable services.
For people experiencing long-term homelessness, and particularly for those who do not have a serious mental illness but may have other disabling health conditions and/or substance use disorders, many of the services that are critical to helping people get and keep housing are not being paid for through Medicaid. Instead, PSH service providers have relied on other sources of funding, including local resources and time-limited grants, making it difficult to sustain or expand services at the scale needed to provide PSH for more people who are experiencing chronic homelessness. Some types of services are particularly difficult to finance with Medicaid reimbursement. In their responses to the Minnesota survey, nearly all providers indicated that they were not receiving Medicaid reimbursement for outreach, engagement, harm reduction services, housing supports, and psychotropic medications management.
It should be noted that this survey of PSH providers was done before the state's early expansion of Medicaid eligibility was fully implemented (enrollment began on March 1, 2011). So the situation with regard to Medicaid enrollment of PSH tenants is likely to have changed significantly since the survey was completed. Eligibility for certain mental health and supportive services would not have changed as much, however, since that would still depend on meeting medical necessity criteria, and the agencies themselves would still have had to become Medicaid providers or to partner with agencies that are certified to deliver the relevant services.
Housing and Service Providers in Partnership
This is a common form of PSH, with many examples in all of our case study sites. Many of these arrangements involve agencies on the service side that are not Medicaid providers, but some examples of partnerships involve a service partner with some capacity to use Medicaid financing:
In Chicago, Heartland Health Outreach (a Health Center) collaborates with Mercy Housing Lakefront to provide on-site health clinics in PSH and also links tenants seen in those housing-based clinics to Heartland Health Outreach's main clinic for ongoing care and treatment. These services are Medicaid-reimbursable if clients are enrolled in Medicaid.
In Los Angeles, A Community of Friends (a housing provider) has arrangements with various providers of Medicaid-reimbursable and county-funded mental health services for supports to tenants in its many buildings.
Also in Los Angeles, Skid Row Housing Trust has arrangements with JWCH's Center for Community Health and Los Angeles Christian Health Center (both Health Centers) as well as Exodus Recovery and LAMP (mental health providers), among others, to serve its tenants.
Tenants Obtain Services Independent of their Housing Provider
In the model of care in which tenants obtain services on their own, the supportive housing provider may only accept tenants who are already connected to services and thus come with their own service provider. Others may offer housing to eligible applicants who do not have established connections to services and work with them to get them connected to whatever services they qualify for.
One agency in Los Angeles County exemplifies the former approach. It operates two site-based PSH developments and scattered-site PSH using vouchers. All tenants "are clients of something," the program administrator explained, whether they receive services from the organization that operates the PSH or another mental health service provider in the area.69 The agency will not accept a tenant into its housing unless the person already has access to mental health services. That said, the services in question are voluntary; they are usually either Full Service Partnership or Field Capable Clinical Services, which operate on the premise that clients may refuse to participate in particular services at particular times.
To have access to the PSH units that the Los Angeles County Department of Mental Health helped create with Mental Health Services Act funding, including both site-based PSH and scattered-site PSH implemented through partnerships with local housing authorities, a person experiencing chronic homelessness must first be enrolled in a service program that can access Medicaid reimbursement and/or funding from other revenues administered by the county. The department helps people who are chronically homeless get connected to services in the county's mental health system first, which in turn provides the support needed to help people get and keep housing, submit successful applications for SSI, and achieve other goals.
The Department of Mental Health uses this approach because it does not provide funding that is specifically designated for services to PSH tenants, but instead creates PSH by connecting the services funded through its existing programs and contracts to either site-based housing units or vouchers for use in scattered-site units. Many of these service programs, particularly those funded through the Mental Health Services Act, have incorporated low-demand, housing-first strategies and do not require that people experiencing homelessness comply with strict program rules or achieve sobriety before they can get housed. The agency's approach, however, generally requires that people experiencing chronic homelessness establish some connection to mental health services before they are offered housing assistance through the resources controlled by the Department of Mental Health.
5.5. Payment Structures and Administrative Challenges
Many issues related to payment surfaced during the case studies. These related mainly to what aspects of the supports needed by people experiencing chronic homelessness and PSH tenants the Medicaid arrangements available during the study period (2010-2012) would and would not pay for. However, providers also described issues with respect to the mechanisms for getting paid.
The issues in each of these areas were quite common across case study sites. We describe them and offer one or two examples of each, though examples could be multiplied for every site.
5.5.1. PSH Service Providers' Concerns
Providers offering Medicaid-reimbursable community-based mental health services (defined in Section 5.2, above) all note that Medicaid does not cover all, or even most, of the activities associated with delivering the services and supports that are part of effective PSH programs for people experiencing chronic homelessness.
The Front End--Engaging People and Helping Them Qualify for Medicaid
In states using Medicaid's rehabilitative services option or targeted case management services benefit to fund services for people experiencing homelessness with SMI--which include California, the District of Columbia, Minnesota, and Illinois--Medicaid will not pay for the work needed to find and engage potential clients. Medicaid does not pay for the period of engagement and assessment that must occur while working to enroll a person in Medicaid. After a person is enrolled in Medicaid, targeted case management benefits can cover some of the activities related to helping a homeless person apply for housing assistance, move into housing, and get connected to services.
As we heard in all case study sites, engaging people experiencing homelessness often takes prolonged outreach efforts, with patient, nonjudgmental relationship-building through conversations and offering practical support or help to meet immediate needs when people experiencing homelessness are not interested in mental health or substance use disorder treatment. This can take months and sometimes years. As one provider says "we start with their ouch." Assessment can happen over time and may involve different team members asking questions, such as asking a homeless person to "tell me about your life," and putting pieces of information together to make a complete picture. When trust has been developed, the person may be more willing to sign forms to provide consent to release information, allowing the provider to access county records of previous hospitalizations or other treatment history needed to establish eligibility for Medicaid-covered services and benefits. During this time service providers cannot bill for any Medicaid-covered services. HUD, SAMHSA, or local funding is often used to cover the costs of services before a person becomes a Medicaid beneficiary and is enrolled in the mental health system.
While Medicaid cannot cover outreach and engagement activities needed to help a person establish eligibility and become a beneficiary, the process of enrolling in Medicaid became a lot easier on January 1, 2014, in states going forward with Medicaid expansion on the basis of income. It may eventually be possible for agencies helping people experiencing chronic homelessness enroll in Medicaid to get reimbursed through Medicaid for the work they do with newly enrolled clients to stabilize their health and behavioral health conditions and help them find housing. For this to happen, the agency would have to be a Medicaid provider and medical necessity would have to be established for the particular client and specific services.
Limitations on Reimbursement for Some Services and Activities
For some services covered under the rehabilitative services option, payment may be available only for face-to-face interactions with the client. Generally in these situations, no payment is provided for the time providers spend searching for a client, attempting to visit when the client is not at home, or waiting for the client. In some cases, states may adjust payment rates for services that are delivered "off-site" (outside of an office or program site) in order to reflect some of the higher costs associated with these services.
For people with behavioral health disorders who have experienced chronic homelessness and those living in PSH, service providers often spend a lot of time waiting--at hospitals, in court (the agency's psychiatrist may go to commitment hearings or other legal proceedings), at a jail, or other venues. Service providers often spend a lot of time traveling to make home visits to people who are living in scattered-site PSH. Generally, Medicaid reimbursement does not cover the time providers spend waiting. Time spent transporting a client to an appointment may be covered only if the provider is using the time to help the client in other ways, for example helping to cope with anxiety or develop skills.
Depending on the state's specific definitions of covered services, activities done on the client's behalf but without the client present--usually called collateral contacts--may or may not be covered as Medicaid benefits. These include setting up medical appointments for the client, checking with health care professionals about the results of those appointments, or interacting with landlords on behalf of the client. In some cases, such collateral contacts may be covered under the rehabilitative services option if the focus of the contact is deemed to be providing advice to a family member or other service provider about how to assist the client or obtaining information that will assist the client in goals related to a treatment plan. Other types of collateral contacts, which often focus on helping the client to get or effectively use other services or benefits such as housing assistance, may be covered as case management services, but only if the state or county offers Medicaid-covered targeted case management services and contracts with the provider to deliver these services.
Medicaid plays an important part in financing services in PSH but it covers only a portion of the activities, and hence the costs, of the services that engage people who are chronically homeless, provide the support needed to link them to housing, and support them in achieving and maintaining stability and recovery. While some states are working to develop and implement definitions of Medicaid services that support recovery and housing stability for people with mental illness, service providers working in PSH say that some of the activities that are necessary for this population do not fit into the definitions of covered service that have been adopted in their states.
Housing-Related Activities. As part of their definitions of services covered under the rehabilitative services option within their Medicaid state plan, some states include much of the work involved with helping clients move into housing and helping them get food, clothing, household items, and other things they need, but many states have not. Also frequently left out of service definitions is ongoing communication with housing providers to negotiate access to housing and to identify and resolve problems that could lead to housing loss.
Exceptions are: (1) the District of Columbia, where both Community Support Services and Assertive Community Treatment include these activities; and (2) Minnesota, where Medicaid targeted case management services include these activities. In California, some of these services are covered as targeted case management in its package of mental health services. Under a 1915(i) home and community-based services state plan amendment, the Louisiana Behavioral Health Partnership (the state's Medicaid managed care plan for behavioral health) covers housing-related services for clients of the Permanent Supportive Housing Program receiving care from either Assertive Community Treatment or Community Psychiatric Care and Treatment teams.
Finding the Client. In addition to the work of engaging clients before they become Medicaid recipients, time spent trying to find people, which can be particularly challenging if they have not yet been housed, is not billable. Travel time is not covered if the client is not at home when the service provider arrives for a home visit. People with chronic patterns of homelessness do not always remember appointments.
Habilitation. Medicaid rehabilitative services are for the restoration of functioning, but many people who are chronically homeless need help to learn new skills for independent living, particularly if they experienced mental illness, substance use disorders, homelessness, victimization, neglect or institutionalization as children or young adults, and never had the opportunity to develop the skills needed to maintain a household, manage a budget, and be responsible tenants. Medicaid-covered targeted case management benefits do not include direct practice to teach or improve client skills (i.e., habilitation). Louisiana's Assertive Community Treatment and Community Psychiatric Support and Treatment services are covered as optional home and community-based services under a 1915(i) state plan amendment, and these services include teaching new skills (habilitation). Going forward, Medicaid's 1915(i) home and community-based services state plan benefits may offer states a good option for covering the range of supportive services that are often needed by people who are living in PSH, because these optional benefits can include habilitative services.
Travel Time with the Client. Transporting clients to doctor's appointments or for housing search is not reimbursable in most case study sites. Some providers reported that they use transportation time to deliver other covered services, such as talking with clients about their service plan and how they are meeting its goals, or helping clients manage anxiety and develop coping skills in preparation for appointments, so that with appropriate documentation some of this time can be billed.
Working with the client on substance use problems directly, without relating substance use to symptoms of a mental illness, may not be reimbursable under benefits defined as mental health services. In California and Illinois, Medicaid-covered substance use benefits include treatment services that are covered only if these services are delivered in locations that are certified as treatment facilities. This is significantly less flexible than the states' Medicaid benefits for mental health services, which can be delivered in a range of settings, including a person's home. To stabilize people with chronic patterns of homelessness in housing, substance use disorder services need to be provided where people live, and at any time that the client is willing to accept and respond to them.
Documentation Requirements for Medicaid Reimbursement
With mental health services authorized under the rehabilitative services option, all care must be justified in terms of its contribution to consumers' rehabilitation or the restoration of functioning that has been impaired by mental illness. We heard about the problems this causes in every case study site, and from virtually every provider. While many mental health service providers are taking steps to integrate attention to health and wellness into their practice, and often adding nurses or health workers to their staff to provide more-integrated care, it can be very difficult for a mental health service provider to get reimbursement for other health-related services.70 If a consumer cuts his arm and needs wound care at home, or needs help to manage his diabetes, the time it takes to clean the wound and put on a bandage or help the client learn to check his blood sugar and make better decisions about diet, nutrition, and reducing alcohol consumption must be justified in words such as "teaching consumer wound care or diabetes selfmanagement as way to reduce anxiety that contributes to exacerbated symptoms of mental illness." Taking the client to a clinic for a medical appointment might be justified only if there is documentation that without assistance, the client might have trouble sitting in the waiting room or communicating appropriately with health care providers because of his delusions or paranoia, and the purpose of accompanying the person to the clinic is to help him with the skills needed to manage those symptoms in a clinic setting. If incorrectly worded, the claim will be denied.
Most states require that for Medicaid to reimburse for a unit of care, the care delivered must relate directly to a goal in a client's treatment plan. These plans must be established at enrollment, so they can only cover what the provider knows about and the client agrees to at that time. Difficulties arise because people's issues may not become clear until service staff have spent some time with them or may fluctuate due to the nature of mental illness. Early on, clients commonly refuse to include certain goals in their treatment plans. Dealing with their substance use is often one of these areas of refusal. Flexibility to change the plan quickly as needs become apparent is important. That flexibility exists in the District of Columbia and is much appreciated by Assertive Community Treatment providers there; some of our other case study sites report having less flexibility, leading to payment difficulties when services are provided for changing client needs that do not tie back directly to goals in the service plan.
Proper justification for and documentation of care is so important for ultimately getting paid that many providers offering Medicaid-reimbursable services to PSH tenants and other people experiencing homelessness devote extensive training and staff resources to getting it right. One Los Angeles agency has recently hired a full-time "quality assurance specialist" to help caseworkers get the documentation right and shepherd it through the appropriate offices to result in payment. Many agencies devote supervisory time to reviewing case notes and to informal teaching, as well as offering regular training sessions in correct documentation.
Meetings, Care Coordination, and Case Conferencing
The people experiencing chronic homelessness or living in PSH on whom this project focuses have health and behavioral health conditions that interact and interfere with functioning in complex ways. In addition, their homelessness needs to be addressed, and their success in using health care appropriately depends on their achieving housing stability. Care coordination is essential for this population. Yet time and again, in all case study sites and from virtually all providers, we heard that in their states Medicaid reimbursement did not pay for the time to do this coordination, case conferencing, and even simple staff meetings.
Los Angeles PSH service providers and people working in county government to align resources for supportive services with housing for people who are chronically homeless often identified care coordination as the biggest gap in funding for PSH and the biggest obstacle to achieving the goal of ending chronic homelessness in Los Angeles. They put the issue this way:
There are no resources to cover care coordination that works to facilitate access to and integration of medical, behavioral health, and social services for people with complex needs, nor is there coverage for "housing case management" services that focus on keeping very vulnerable people who are chronically homeless in housing and helping them to follow prescribed regimens. These services are needed, but Medicaid reimbursement under current rules generally does not cover them and [Los Angeles County] does not have a designated source of funding to pay for them.
Care coordination could be approvable as part of another state plan service. For example, care coordination under the rehabilitative services benefit would include coordination of and referral to needed mental health or behavioral health services. This is a more narrowly defined service than targeted case management, which aims to assist individuals with accessing all needed services.
Case conferencing may also be reimbursable as a part of targeted case management if it is for the purpose of developing or revising the care plan. Alternatively, states could build some costs into the service rate, including costs associated with case conferencing and staff meetings.
5.5.2. Services Integration
An important premise of the Affordable Care Act is that the twin goals of improving health and reducing unnecessary spending can often be served best by coordinating care for the most vulnerable people--those with disabilities and multiple chronic health conditions, often complicated by social isolation. The idea is to "treat the whole person" by assuring that providers helping clients with acute and chronic physical health conditions, mental health issues, and substance use problems work together as members of integrated, multidisciplinary teams while also appreciating that the clients' housing situation and other social determinants of health have a significant impact on treatment outcomes. The most innovative models of care for people with complex conditions call for this type of care coordination and attention to housing stability and social supports. Integrated approaches have certainly proven effective for the population on which this report focuses.
Most Medicaid state plan provisions that govern mental health services were written well before the "whole person" concept emerged, however, with the result that covering the coordination activities that make these innovative models work has often proved challenging. The two accountable care or integrated service/care coordination models we highlight in Chapter 7 are designed to overcome this challenge. Before describing them, however, it is important to appreciate the range of issues we are talking about.
Outdated Service Definitions. The longer it has been since a state revised its definitions of Medicaid-covered mental health services, the more likely it is that the most innovative providers will have difficulties matching what their model requires they do to the service definitions that govern claim reimbursement.
Silos. Policymakers and providers cited numerous instances in which they had to deal with diverging service definitions, provider certification requirements, care delivery locations and circumstances, and modes of contracting established by various single-focus state agencies (e.g., mental health, substance use services). In many cases, the state Medicaid agency has delegated to other departments of state government much of the responsibility for determining aspects of the Medicaid program pertinent to the departments' areas of responsibility. These service silos make it difficult to deliver and get reimbursed for integrated care for people with multiple co-occurring conditions.
Data Systems. Providers often reported that each state or county agency they deal with requires that providers use its data system. Therefore, when a provider manages to access multiple types of funding, including Medicaid reimbursement, to deliver multiple types of service for its clients, it has to do double and sometimes triple data entry, usually with slightly different fields and data definitions. Further, providers report that data systems from these public funding agencies are frequently antiquated, difficult to access, difficult to use, and difficult to extract performance data from for a provider's own use. As providers are implementing new technology for electronic health records, most of those who were interviewed as part of this case study indicated that they have been unable to find products that integrate information about health care, behavioral health services, and other supports needed to provide comprehensive and coordinated care for people with the most complex needs. As a result, even when they are adopting new technology, they often find themselves maintaining parallel systems.
Privacy Rules and Data Sharing Restrictions. Public agencies and systems of care almost always have their own data privacy rules, often based on federal or state requirements and/or legislation, that make it difficult to share data across systems to promote integrated client care. Some things may be changing on this front because of the changes in types of data, data access, and data systems that states are developing to comply with various aspects of the Affordable Care Act.
Audit Functions. Respondents in case study sites noted instances in which state auditors interpreted program rules that govern separate Medicaid benefits for health care, mental health, and substance use disorder services or allowable costs for categorical programs in ways that did not seem to take into consideration best practice models of integrated care. For instance, an audit of a community clinic delivering integrated primary care and behavioral health services might disallow costs for staff positions that provide case management services or peer support that would be recognized as a standard part of the staffing model for community behavioral health services. In some cases this may be a result of auditors relying on outdated service definitions that have not been revised to reflect new models of care, or an outdated understanding of practice models that could be covered under the definitions of covered benefits.
Case conferencing and care coordination are ways that agencies try to assure services integration for their clients. Many providers believe it would help to facilitate and cover the costs of better care if these activities were included in definitions of Medicaid-covered services. It would also make a considerable difference if the various agencies that govern health care and behavioral health services worked together to better align their requirements and to reduce reporting burdens for providers who are trying to work in an integrated manner to address all of their clients' health and behavioral health needs.
Mental Health Versus Substance Use Disorder Services
Illinois and California provide good illustrations of the difficulties for providers and clients when the rules of mental health and addiction treatment agencies are not aligned to facilitate the delivery of integrated care for co-occurring disorders.71
Illinois funds many community-based mental health services that are covered under Medicaid's rehabilitative services option through the Department of Mental Health's Rule 132, and Medicaid-reimbursable substance use disorder services under the Department of Human Services' Division of Alcoholism and Substance Abuse. Providers of services in PSH reported significant difficulties when trying to coordinate these Medicaid benefits to serve people experiencing homelessness and PSH tenants who have co-occurring mental illness and substance use disorders. The two agencies have different requirements for just about everything, such as time frames for treatment planning and follow-up, allowable treatment types, and amounts and lengths of treatment. To cope with these differences and because it wanted to be able to offer its consumers integrated services, one agency, Heartland Health Outreach, created a crosswalk of rules and developed an integrated assessment and service planning tool that complies with all rules and allows Heartland Health Outreach to serve a target population of homeless people severely impacted by two or more chronic and disabling conditions.
One aspect of the different requirements is particularly relevant for agencies working with people who have been homeless a long time and who have both mental health and substance use disorders. Most Division of Alcoholism and Substance Abuse funding only covers care delivered in a treatment facility licensed by the Division of Alcoholism and Substance Abuse. Rule 132/Medicaid Rehabilitation Option care, in contrast, is heavily oriented toward services delivered in the community, mostly in people's homes. When PSH residents need and want substance use related services, they must go to a treatment facility to get them, while staff offering mental health services may come to where the clients live. Many agencies in Chicago's homeless assistance network may serve people with co-occurring mental illness and substance use disorders, but very few of them have a Division of Alcoholism and Substance Abuse facility license that allows them to deliver Medicaid-reimbursed substance use disorder treatment services. Mental health providers that see a lot of people with co-occurring substance use disorders try to offer some services to meet their needs but find themselves hard pressed to cover the cost. As a result, many mental health agencies have limited capacity to deliver integrated care for people with the most severe substance use disorders.
California's Medicaid-covered benefits to address mental health and substance use disorders are similarly defined separately, and these benefits have been administered separately not only at the state but also at the county level. While some California counties have created departments of behavioral care to administer both mental health and substance use disorder services, in Los Angeles County, one department administers mental health services while another administers substance use treatment services, including services that are covered by Medicaid. These benefits and treatment programs are usually not integrated or well-coordinated with each other or with other Medicaid-covered health care. As is true in Illinois, California has provided a limited package of Medicaid-covered benefits to address substance use problems and requires that nearly all of these services be provided in licensed treatment facilities to qualify for Medicaid reimbursement.72 For people with histories of chronic homelessness who live in PSH, the services that are often most needed focus on reducing harmful substance use and intervening quickly during times of relapse use to reduce problem behavior and avoid crises that could lead to the loss of housing. These services, which facilitate change and support recovery, are delivered in the person's home or elsewhere in the community but not in a certified treatment facility. Medicaid coverage for substance use services would be available only when tenants are willing and able to enroll in a treatment program and participate in services delivered in certified treatment locations. Medicaid reimbursement is not currently available for the service activities that are frequently a part of the PSH service model, including motivational interviewing, substance use disorder recovery support groups that meet on-site in PSH, individual counseling and coaching to support recovery and relapse prevention, and other services that may be integrated into the delivery of primary care or mental health services for PSH tenants.
5.5.3. Getting Paid
Rates
We sometimes heard during site visits that reimbursement rates for the services needed by people with patterns of chronic homelessness were too low. Several Minnesota providers dropped Adult Rehabilitative Mental Health Services-funded programs for this reason. In the District of Columbia, the Department of Mental Health found that it would have to raise its Assertive Community Treatment rates to get any agency to provide the service. In 2008, the agency committed to expanding these services from somewhat fewer than 400 people to about 1,200 people. It offered contracts but got no takers. In addition, Pathways-DC had already informed the Department of Mental Health that it could no longer afford to provide Assertive Community Treatment services at the current rate. Working with the District of Columbia's Medicaid agency, the Department of Mental Health increased the reimbursement rate per increment of time by 25 percent, using its own departmental funds for the state match. This level of funding proved to be sufficient to keep Pathways-DC in business and attract new providers. Also in the District of Columbia, however, some mental health providers will not take people enrolled in certain Medicaid managed care plans because the plans' reimbursement rates for mental health services are too low.
Payment Methods and Limitations
Payment structures varied across our case study sites and also within each site depending on the type of services provided. Medicaid reimbursement for most of the PSH services that are covered as mental health benefits in our case study sites is based on claiming (or billing) for covered services in 15minute increments. Targeted case management services in Minnesota have a per-person permonth payment structure.
Illinois providers note that, as clients continue to need supports that vary over time but do not reliably dwindle to nothing, the state Medicaid office gives their requests for payment or authorization for continued services increasing scrutiny. In response to budget limitations, systems have been put in place to manage utilization of the most-intensive and costly services and to encourage transitioning people to lower, less costly levels of care when possible. Further, some types of care have limits on the units of service that can be supplied, and these limits are sometimes considerably lower than the clients with complex needs require (e.g., five hours of case management a month when providers say that it takes 20 hours to really help some clients). Providers in other states also reported unit-of-service limitations that are not realistic, given the needs of people who have experienced chronic homelessness.
The District of Columbia's Assertive Community Treatment teams are paid at a rate established by the Department of Mental Health for each 15-minute increment of time spent with a client. Unlike the situation in many states, however, there is no limit on the number of service units that team members may spend with clients and be reimbursed for. If a staff person spends two hours with a client, Medicaid would cover all eight 15-minute service units. The Pathways-DC director feels that this is preferable to a payment structure that offers a fixed monthly rate for program participants, which has been used in some states for ACT programs, because it allows for additional reimbursement when serving clients who need more-intensive services and supports.
Service providers in other communities frequently complained about the burdens associated with documenting all covered services in 15-minute increments. They often said that they find it very challenging to reconcile billing and documentation requirements with the expectation for "doing whatever it takes" to engage with and connect the most vulnerable people to housing and to deliver flexible, client-centered care to support stability. Many of these providers told us that they believed that a monthly per-member rate, or a set of rates that could be adjusted for clients in need of varying levels of support, would be a more appropriate payment mechanism for the moderate level of services delivered by Community Support Teams and the more-intensive models of care such as Assertive Community Treatment. They believe that monthly rates covering a flexible package of services would allow service providers to spend more time providing direct services for clients and coordinating their care and less time with paperwork.
Knowing How to Bill
We did not interview many agencies in our case study sites that had recently become Medicaid providers, so we do not know if issues related to learning billing procedures, submitting forms, and knowing timing are widespread. The clearest discussions we had with behavioral health providers new to Medicaid were in Los Angeles.
The Los Angeles County Department of Mental Health has provided some training for contract providers related to documentation and billing requirements to get Medicaid reimbursement for services to people who are homeless or leaving homelessness, including the outreach, engagement, and housing-related services that are included in the county's coverage for both moderate and intensive service levels. But service agencies new to using Medicaid or trying to figure out how to comply with service planning and documentation requirements say that they have a hard time finding this guidance. Neither the state nor the county Department of Mental Health had provided systematic guidance about how to obtain Medicaid reimbursement for flexible, client-centered, and multidisciplinary team models of service, even though the county agency funded several demonstration projects with just these configurations and goals in 2011.
Service agencies that are becoming Medicaid providers need clear guidance that is accessible and welldocumented to help build staff capacity and implement systems that meet Medicaid requirements for service plans, case notes, billing, and other documentation. One provider said that "myth buster" guidance from CMS is needed.
Reimbursement for Services
Reimbursement to providers for Medicaid services comes after the services are provided. The time lag between an agency paying its staff to help a client and receiving reimbursement for the cost of that care can be very important. Small nonprofit agencies often do not have the financial resources to front the cost of care that may take months or sometimes years to recover through public payments.
5.6. A Final Note: The District of Columbia Department of Mental Health's Comprehensive Strategy for Expanding Services
The District of Columbia Department of Mental Health (DMH) has made a considerable investment in service expansion, including adding many housing units and other services for its clients who are homeless. Earlier parts of this chapter described the agency's investments in housing and expansion of Assertive Community Treatment services. Here we describe the larger scope of the District of Columbia's mental health services, looking at how the service categories created in 2008 were able to include Assertive Community Treatment and other evidence-based practices to promote community-based care.
Of the nine service categories included in the District of Columbia's Mental Health Rehabilitative Services, three are specifically designed to be delivered in the community (community support, community-based intervention, and Assertive Community Treatment). Two of these, Community Support Services and Assertive Community Treatment, are the services most commonly used with people who are or have been homeless. Specific aspects of the District of Columbia's Assertive Community Treatment services were described earlier, so here we focus on the aspects of its Community Support Services that are relevant to PSH tenants. Community Support Services are intended to help consumers manage the symptoms of their illness sufficiently to adapt to a home environment, manage their finances appropriately (which helps keep the rent paid), maintain independent living, and regain coping skills and strategies to avoid institutionalization and possibly losing their housing.
Four service categories (diagnosis/assessment, medications/somatic treatment, counseling, and crisis/emergency) do not specify a treatment location and thus could occur in the context of the three community-based services as well as in other contexts. Only two categories (day services and intensive day treatment) specify that they must be delivered in a DMH-certified Community Mental Health Rehabilitation Services Agency.
The District of Columbia's Department of Mental Health also recognized that transforming the service delivery system required other actions. In addition to enhancing the Assertive Community Treatment reimbursement rate, specifying Assertive Community Treatment reimbursable services, articulating the certification criteria for agencies offering Assertive Community Treatment services, and expanding the program from three to 12 Assertive Community Treatment teams, the Department of Mental Health contributes to the development of Assertive Community Treatment and other mental health services for high-need populations in several ways.
The department's director describes his agency's strategy for eliciting quality care for clients of Assertive Community Treatment services as follows:
Pick an evidence-based practice that does what you need and that you have confidence can be replicated in your own setting--in this case Assertive Community Treatment.
Write the criteria you will use to certify that an agency is qualified to deliver that practice in a way that supports the fidelity of the practice.
If using contracts, require in contract language that the provider meet the fidelity criteria (but even if you do not do contracts, use the leverage you have through the certification criteria and monitoring practices).
Set rates that will attract providers who can meet and maintain fidelity.
Provide training, initial and ongoing, that moves agencies toward doing the job in a way that meets fidelity criteria.
Provide oversight and accountability; pick a fidelity scale and use it to monitor, in person, against the scale's criteria and also monitor for positive outcomes for clients (the District of Columbia's Department of Mental Health has been doing the former since 2009 and began to do the latter in 2011).
Have a mechanism for enforcing contract provisions; the District of Columbia's Department of Mental Health has two: (1) withholding referrals of new clients for a time until an agency comes into compliance; and (2) decertifying the agency if it continues to resist or remains unable to comply with fidelity criteria.
Having had a lot of experience with Assertive Community Treatment in previous jobs, the director appreciated that an agency new to Assertive Community Treatment would take a while to get up to fidelity standards and that even an experienced agency would need some time for a new team to receive enough client referrals to reach full capacity and be able to sustain itself largely from Medicaid reimbursements. The department estimated that the start-up time for an agency that had never previously done Assertive Community Treatment was 3-6 months. The Pathways-DC director says that, in her experience, it takes a new team in an experienced agency a couple of months to reach self-sustainability, depending on the rate of client referrals to reach 100 clients. That agency also gives a new member of an existing Assertive Community Treatment team a start-up/orientation period of 3-5 weeks that involves shadowing other staff, discussing approaches, and getting explicit training before being expected to pull his or her own weight. During these start-up periods, staff need to be paid, but Medicaid reimbursement does not cover costs for staff orientation.
To cover the start-up period, the Department of Mental Health offered no-interest loans of $175,000-$200,000 to agencies willing to become Assertive Community Treatment providers. These loans were to be paid back as the new agencies could (all have done so). The department also offered, and still provides, training to new and existing providers, via a training contractor.
5.7. Summary
The case study sites in this research provide examples of different approaches for delivering the services that help people with serious mental illnesses experiencing chronic homelessness get and keep housing, and for using Medicaid to pay for the services. Medicaid-covered mental health services that can be covered under the rehabilitative services option and delivered in PSH include, Rehabilitation Mental Health Services, Assertive Community Treatment, and services provided by Community Support Teams. Medicaid's targeted case management benefits also show promise as a way to cover some of the services that help people with SMI, but this approach was only used in two of the case study sites (California and Minnesota). Some of the behavioral health services and supports needed by people living in PSH can be covered as optional state plan home and community-based services under Section 1915(i).
Efforts to use Medicaid to pay for behavioral health services delivered through the program models that have been recognized as best practices for homeless people with co-occurring disorders sometimes run into administrative complexities (data system limitations, conflicting policies/procedures and payment mechanisms across types of services and benefits) and gaps in covered services. State agencies must resolve these challenges if Medicaid is to become a more consistent resource for services to people experiencing homelessness or living in PSH.
6. Medicaid Managed CARE
Chapter 6 Highlights
Medicaid managed care began in many states with a focus on enrolling children and families. However, a growing number of states now allow people with disabilities to enroll in managed care plans, and some states require that most seniors and people with disabilities do so. Among case study sites, California, Illinois, and Minnesota have this requirement for all or many beneficiaries who are seniors and persons with disabilities.
Many states are using managed care plans to provide coverage to people who became newly eligible for Medicaid in 2014 under the terms of the Affordable Care Act, which includes many people experiencing homelessness or living in PSH.
As the shift to managed care happens, it will be essential for many of the organizations that provide Medicaidcovered health services to indigent and homeless people to become part of the health plans' provider networks.
Managed care plans must either deliver care coordination services to their members or contract with other organizations to do so. It is typical for the plans to do nearly all such services by telephone--a practice with severe limitations when working with clients experiencing homelessness and even people living in PSH. As they accommodate to serving members with more complex health and behavioral health conditions, managed care plans are being encouraged to revamp their approach to care coordination for these higherneed members.
Coordination between managed care plans and public mental health departments with regard to shared patients is often quite minimal. One exception among case study sites is Minnesota, where managed care plans under the state's Special Needs Basic Care demonstration are responsible for a range of Medicaid-covered services that includes both medical care and community behavioral health services. Some of these managed care health plans have structured agreements with community-based providers of mental health services, including services linked to PSH, to integrate health-related care management services with the targeted case management services they deliver. These providers receive additional reimbursement for the more-intensive coordination activities involved.
Managed care plans have an incentive to control costs by helping to reduce avoidable hospitalizations or emergency room visits for their members. When the managed care plans receive funding on the basis of capitation, a fixed payment per-member per-month, they may have the flexibility to do some things that could potentially be of great help to members with complex and co-occurring health and behavioral health needs, depending on the specific provisions of a state's Medicaid program and of the contracts between the state and health plans. These include using part of their per-member per-month funding, or their profits, to pay for more-intensive care coordination services if those services are likely to produce better outcomes while reducing the use of other types of services such as inpatient hospital care.
A major issue for managed care plans is rate-setting, specifically being able to negotiate risk-adjusted rates based on the complexity of a member's health status and therefore the intensity of the care coordination needed. Generally states are not using risk-adjustment methodologies that account for the complexity of health needs and the history of service utilization and costs for people experiencing chronic homelessness and others with the most complex health and social support needs.
An example of care coordination in a behavioral health carve-out is Louisiana's Behavioral Health Partnership. Louisiana has undertaken a multiyear, comprehensive redesign of its public behavioral health system for children and adults, requiring numerous waivers and state plan amendments. One of this program's components, authorized under a Section 1915(i) state plan amendment, was designed explicitly to cover the array of behavioral health services needed to help people experiencing homelessness get and keep housing. It is an excellent example of a Medicaid state plan modification that has won CMS approval to have Medicaid cover the care coordination services most needed by people experiencing homelessness and living in PSH.
6.1. Introduction
This chapter begins with a brief overview of developments nationally, then focuses on approaches being used in case study sites. States are increasingly relying on managed care approaches to finance and deliver health care and behavioral health services to people enrolled in Medicaid. Under a managed care approach, states often provide capitated, per-member per-month financing to Managed Care Organizations (MCOs) that in turn contract with health care providers under arrangements intended to reduce costs and increase care quality and coordination.
As states enroll growing numbers of people in Medicaid managed care plans, including PSH tenants and people who are experiencing chronic homelessness, it will be essential for many of the organizations that provide Medicaid-covered health services to indigent and homeless people to become part of the health plans' provider networks. If they do not, they will not be able to obtain Medicaid reimbursement for delivering covered services to plan members. Service providers working to help facilitate access to health care and coordinate care for people who are chronically homeless and PSH tenants will need to understand the impact of managed care enrollment on the services available to their clients and patients.
6.2. How Medicaid Managed Care Is Evolving and What It Means for PSH
- In 2010, California made enrollment into managed care plans mandatory for most seniors and persons with disabilities enrolled in Medicaid in Los Angeles and most other urban counties. The health plans are responsible for managing medical services, while most mental health services and substance use treatment services remain under separate county-administered systems.
- Minnesota state legislation enacted in 2011 requires that people with disabilities be assigned to a Special Needs Basic Care health plan unless individuals opt out of enrollment. These plans are responsible for covering both health and behavioral health services.
- Illinois is taking several approaches to move at least half of all Medicaid beneficiaries into care coordination arrangements, as required by a 2010 state law. The process started with beneficiaries who are seniors or persons with disabilities, for whom managed care entities must provide a benefit package that includes medical and behavioral health services. The first phase began with managed care plans in the "collar counties" that surround the city of Chicago.
- Louisiana has established a statewide behavioral health system of care administered by an MCO responsible for delivering and financing behavioral health care services. Medicaid beneficiaries qualifying for behavioral health services began getting their care through this MCO in phases beginning in March 2012.
- The State of Connecticut has taken a different approach to managing care, creating a self-insured administrative services organization (ASO) for Medicaid-covered health services and a separate ASO for behavioral health services. Both were in the early implementation stages at the end of the study period.
6.3. Seniors and People with Disabilities Moving into Managed Care
We now look at recent developments in enrolling seniors and persons with disabilities into Medicaid managed care and linking them to health services in three of our case study communities--Minnesota, Illinois, and California.
Minnesota
During the time frame of this study (2010-2012), Minnesota saw a significant increase in enrollment in Medicaid managed care plans, as large groups of people moved into managed care or moved from one plan to another as a result of state policy changes. Beginning in January 2012 (with phased-in enrollment during 2012), people with disabilities ages 64 and younger who had been covered by fee-for-service Medicaid were asked to enroll in a managed care health program called Special Needs Basic Care.
Some individuals are excluded from Special Needs Basic Care enrollment, and anyone can choose not to enroll (opt out) and instead stay in fee-for-service (FFS). The state's budget assumptions anticipated that about 50 percent of people would opt out.
The Special Needs Basic Care managed care program was designed for Medicaid-eligible people with disabilities, including those who are dually eligible for Medicare benefits. It began in 2008, with about 6,000 people enrolled in the plans. Under expansion beginning in 2012, enrollment in these plans grew to more than 37,600 people in April 2013.73 The plans are responsible for covering basic health care and most behavioral health care services. Basic health care includes inpatient and emergency hospital care and up to 100 days of nursing home care; behavioral health care services include the targeted case management (TCM) services that are often connected to PSH.
State legislation enacted in 2011 also set targets for reductions in hospital emergency department utilization, rehospitalizations, and inpatient hospital admissions--with penalties and incentives paid for by "withholds" from payments to health plans. The strategy is to withhold a portion of the capitated payment to plans and use the money for incentive payments. The incentive payments and withholds push the plans to focus attention on service strategies that reduce avoidable hospital admissions and re-admissions. These new arrangements are challenging MCOs and provider networks to change their delivery systems to "bend the cost curve."
As Special Needs Basic Care enrollment expansion got under way in Minnesota, some of the agencies serving people who are chronically homeless and PSH tenants were wary, uncertain about how the change from FFS to managed care would impact access to health care for their clients. They were also concerned about effects on payments to mental health service providers who already received Medicaid reimbursement for providing TCM services.74 These concerns proved groundless, however.
Over time many of the mental health service providers who deliver TCM services in PSH have been able to establish contracts with the Special Needs Basic Care health plans, through which they continue to receive reimbursement for these services at monthly rates that are comparable to the rates they had previously negotiated with the counties. One MCO was permitted to establish a three-tiered rate-structure, with higher rates paid for clients who need more frequent intensive services and lower rates paid for clients who need less support. The MCOs also offer transportation to medical appointments, and some also offer fitness, health promotion, nutrition, dental, and care management services for their members, as well as other resources.
Based on our interviews with mental health service providers, the Special Needs Basic Care plans have generally been good for mental health clients, including both people who are currently homeless and PSH tenants. They have added some complexity for provider organizations in MCO contractor service networks, however, because arrangements with each MCO are a little bit different, both in terms of payment to the mental health service providers and the other services available to plan members.
Illinois
In Illinois, state law enacted in 2011 requires that at least 50 percent of Medicaid beneficiaries move into some form of "care coordination" by January 1, 2015. About 2 million people are expected to enroll in some form of care coordination by this date, with about a million people continuing to receive care through FFS arrangements after that time.
The director of the Illinois Department of Healthcare and Family Services (HFS) envisions that the state will develop several different approaches to care coordination. The state's approach includes but is not limited to managed care health plans operated by commercial insurance companies or health maintenance organizations that accept full-risk capitated payments. In addition to these models, Illinois care coordination models also include:
Managed Care Community Networks (MCCNs). Provider-organized entities accepting full-risk capitated payments.
Care Coordination Entities (CCEs). Provider-organized networks providing care coordination for risk-based and performance-based fees, but with medical and other services paid on a feeforservice basis.
The roll-out plan for care coordination began with a focus on seniors and persons with disabilities. This group, comprising16 percent of the Illinois Medicaid population, incurs 55 percent of Medicaid costs. The first phase began in 2011 with the enrollment of seniors and persons with disabilities into traditional managed care plans operated by insurance companies in the "collar counties" surrounding Chicago. HFS selected the first group of six CCEs and MCCNs in late 2012, and began negotiating contracts under the HFS Care Coordination Innovations Project. Implementation of these projects got underway in 2013. The state adopted a plan to expand care coordination through these three models to other population groups and parts of the state during 2013 and 2014.
The early experience with implementing managed care for seniors and persons with disabilities who are Medicaid beneficiaries in the collar counties has been challenging. The two commercial MCOs selected by the state had little experience enrolling and managing care for people with mental illness or other disabilities. The plans have lacked adequate provider networks with the capacity to serve people with behavioral health disorders and in particular to provide integrated services to people who have co-occurring mental health and substance use disorders. So far, agency leaders and other stakeholders report that the commercial managed care plans have not moved far toward changing the delivery system to improve access and health outcomes for seniors and persons with disabilities. Providers who deliver services to people experiencing homelessness in those counties complain that the two MCOs have different and complex billing requirements and procedures for pre-authorization that make working with them difficult.
The state's Care Coordination Innovations Project, launched in 2012, is an ambitious effort by the state and some of its most innovative providers of health care and behavioral health services to create alternative approaches to coordinating and integrating care for some of the costliest and most vulnerable and disabled Medicaid beneficiaries. One of the new CCEs, Togther4Health, has been developed under the leadership of Heartland Health Outreach, a Health Care for the Homeless program, working in partnership with many of Chicago's leading providers of health care and behavioral health services for people who are currently homeless and for PSH tenants. Together4Health will be discussed in the next chapter of this report.
California
In California, the mandatory enrollment of seniors and persons with disabilities into Medicaid managed care plans proceeded rapidly, starting only seven months after the Centers for Medicare and Medicaid Services approved the state's Medicaid waiver request in November 2010. In 16 counties, nearly 240,000 people were required to choose a health plan or have one assigned by the state, and to select a primary care provider or medical home or have one assigned to them. For many people, the assignment process required or resulted in a change in health care providers. The first group was mandatorily enrolled in Medicaid managed care on June 1, 2011, and the transition process was completed in May 2012.75
Health care providers and advocates reported significant challenges with the process of transitioning people with disabilities into managed care.76 Written notices sent to beneficiaries by the state Medicaid office were complex and hard to understand. The notices often failed to reach people because of outdated contact information, and this was particularly a problem for people with chronic patterns of homelessness. Statewide, fewer than half of the beneficiaries chose a health plan, with the rest being assigned to a plan by default.
The California Medicaid managed care plans to which many people were assigned received only limited information about their new members who are seniors and persons with disabilities. LA Care, the largest of the Medicaid managed care plans in Los Angeles County (and the largest public managed care health plan in the country) reported not receiving any claims history data for new members until 8-10 weeks after they were enrolled. At the same time, the plan was required to assign primary care providers to all new members within 24 hours of enrollment, if the new members did not select a provider themselves. Therefore, many assignments were made without knowing where people had been receiving care. The frequent result was confusion among both beneficiaries and health care providers and disruptions in continuity of care.
When a person experiencing homelessness or a PSH tenant seeks medical care from a health care provider located in a shelter or PSH project, or when a health care provider participates in outreach and efforts to engage and serve people experiencing homelessness, the Medicaid managed care plans do not reimburse those providers unless they have been assigned as the primary provider for that person. The providers must request a reassignment, which means that the health plans must commit staff resources to processing reassignment requests.
In addition to problems with enrollment and assignments, the Medicaid managed care plans and provider networks had limited experience serving seniors and persons with disabilities before the rapid expansion of enrollment in 2011 and 2012. Most plans and many of the health care providers who accepted the new group of seniors and persons with disabilities lacked the experience or the capacity to serve people with complex needs that include mental illness and often patterns of homelessness and co-occurring substance use disorders.
6.4. Care Coordination Through Managed Care Organizations
Managed care plans must either deliver care coordination services to their members or contract with other organizations to do so. By care coordination, we mean the health assessment and care management needed by people to address multiple behavioral and physical health needs. This section describes some of the challenges that managed care plans have encountered in serving seniors and persons with disabilities and how those challenges have been overcome.
For those identified as needing care coordination, services may include arranging for specialty care, home health services, and medical equipment such as wheelchairs. Care managers also sometimes provide case management--for example, information about transportation assistance, food programs, and other social services. To the extent the care managers know about housing and shelter options for homeless members, they provide information about them. In Los Angeles, nearly all of these care management services are delivered by telephone, and this is the approach typically used by MCOs. Less frequently, health plans have nurse care managers, social workers, case managers, or patient navigators who deliver face-to-face services to some members who have been identified as "high-risk" because of diagnostic or claims data, including patterns of using hospitals or pharmacy services.
In Los Angeles, LA Care's existing systems of risk assessment and care management had limited capacity to engage and provide the intensive support needed for people with complex health problems and chronic patterns of homelessness. Health risk assessment forms are mailed to individuals upon enrollment into managed care, and LA Care staff attempt to reach people by telephone to complete the assessments. However, response rates are very low. Care management may be offered to a member only if the health assessment is completed and the member is identified as high-risk or if needs are identified at the time of discharge from an inpatient hospitalization or based on other health service utilization data. When a patient is discharged from a hospital, the plan makes three attempts to contact him or her by telephone or mail. Many plan members do not respond to mail or telephone contacts or cannot be reached using the available contact information. Thus LA Care's standard approach is unlikely to identify plan members who are experiencing chronic homelessness or to engage and deliver ongoing care management services to them.
At the time of our visits, very little coordination or information sharing occurred between the care management services offered by Medicaid managed care plans such as LA Care and the services and supports available from the county mental health system for members who have serious mental illness, including PSH and the supportive services that go with it. As the state prepared to implement a demonstration initiative to coordinate care for people who are eligible for benefits through both Medicaid and Medicare, efforts were under way to improve coordination and communication among California's Medicaid managed care plans, including LA Care and county systems responsible for mental health and substance use disorder services.
In Minnesota, the Special Needs Basic Care plans that have enrolled Medicaid seniors and persons with disabilities are responsible for completing comprehensive health assessments and providing care coordination services to help patients get the care they need from primary care providers, specialists, and other health care services. The plans are also responsible for a benefit package that includes targeted case management services for people with serious mental illness.
Some of the Special Needs Basic Care plans have worked with mental health service providers, including those who deliver services in PSH, establishing contracts and sharing training and other resources. The TCM providers also deliver some of the care management services that the health plan's nurse care managers might otherwise do. To build their capacity to deliver this broader scope of services, the mental health service provider organizations have added nurses to their case management teams, trained staff to conduct more comprehensive health assessments, and implemented electronic health records that integrate some medical and behavioral health information. As their roles expand from case management to care management, many staff members must acquire new skills.
For example, Guild, Inc. is a mental health and PSH provider organization that has made a significant investment and organizational commitment to staff training and change management. The organization adjusted its electronic health record system to prompt case managers to ask questions about physical health when they meet with clients. In 2010, staff began to get baseline data on some health indicators, and by the end of 2011 the data showed a big increase in the number of mental health clients who have seen their primary care providers and had physical exams.
One of the Special Needs Basic Care health plans, Medica, provides care management services using a combination of staff (social workers, nurses, and nurse-practitioners) and vendors or partner organizations, including the mental health providers who deliver TCM services in PSH. Medica care coordinators do home visits for some members, in addition to providing services by telephone. Medica care management tools (such as assessment instruments, care plans, and information systems) are shared with the plan's vendors. Medica recognizes that some of these partner organizations have a background in social services but less capacity or experience with medical issues. The Medica nurses and nurse-practitioners are available to these partners to provide clinical consultations or do home visits as needed.
6.5. Medicaid Financing Issues for Managed Care Organizations and Providers
"Full-risk" managed care plans receive funding on the basis of capitation, meaning that the plans are paid a set amount per-member per-month and expected to cover all care needed by their members. Capitation payments may be adjusted based on a variety of factors, including geography (reflecting regional cost variations within a state), characteristics of plan members, and plan performance relative to specified quality metrics or other performance criteria.
Depending on the specific provisions of a state Medicaid plan or waiver and of the contracts between the state and health plans, MCOs may have the flexibility to do some things that could potentially be of great help to members with complex and co-occurring health and behavioral health needs such as those experiencing chronic homelessness or living in PSH. First, they can use capitated funding to pay for care management and also potentially for services that are not easily reimbursable under a fee-for-service system, if these services can produce better health outcomes or control utilization of other more costly services. Some states permit the MCOs to use a share of savings for "re-investment" strategies that can cover some of the costs of innovative care models, if they can achieve savings in other costs.
MCOs can use a portion of their profits to pay for services or activities that are not specifically defined as Medicaid benefits, but generally they must get state approval if they want to use their capitated funding in these ways. Otherwise, without state approval, they may not be permitted to pay for services not covered in a state's Medicaid plan. If states want their MCOs to have the flexibility to pay for services that help achieve savings in costs for avoidable hospitalizations, the states in turn must get CMS approval as part of the terms of a waiver under Section 1115 or 1915(b)(3) before using the Medicaid program to pay for what may be considered "costs not otherwise matchable" (CNOM), including costs of services that are not specifically included in the Medicaid state plan. This creates some uncertainty regarding the degree to which MCOs have flexibility to pay for services in PSH, to the extent some of these services may not be currently defined as covered benefits for some of the people who have experienced chronic homelessness, particularly people without serious mental illness who have been prioritized for PSH because of their vulnerability or frequent and avoidable emergency room visits and hospitalizations.
6.5.1. Risk-Adjustment
Health policy experts have described the importance of "risk-adjustment" in setting capitation rates, meaning that plans (and groups of providers) may receive capitation rates that are adjusted based on characteristics of plan members that predict higher or lower risk for the total costs of delivering appropriate care.77 For example, a health plan or provider network that specializes in serving people who are receiving high-cost care for cancer, AIDS, or liver disease would receive a higher rate per-member per-month, compared with a plan or network that enrolled mostly relatively healthy members for whom expected costs and risks would be lower.
Rates could be adjusted to pay more for health plans or providers who serve people with serious mental illness, including co-occurring substance use disorders, compared with those without behavioral health care needs, based on data that demonstrates higher costs associated with managing chronic illness for people with these added conditions. Some providers who focus on serving people with chronic patterns of homelessness and complex health needs (including those who incur high costs for hospitalizations, emergency room visits, and stays in nursing homes) would like to be able to use risk-adjusted capitation rates to serve vulnerable people with the greatest needs and create incentives for improving the quality and efficiency of care for them.
The state Medicaid agency staff interviewed as part of this study explained that current approaches to risk-adjustment are far from ideal. Often, they take into consideration only a few variables that are easy to track in Medicaid data such as age, gender, home address (to reflect regional cost variations), and whether a person is receiving Supplemental Security Income (SSI) benefits, nursing home care, or home and community-based services (HCBS) that may be available through a Medicaid waiver. State Medicaid staff say that these factors predict only a small fraction of the variation in costs among Medicaid beneficiaries. Important factors omitted from current risk-adjustment practices include service utilization or claims history, social determinants of health such as deep poverty and homelessness, or the complexity of and interactions among a beneficiary's health conditions.
Data provided by the Illinois Medicaid program show that about 3 percent of people enrolled in that state's program receive health care services associated with about 50 percent of total Medicaid expenses, and 20 percent of all expenses are associated with care for only 0.5 percent of beneficiaries. For this small group, costs averaged more than $100,000 per person in 2011. Meanwhile 74 percent of Medicaid beneficiaries received services with average costs of less than $500 in the same year.
With better risk-adjustment, a program that targets services to people in the top cost deciles would receive funding at a rate significantly higher than the amount paid to a program serving primarily people with lower anticipated costs.
Managed care plan administrators are concerned about "adverse selection"--meaning that if they develop specialized programs and provider networks with the capacity to deliver high-quality care tailored to meet the needs of people experiencing homelessness with the most complex health conditions and highest costs, those health plans will likely attract more members who need this level of service. Without risk-adjustment, the plans that enroll too many of these members will lose money, even if they deliver care that improves health outcomes and reduces avoidable costs. But if the capitation payments to the health plans were appropriately risk-adjusted, so that plans with more high-cost members received higher capitation rates, the health plans with specialized programs could serve these members and achieve savings.
State officials would like the option to offer stronger incentives to health plans (especially those with proven capacity overall) to enroll and deliver high-quality, cost-effective care to the relatively small number of individuals who have the most complex needs and who incur avoidable costs, including people with chronic patterns of homelessness. They recognize that this is the group of people for whom effective care management and more appropriate and integrated services, delivered in the right setting and tailored to the needs of individuals, have the potential for making a big impact on costs and outcomes.
However, state Medicaid program staff have had little opportunity to develop or test the robust risk-adjustment methodologies that would be needed to pursue this concept. As state Medicaid programs and health plans have been strained to implement the rapid transition to managed care for many thousands of Medicaid beneficiaries and to prepare for enrolling people who became newly eligible for Medicaid in 2014, some say that it is nearly impossible for Medicaid agency leaders to devote the attention needed to address this complex design challenge for a small number of people--even though they recognize that the cost implications and potential savings opportunities are significant.
6.5.2. Innovative Approaches from Case Study Sites
Even without robust risk-adjustment tools or clear financial incentives, a few Medicaid managed care plans are moving ahead to support innovative programs and to establish partnerships that can help the plans control costs and improve outcomes for their current members.
Minnesota: Managed Care Support Services Linked to Permanent Supportive Housing
In Minnesota, state contracts with the Special Needs Basic Care plans allow the MCOs to provide "in lieu of" services--meaning some services that are not defined in the state Medicaid plan but "make sense" because of the needs of members and the potential to achieve cost offsets. Representatives of Medica (one of the MCOs participating in managed care in Minnesota) are initially focusing on identifying members who are experiencing homelessness and making frequent use of hospital care or other health services. They say they recognize that, "If people aren't housed they cannot focus on health care." They believe that people identified by the plan as having long or frequent episodes of homelessness and who may be eligible for federal or state housing subsidies are likely to be high users with avoidable costs in the future, even if they are not high-cost, frequent users now.
Performance incentives include Medicaid payment withholds (in rates paid to managed care plans) based on performance targets for reducing emergency department use and hospital re-admissions. Such incentives have real financial implications for health plans and have given Medica added motivation to invest in partnerships with some of the organizations that provide PSH and services for people experiencing homelessness.
Beginning in December 2012, Medica and Hearth Connection established a partnership to serve 85 Medica plan members living in PSH. The health plan provides funding for services that help people retain their housing and become or remain healthy, with HUD's Shelter + Care program paying the rent.
At the time of our final site visit, implementation was just beginning with the identification of Medica's Special Needs Basic Care plan members who appear to be homeless, eligible for housing subsidies and targeted case management services, and in need of both housing and more-intensive supports than the standard approach to care coordination.
During the project's first four months, the Medica Supportive Housing Project enrolled 51 single adult participants. Medica provides Hearth Connection with a list of names of plan members who have been identified based on utilization data or referrals from Medica's social workers and care managers. The program is not limited to serving people with the highest costs, but Medica is hoping to see some return on investment in terms of savings or improved health outcomes.
The project is being implemented in collaboration with a subset of Hearth Connection's partner organizations that already have the capacity to deliver Medicaid-reimbursed TCM services. Hearth Connection and its partner service providers are using the information provided by Medica to find people and engage them in housing and services. Some of the people referred by Medica have previously had limited interaction with the community's homeless outreach programs or community-based social services.
Medica makes payments based on a negotiated amount per-member per-month for two months as service providers try to find and engage each person. Payment is available for an additional month, if needed, to get the person engaged and enrolled in services and connected to a housing unit whose rent can be subsidized using Shelter + Care. Ongoing services are available through the existing TCM reimbursement mechanism, which the plan pays on a monthly basis, or through other existing benefits provided through the Special Needs Basic Care plan.
Hearth Connection would like to negotiate similar agreements with other MCOs and with Hennepin Health (described in Chapter 7 of this report). Another PSH provider currently accepts referrals from Hennepin Health housing navigators and will also get referrals to serve Medica members. So far, the scale of both efforts is small. Competition for supportive housing units has not yet been an issue, but there is some concern about whether there will be enough housing subsidies or opportunities in site-based PSH to meet demand as both Hennepin Health and Medica expand their efforts to link homeless members to housing.
The partnering organizations see this project as an opportunity for collaborative learning and cross-training. Hearth Connection is providing training about housing-first and PSH for Medica care managers, and the Medica care managers will provide training for new Hearth Connection service teams to support them in doing care management for health care. Medica will invest in data analysis and evaluation. Hearth Connection and its partners expect to learn a lot about health care delivery systems and to build their competence in the area of health care. They see the project as an opportunity to build or strengthen connections to health homes, community clinics, and hospitals. Hearth Connection hopes for more opportunities to expand, as plans and health care providers begin to recognize the importance of social determinants of health and of PSH as a cost-effective intervention.
For some Medicaid managed care plans and providers of services to people who are currently homeless and PSH tenants, funding relationships may begin with one-time grant funding through the MCO's program of charitable giving or a foundation connected to the health plan.
For example, some relationships with homeless service providers in Minnesota begin with grants through the Medica Foundation. This allows time to build relationships as plan representatives and providers learn to talk the same language, establish trust, and begin to see results. Over time, more of these services and partnerships are expected to move under the health plan with ongoing contracts.
Through its foundation, Medica is providing grant funding to St. Stephen's Human Services, a provider of PSH and other services for people experiencing homelessness. The grant will pay for a housing navigator who will work with 15 people experiencing homelessness who use emergency room services frequently and are not connected to primary care or other more appropriate health services. The navigator will help link people to other services that are available through the Special Needs Basic Care plan, including primary care and transportation assistance, and work to connect people to housing options that meet their needs.
California: Challenges with Rate-Setting for Managed Care
In California, the opportunities for using capitation as a sustainable strategy for financing more flexible and effective approaches to serving high-need and high-cost beneficiaries are not so clear as they are in Minnesota.
LA Care is the largest public managed care plan in the country, serving more than 1 million Los Angeles residents through free and low-cost health insurance programs. It is one of two Medicaid managed care plans in Los Angeles County.78 Part of LA Care's mission as the managed care health plan for Los Angeles County is to preserve and strengthen the "safety net" providers of health care for very poor people in the county, including the county hospitals and clinics operated by the Los Angeles County Department of Health Services (DHS). As described in more detail in other chapters in this report, DHS and safety net providers that are part of the LA Care provider network are actively involved in serving people who are chronically homeless, creating PSH, and delivering services in PSH. DHS and some of the providers are hoping that LA Care will be able to use a portion of the Medicaid funding it receives to pay for services that help to achieve reductions in other costs for services covered by Medicaid, including avoidable emergency room visits, hospitalizations, and nursing home stays.
LA Care pays a capitation rate to some medical groups or provider networks to cover primary care, specialty care, and hospital services, and it pays some hospitals directly for inpatient and emergency room care. LA Care also pays directly for the first 100 days of nursing home stays. These nursing home stays often follow discharge from an inpatient hospital stay, particularly for patients who entered the hospital from a homeless situation and cannot be discharged safely to shelters or the streets. LA Care also pays for pharmacy and some other expenses. Efforts to control avoidable hospitalizations and provide better support during care transitions are still evolving. Communication and linkages among hospitals, primary care providers, health plan staff, and the mental health service providers and PSH providers who serve the most vulnerable chronically homeless people in the community still need to be improved.
Leaders at LA Care, DHS, and other public and nonprofit agencies recognize that there are significant opportunities to collaborate and develop better procedures for enrollment, assignment of primary care providers, and ongoing care management for people experiencing homelessness and residents of PSH. LA Care is interested in finding better ways to identify those individuals who have the greatest vulnerability and most complex needs and to serve them effectively, recognizing that the health plan has an interest in improving the quality of care and achieving savings.
Medicaid managed care capitation rates are based on the services included in California's Medicaid state plan. It is therefore unlikely that Medicaid managed care capitation rates will cover all the service elements in a PSH program, as the state plan does not include some important services. Based on preliminary discussions with senior leaders at the California Department of Health Care Services, which runs the state's Medicaid program, it is not clear if or how current Medicaid managed care financing mechanisms will pay for some of the service interventions that are likely to produce better outcomes for people experiencing homelessness and to reduce costs for avoidable hospitalizations. Among these are medical respite and nursing and other flexible services in PSH, including services that are delivered in PSH to address problems related to substance use disorders. Based on the terms of California's current Medicaid program, including approved waivers, there is some uncertainty about whether the state could allow health plans to use their capitation rates to pay for services that are not currently defined as covered benefits in the Medicaid state plan, even if there is evidence that these services reduce avoidable costs for other covered services.
6.6. Managed Care in a Behavioral Health Carve-Out--Louisiana's Behavioral Health Partnership
Louisiana has undertaken a multiyear, comprehensive redesign of its public behavioral health system for children and adults. The redesign has required numerous waivers and state plan amendments, some of which are still to come. Completion of the redesign's components is not expected until 2015 or 2016. Known as the Louisiana Behavioral Health Partnership (LBHP), the new system is structured as a type of managed care organization--a statewide management organization--responsible for coordinating care and managing both Medicaid-funded and state-funded behavioral health programs.
Magellan Health Services operates LBHP, which began enrolling clients who qualify for services covered by LBHP programs on March 1, 2012. Services available from LBHP include a broad array of behavioral health services for children and adults.79 As Louisiana has obtained federal approval for changes in Medicaid-covered benefits, new services have been added. Persons experiencing chronic homelessness or living in PSH who qualify for Medicaid are a small part of LBHP's membership, but the plan's provisions include services that have been structured explicitly to help this group manage their health conditions while achieving and maintaining stable housing.
In Louisiana, this study focused on a group of people with complex health and behavioral health needs who were homeless or formerly homeless and participate in a special program--the Permanent Supportive Housing Program (PSHP). PSHP was established in Louisiana with federal funds in the wake of the 2005 hurricanes Katrina and Rita.80 Most PSHP clients have made the transition to coverage through the Louisiana Behavioral Health Partnership, where they and other LBHP members experiencing homelessness or living in PSH may receive a broad range of health care and behavioral health services. The most relevant of these Medicaid-covered services are Assertive Community Treatment, Community Psychiatric Support and Treatment, and other psychosocial rehabilitation and substance use disorder treatment services.81
In addition to the services provided through the Louisiana Behavioral Health Partnership, different components of the state Medicaid program have been covering other aspects of care. For example, medical care is covered separately. For those who need assistance with basic self-care activities, inhome personal care services are covered under the state's Medicaid Long-Term Personal Care Services program. Participants who qualify for and have applied for 1915(c) home and community-based services are either receiving or on waiting lists for those services. A small percentage of participants are also receiving transition assistance from the state's Money Follows the Person demonstration program.
6.6.1. The Role of Louisiana Behavioral Health Partnership for PSHP Clients
Louisiana's 1915(i) State Plan Amendment
As a condition of transferring PSHP's block grant funds to the State of Louisiana, HUD required the state to commit to continuing funding for the PSHP's service component once the block grant funds ran out. Certain provisions of Louisiana's Medicaid state plan, including new covered services and arrangements to provide these services through the Louisiana Behavioral Health Partnership, are designed to fulfill a good part of that commitment to sustaining services for eligible PSHP clients. Under these provisions, Medicaid reimbursements through the Louisiana Behavioral Health Partnership replace some of the block grant dollars that have been paying for services for many Medicaid-eligible clients. The component of greatest interest for people experiencing chronic homelessness or living in PSH is a state plan amendment under Section 1915(i) that received CMS approval in December 2011 and became effective on March 1, 2012.82 To fulfill its PSHP sustainability obligations, the state will also use other resources for persons and activities that Medicaid cannot cover.
To be eligible for Medicaid-reimbursed services under 1915(i), a person must have one or more of the included psychiatric diagnoses, be enrolled in Medicaid, and also meet 1915(i) functional impairment criteria. These eligibility requirements are similar to the requirements for specialty mental health services in all of our case study sites (see Chapter 5). In the CMS approval letter for Louisiana's 1915(i) (p. 11), a qualifying functional impairment is defined in terms of LOCUS scores on the Risk of Harm and Functional Status subscales and composite/global LOCUS score reflecting a "moderate" level of functioning.83 To reach the final score, many factors are considered during assessment and LOCUS administration, including current functioning, treatment history, availability of supports, housing instability, and similar aspects of a client's situation.
Eligibility for 1915(i) Services
Louisiana's 1915(i) state plan amendment provides home and community-based services for adults over age 18 who meet at least one of the following criteria:
Persons with ACUTE Stabilization (AS) Needs. The person with AS needs currently presents with mental health symptoms that are consistent with a diagnosable mental disorder specified within the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) or the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), or subsequent revisions of these documents.
Persons with SMI (federal SAMHSA definition of Serious Mental Illness as of December 1, 2011). The person with major mental disorder (MMD) has at least one diagnosable disorder that is commonly associated with higher levels of impairment. These diagnoses, per the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) or the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), include eight psychotic disorder classifications (six for schizophrenia, one for delusional disorder, one for psychosis not otherwise specified, seven bipolar disorder classifications, two depression classifications, and MMD).
An adult who has previously met the above criteria and needs subsequent medically necessary services for stabilization and maintenance. Exclusion: diagnosis of a substance use disorder without an additional co-occurring Axis I disorder.
6.6.2. Services Available Under 1915(i)
The 1915(i) amendment was developed to cover an array of home and community-based services needed by many people with serious mental illness, especially those who are homeless, formerly homeless, or at risk of homelessness. Inclusion of these services furthers the goal of covering the services needed by many PSHP clients that is explicit in CMS's approval of Louisiana's 1915(i) state plan amendment.84 Covered services include: (1) treatment by a licensed mental health practitioner--an individual licensed in the State of Louisiana to diagnose and treat mental illness or substance use disorders acting within the scope of all applicable state laws and their professional license; (2) Community Psychiatric Support and Treatment; and (3) Psychosocial Rehabilitation, and Crisis Intervention (approval letter, p. 17).
A PSH-specific certification is required for agencies offering tenancy support services to PSHP clients through 1915(i), as some of the support services that PSHP clients have received through that program would not otherwise be part of Community Psychiatric Support and Treatment functions. We refer to this combination of certifications and the services provided by these agencies as PSH-Community Psychiatric Support and Treatment.
Many services of great importance to people experiencing homelessness as they move into and live in PSH are explicitly included in PSH-Community Psychiatric Support and Treatment. The Louisiana Behavioral Health Partnership Technical Manual-Service Definitions describes these services as "restoration, rehabilitation, and support to develop skills to locate, rent, and keep a home, landlord/tenant negotiations, selecting a roommate, and renter's rights and responsibilities." The manual goes on to include in these services "assisting the individual to develop daily living skills specific to managing their own home, including managing their money, medications, and using community resources and other selfcare requirements." Habilitation is included in "developing and implementing social, interpersonal, self-care, daily living, and independent living skills to restore stability, to support functional gains, and to adapt to community living." Medicaid will cover activities furthering these goals as long as they are established as medically needed by LBHP members.
6.6.3. How the Louisiana Behavioral Health Partnership Works--Role of Magellan Care Managers and Tenancy Management Specialists
The staffing structure to support care coordination for people with complex and interacting behavioral health conditions within the Louisiana Behavioral Health Partnership is described here in some detail because it provides the best example we encountered of how an MCO's staff are working with community providers to facilitate getting the right care to its more challenging members, including supports to assure housing acquisition and retention. Within the Louisiana Behavioral Health Partnership, Magellan has set up a staffing structure designed to support client case managers and facilitate getting the right care to plan members. Duties are split between health care and tenancy-related needs. Magellan's care managers are staff members who serve as primary liaisons between a member's care provider or team and the LBHP. A second type of staff, tenancy management specialists, takes on housing-related activities to support members as they seek, obtain, and retain housing.
Magellan care managers are a care provider's primary point of contact with the Louisiana Behavioral Health Partnership. They authorize care for plan members and also assure that clients get the care they need. They discuss treatment plans with providers, checking to see whether the Louisiana Behavioral Health Partnership offers services that would benefit the member but that perhaps the provider did not know about or did not ask for (e.g., a detox bed that is open and that the member might benefit from using it). Care management began these services in March 2012 for everyone then enrolled in the Louisiana Behavioral Health Partnership, including PSHP clients receiving Assertive Community Treatment services. PSHP tenants eligible for Community Psychiatric Support and Treatment services began enrolling in the Louisiana Behavioral Health Partnership in 2013, once Magellan was authorized to provide PSH-Community Psychiatric Support and Treatment services as a covered benefit and PSHP clients received the assessment required to establish eligibility for that benefit.
Services for Assertive Community Treatment authorized under 1915(i) are reimbursed on a monthly case rate, while services for other levels of care are authorized as a number of monthly units of care (in 15minute increments). Magellan uses an initial allocation of care units as a checkpoint, not as a ceiling. The reasoning being that the initial allocation might be enough, and before authorizing more they want to see what has been accomplished. But if more care units are needed, Magellan encourages providers to ask for them. Magellan officials figure that over time they will be able to tell whether authorizing more units of Community Psychiatric Support and Treatment or other types of care pays off in reduced use of expensive emergency services as they expect it will. They want to manage costs by improving outcomes and over time will have the data to make this management approach a reality.
Magellan care managers are working to educate providers to ask for more units if the client's circumstances appear to call for them, and the care managers will usually increase the authorization once they have the facts. Magellan describes the relationship of its care managers to client case managers or teams as one of information seeking/provision and consultation; it has not been adversarial.
Care managers also examine quality-related issues for each provider service team in their portfolio. They review staff credentials to assure that they comply with requirements, check for any complaints against particular provider staff (e.g., lawsuits, complaints to medical boards or employers), and perform other quality control functions.
Magellan's tenancy management specialists handle relationships with landlords and property managers for PSHP housing units, increasingly taking over for the agency that administered Housing Choice Vouchers for the program.85 Tenancy managers negotiate with landlords, deal with landlords when tenant issues arise, and otherwise remove the burden of direct work with landlords from the Community Psychiatric Support and Treatment staff. They do not do direct work with plan members, which remains the job of the Community Psychiatric Support and Treatment teams. The housing-related work of the teams includes helping clients find and move into housing and resolve any behavioral issues that threaten their continued tenancy. If landlord-related housing issues arise, the Community Psychiatric Support and Treatment staff can contact their Magellan care managers and tenancy management specialists for help getting the issues resolved.
6.6.4. Relevance of the Louisiana Behavioral Health Partnership's 1915(i) Services to Qualifying PSH Tenants in Louisiana
Services available under Louisiana's 1915(i) provisions are an excellent example of how a state could shape its Medicaid state plan to maximize the program's ability to cover services of greatest value to people experiencing chronic homelessness or living in PSH. When the PSHP began in 2007, the program's state funding and non-Medicaid federal resources were used to pay for services to help clients get and keep housing, provide supportive services, provide behavioral health services (if the level of care was Assertive Community Treatment), and connect to other agencies to meet client needs. At that time, the agencies delivering these supportive services were not Medicaid providers in Louisiana, and thus needed to become certified to offer one or more of the services available through the Louisiana Behavioral Health Partnership once clients transitioned to that plan. Relevant services for PSHP clients and tenants eligible for services under the state's 1915(i) state plan amendment include Community Psychiatric Support and Treatment, Crisis Intervention, Psychosocial Rehabilitation, and Assertive Community Treatment. As described earlier, a PSH-specific certification is also required for agencies offering tenancy support services to PSHP clients through 1915(i), and additional specialized training is required to obtain this PSH certification.
All agencies serving PSHP clients in Orleans and Jefferson parishes, the local focus of this study, qualified to continue offering their services as Medicaid providers in Louisiana. Those delivering Assertive Community Treatment did so as of March 1, 2012, the date that enrollment in the Louisiana Behavioral Health Partnership began. Program participants who qualify for Assertive Community Treatment services also meet the diagnostic and impairment criteria for SSI and most are now enrolled in Medicaid. These participants also meet the eligibility criteria for services covered under 1915(i), so once the Assertive Community Treatment agencies were certified they began enrolling their clients in LBHP. They likewise began seeking Medicaid reimbursement for services delivered after that date.
During the years before the Louisiana Behavioral Health Partnership was established, some participants in Louisiana's PSHP received services from Housing Support Teams, the predecessors to the Partnership's Community Psychiatric Support and Treatment Teams. These teams provided a somewhat less-intensive level of support for people who did not qualify for Assertive Community Treatment. All the agencies that were operating Housing Support Teams and chose to pursue certification also qualified as Medicaid providers and completed the required specialized training to deliver PSH-specific Community Psychiatric Support and Treatment for PSHP clients. With the transition to the Louisiana Behavioral Health Partnership, some additional agencies also qualified and came on board. Service agencies in the program also had the option to seek certification to deliver Psychosocial Rehabilitation and Crisis Intervention services, and all but one are now certified to provide these service to qualifying clients.
Additional behavioral health agencies may seek certification to provide PSH-specific Community Psychiatric Support and Treatment services to clients qualifying under 1915(i) and living in or qualifying for PSH offered through the PSHP; this process is already under way. Officials consider such expansion desirable, as it would increase competition among providers while affording consumers a choice if they live near more than one qualifying agency. To qualify, agency staff would have to have the right credentials, complete the special training for PSH tenancy work, and the agencies themselves would have to be certified for PSH-specific Community Psychiatric Support and Treatment.
Louisiana anticipates that the PSHP will cover more clients as more housing units become attached to the program. The state added 351 units to the program in 2013 through a new Section 811 project (HUD affordable housing for people with disabilities) and expects to add more as opportunities arise. Medicaid could cover the costs of some of the supportive services to tenants in these units if the tenants themselves qualify for 1915(i) services and the agencies providing the services are certified as providers of PSHspecific Community Psychiatric Support and Treatment services.
6.6.5. Home and Community-Based Services Under a 1915(c) Waiver
A 1915(i) state plan amendment is not the only way that Louisiana has structured its Medicaid program to support the housing-related services needed by people with complex health and behavioral health conditions. The state also has several 1915(c) Home and Community-Based Services waivers that give it additional flexibility.
The PSHP is a cross-disability PSH initiative; some participants do not have a serious mental illness and thus do not fall under the purview of the Louisiana Behavioral Health Partnership, although they do have other qualifying disabilities. Many of these individuals can be served under one of the state's four existing 1915(c) Medicaid HCBS waivers for persons with developmental disabilities or for persons, including the elderly, who acquire a physical or cognitive disability after age 22 (generally referred to as the Aging/Disabled population). Louisiana submitted Medicaid waiver amendments to CMS to add tenancy supports for persons served under these waivers, all of which have been approved (see amendment wording below). PSHP participants who currently receive or who qualify and are certified for participation in one of these waivers will have their tenancy supports reimbursed by Medicaid through that mechanism. At the time this research concluded, it had not yet been decided whether claims under 1915(c) waivers would be processed through Louisiana Behavioral Health Partnership/Magellan (for plan members) or be billed directly through the regular Medicaid claims process (for everyone receiving relevant services).
EXHIBIT 6.1. Possible Service Definitions for Two New Housing Services Provided under 1915(c) Waivera
1. Housing Stabilization Services
Service Definition (Scope) Housing Stabilization Services enable waiver participants to maintain their own housing as set forth in the participant's approved plan of care (POC). Services must be provided in the home or a community setting. The service includes the following components:
- Participate in plan of care renewal and updates as needed, incorporating elements of the housing support plan.
- Provide supports and interventions per the individualized housing support plan. If additional supports or services are identified as needed outside the scope of Housing Stabilization Services, communicate the needs to the Support Coordinator.
- Provide ongoing communication with the landlord or property manager regarding the participant's disability, accommodations needed, and components of emergency procedures involving the landlord or property manager.
- Update the Housing Support Plan annually or as needed due to changes in the participant's situation or status.
Specify Applicable (if any) Limits on the Amount, Frequency, or Duration of this Service This service is only available upon referral from the Support Coordinator. This service is not duplicative of other waiver services including Support Coordination. This service is only available to persons who are residing in a State of Louisiana Permanent Supportive Housing unit. No more than 72 units of Housing Stabilization Services can be used per year without written approval from the Support Coordinator. No more than 165 units of Housing Transition or Crisis Intervention and Housing Stabilization Services can be used per year without written approval from the Support Coordinator.b
2. Housing Transition or Crisis Intervention Services
Service Definition (Scope) Housing Transition or Crisis Intervention Services enable participants who are transitioning into a PSH unit, including those transitioning from institutions, to secure their own housing or provides assistance at any time the participant's housing is placed at risk (e.g., eviction, loss of roommate or income). The service includes the following components:
- Conduct a housing assessment identifying the participant's preferences related to housing (type, location, living alone or with someone else, accommodations needed, other important preferences) and needs for support to maintain housing (including access to, meeting terms of lease, and eviction prevention), budgeting for housing/living expenses, obtaining/accessing sources of income necessary for rent, home management, establishing credit and understanding and meeting obligations of tenancy as defined in lease terms.
- Assist participant to view and secure housing as needed. This may include arranging or providing transportation. Assist participant to secure supporting documents/records, completing/submitting applications, securing deposits, locating furnishings.
- Develop an individualized housing support plan based upon the housing assessment that includes short and long-term measurable goals for each issue, establishes the participant's approach to meeting the goal, and identifies where other provider(s) or services may be required to meet the goal.
- Participate in the development of the plan of care, incorporating elements of the housing support plan.
- Look for alternatives to housing if permanent supportive housing is unavailable to support completion of transition.
- Communicate with the landlord or property manager regarding the participant's disability, accommodations needed, and components of emergency procedures involving the landlord or property manager.
- If at any time the participant's housing is placed at risk (e.g., eviction, loss of roommate or income), Housing Transition or Crisis Intervention Services will provide supports to retain housing or locate and secure housing to continue community-based supports including locating new housing, sources of income, etc.
Specify Applicable (if any) Limits on the Amount, Frequency, or Duration of this Service This service is only available upon referral from the Support Coordinator. This service is not duplicative of other waiver services including Support Coordination. This service is only available to persons who are residing in a State of Louisiana Permanent Supportive Housing unit or who are linked for the State of Louisiana Permanent Supportive Housing selection process. No more than 93 units of Housing Transition or Crisis Intervention can be used per year without written approval from the Support Coordinator. No more than 165 units of Housing Transition or Crisis Intervention and Housing Stabilization Services can be used per year without written approval from the Support Coordinator.
- This wording is attached, with CMS approval, to Louisiana's 1915(c) Community Choices Waiver (in 2013), as well as to its 1915(i) state plan amendment (approved by CMS in 2011). For more information see http://new.dhh.louisiana.gov/assets/docs/OAAS/publications/CCW_Fact_Sheet.pdf and http://new.dhh.louisiana.gov/assets/docs/BehavioralHealth/LBHP/SPA_TN_11-13.pdf.
- This wording refers to limits on units of service used by a particular client, not to limits on the number of clients that may be served.
6.6.6. Services for People with Substance Use Disorders
Many people experiencing homelessness and PSHP tenants who have substance use disorders also have a co-occurring serious mental illness, and they may be enrolled in Medicaid and eligible for 1915(i) services on the basis of their mental illness. But the eligibility criteria specified in Louisiana's 1915(i) state plan amendment do not include people with a diagnosis of substance use disorder who do not also have a co-occurring Axis I mental illness diagnosis.
Medicaid recipients enrolled in the Louisiana Behavioral Health Partnership have access to all the substance use treatment services available within Louisiana's Medicaid program, as well as other state-funded substance use services. Some stakeholders described these benefits and services as limited--a situation similar to that in many other states. Some PSHP participants who do not have a mental illness have one or more chronic and disabling health conditions. If they are eligible for Medicaid as an SSI beneficiary, they may receive other Medicaid services and supports, which are administered separately from the benefits managed through the Louisiana Behavioral Health Partnership. Some of these participants receive benefits available under one or more of the state's home and community-based services waivers. Because Louisiana policymakers have decided not to expand Medicaid eligibility under the Affordable Care Act, it currently appears unlikely that most nonelderly homeless adults whose disabilities are attributable to substance use will be enrolled in Medicaid or eligible for Medicaidcovered services, unless they have another disability that makes them eligible for SSI.
6.6.7. Use of Savings for Services Beyond Those Specified in the Medicaid State Plan
A final important provision of the Louisiana Behavioral Health Partnership is its ability to use program savings to pay for types of service not explicitly included in Louisiana's Medicaid state plan. This ability is authorized under a provision of one of the state's plan amendments--1915(b)(3). In Louisiana these savings will be used to fund children's services, but other states could also request this arrangement, which would allow managed care organizations some flexibility to provide services, such as care coordination and housing supports for high utilizers of expensive services, beyond those specified in the Medicaid state plan.
6.7. Summary
There has been a substantial movement nationwide toward managed care for Medicaid beneficiaries, initially for families but in recent years also for seniors and people with disabilities. Many states are requiring that people newly eligible for Medicaid in 2014 enroll in managed care plans, most of which are expected to cover both medical and behavioral health care. Risk-adjustment in setting capitation rates is a critical piece of the managed care puzzle for addressing the needs of people with complex conditions, including those with histories of chronic homelessness. Government officials, PSH providers, and other stakeholders interested in using Medicaid for services in PSH can learn from some promising program initiatives now under way. This chapter reviewed developments in managed care arrangements in case study sites to include provisions designed to meet the needs of people with complex health needs and cooccurring conditions, including those experiencing chronic homelessness or living in PSH. These include Minnesota's Special Needs Basic Care program and the Louisiana Behavioral Health Partnership.
Experiences with enrolling seniors and persons with disabilities in managed care plans in some other case study sites indicate that the shift to managed care may encounter some setbacks, at least initially if managed care plans and health care provider networks lack experience with people who have a mental illness or other disabilities (with or without co-occurring substance use issues), making it difficult for the plans to offer a sufficient supply of some services or to facilitate continuity of care with trusted service providers. New initiatives are under way to alleviate these difficulties.
7. Innovative Models for CARE Coordination, Including Accountable CARE Organizations
Chapter 7 Highlights
The Accountable Care Organization (ACO) concept is fairly new, first appearing in 2007. The Kaiser Commission on Medicaid and the Uninsured describes an Accountable Care Organization as, " a providerrun organization in which the participating providers are collectively responsible for the care of an enrolled population and also may share in any savings associated with improvements in the quality and efficiency of the care they provide."
The first ACOs were created to serve Medicare patients. Recently several states have launched initiatives to develop and implement ACO-like models in Medicaid, most of which are in the early stages of development.
Two examples in this chapter--Together4Health in Chicago and Hennepin Health in Minnesota--are developing ACO-like models within Medicaid. The third is a unique approach to integrating housing into health and behavioral health care in Los Angeles launched by the county Department of Health Services.
These three initiatives differ in some ways while working toward similar goals:
Auspices: Hennepin Health is a state demonstration project run by the county's Human Services and Health Department; Together4Health is a limited liability for-profit company operating under a contract with the Illinois Medicaid office; Housing for Health is an innovative restructuring of some county Department of Health Services activities, designed from within the department.
Funding: Hennepin Health uses state, county, and Medicaid dollars; Together4Health uses Medicaid dollars and support from foundations for start-up costs; Housing for Health uses county general fund dollars and has obtained funding from a foundation for housing subsidies.
Target Populations: All serve low-income populations; Hennepin Health serves adults who are newly eligible for Medicaid, homeless and housed; Together4Health serves Medicaid beneficiaries only, homeless and housed, including those eligible for both Medicaid and Medicare; Housing for Health is only for the most vulnerable homeless people served by the Department of Health Services, with the most complex, cooccurring conditions (although the department serves the larger homeless and housed low-income populations in its many other activities).
All three are creating strategies that seek to integrate care for their clients across four critical domains: medical care (both primary and specialty), mental health care, substance use treatment, and housing.
7.1. Introduction
This chapter looks at three innovative models for care coordination for individuals experiencing chronic homelessness. Two of the examples are initiatives to create Accountable Care Organizations (ACOs) or ACO-like models--Hennepin County, Minnesota's Hennepin Health and Chicago's Together4Health (T4H). These initiatives are led by providers from the nonprofit and public sectors working to organize the local health and behavioral health care delivery systems to meet the needs of the community's most vulnerable, extremely low-income members. Both have an explicit focus on those with chronic patterns of homelessness, and both include housing as part of the picture. A third example is Housing for Health, Los Angeles County Department of Health Services' ambitious program to link housing, health, and behavioral health services for the same population through linkages with housing providers and its own network of county hospitals, clinics, and contracted service providers.
The Accountable Care Organization (ACO) concept is fairly new, first appearing in 2007. The Kaiser Commission on Medicaid and the Uninsured describes an Accountable Care Organization as, " a provider-run organization in which the participating providers are collectively responsible for the care of an enrolled population and also may share in any savings associated with improvements in the quality and efficiency of the care they provide" (Kaiser 2012).
The first ACOs were created to serve Medicare patients. The Affordable Care Act contains provisions that recognize Medicare ACOs; it also authorized a demonstration project for pediatric ACOs and provided authority for the Centers for Medicare and Medicaid Innovation to test new models of care delivery and payment reform. Several states have launched initiatives to develop and implement similar models in Medicaid that aim to reduce costs and increase quality, most of which are in the early stages of development. Both T4H and Hennepin Health are examples of efforts to create ACO-like entities in Medicaid.
The three initiatives featured here--Hennepin Health, T4H, and Housing for Health --differ in some ways while working toward similar goals.
Hennepin Health. Hennepin Health is one of the pilot projects selected by the State of Minnesota to develop ACOs to serve people enrolled in Medicaid. It has been designed to enroll and deliver care to adults who are newly eligible for Medicaid under the Affordable Care Act.86 It is county-run, with the county's health care and human service systems playing key early roles. Its goal is to integrate medical, behavioral health, and human services in a patient-centered model of care. A central premise of Hennepin Health is to promote the integration of care across fragmented service systems and to address social determinants of health as a strategy for improving health outcomes and lowering costs for the most complex and highest-cost Medicaid enrollees. Hennepin Health is expected eventually to serve more than 10,000 people and had 8,774 people enrolled as of July 2014.
Hennepin Health was a "work in progress" during the study time frame; experiences during its first year illustrate some of the challenges ahead for such efforts, as well as some of the opportunities for connecting an emerging ACO to supportive housing and other services and supports to address social determinants of health.
Together4Health (T4H). T4H is a new for-profit company comprising a network of providers covering the city of Chicago. The Illinois Medicaid office selected T4H as one of six Care Coordination Entities (CCEs) following a competition offered by the Illinois Department of Healthcare and Family Services (of which the Medicaid office is a part) in conjunction with the governor and three other state agencies. T4H members include five hospital systems (including Cook County), eight Federally Qualified Health Centers, and numerous mental health, substance use, behavioral health, and permanent supportive housing providers, as well as advocacy organizations. T4H and the state settled a contract for the program in late fall 2013, and T4H began enrolling clients in December 2013. While not currently a full-risk managed care organization, it anticipates working toward that status over the next few years.
Los Angeles County's Housing for Health is similar to Hennepin Health in that it is a county-run program seeking to integrate health and behavioral health care and stable housing. It negotiates directly with housing providers, seeking to obtain housing units dedicated to the clients of the Department of Health Services' many hospitals, clinics, and community partners in exchange for covering the cost of supportive services to help people retain housing.
7.2. Accountable Care Models in Medicaid
Accountable Care Organizations and similar integrated care models emphasize person-centered, continuous and comprehensive care. The CMS Center for Medicaid and CHIP Services released two letters to state Medicaid directors in 2012, providing guidance regarding Medicaid Integrated Care Models (ICMs), including ACOs and ACO-like models for payment and service delivery reform.87
As described by the Kaiser Commission on Medicaid and the Uninsured, ACO models vary, but they typically include three key elements: a provider organization at the base, accountability for shared outcomes, and the potential for shared savings. ACOs all focus on patient-centered care and involve the increased use of data and quality metrics, increased coordination of care, and incentives designed to reward improved outcomes. ACOs are intended to achieve savings in comparison with costs of health care services delivered and financed through fee-for-service arrangements. While ACOs are intended to improve health care quality while also controlling costs for all patient populations, they are particularly focused on providing benefits for patients with complex medical problems or social needs, who have the most to gain from improvements in care delivery, care coordination, and closer collaboration among providers of health care and social services.
ACOs: Key Activities and Functions
As ACOs and ACO-like models for people enrolled in Medicaid emerge in several states across the country, the Center for Health Care Strategies has observed some key activities and crucial functions:
Patient-centered care management and coordination, directed by providers (e.g., primary care team) as opposed to the managed care organization.
Targeted and intensive complex care management, tailored to the needs of a smaller subset of high-need, high-cost patients, with cross-functional care teams that span physical health, behavioral health, and social services, including long-term supports and services.
Data infrastructure and analytics, including claims-based data, electronic health records, and a health information exchange.
Motivated and mission-driven leadership and providers:
- Empower providers to transform care delivery, including building high-performing, cross-functional teams that include primary care providers who are engaged in on-the-ground collaboration with mental health, substance abuse, long-term supports and services, social service providers, patients, and their families.
- Structure ACO for meaningful patient and community partnerships, including the capacity to address social needs such as unstable housing and homelessness that directly lead to health challenges.*
* Center for Health Care Strategies, Accountable Care Organizations in Medicaid: Emerging Practices to Guide Program Design, Policy Brief, February 2012. http://www.chcs.org/usr_doc/Creating_ACOs_in_Medicaid.pdf.
While emerging ACO models hold much promise for improving outcomes while controlling health care costs for patients with complex health and social needs, these models require substantial initial investments in capacity-building and infrastructure development. To be feasible, these ACO models also require that states or other purchasers and providers negotiate payment models that align financial incentives to serve patients with the greatest needs and highest risks. Well-designed systems for setting rates, sharing savings, and rewarding performance, including appropriate risk-adjustments, are important components of ACO financing strategies. They are often, however, very challenging to create, in part because existing risk-adjustment methodologies do not capture factors associated with social determinants of health or other complexities related to co-occurring health and behavioral health conditions (Lewis et al. 2012).
The next three sections of this chapter describe the new models we have been following through case studies. As we describe each of these major efforts, we describe how care coordination and housing stabilization services are organized and delivered; how the finances work, including the role of Medicaid and other funding sources; challenges to financial viability; and issues related to information technology and data sharing.
7.3. Hennepin Health
In Minnesota, a 2010 state law authorized the Department of Human Services to develop a Medicaid demonstration project to test alternative and innovative health care delivery systems, including Accountable Care Organizations. That year a state law also authorized Hennepin County to establish a pilot program to provide a health delivery network for adults without children whose incomes were at or below 75 percent of the federal poverty level. In 2011, a new state law, the Medical Assistance Reform Waiver Act, included the expansion of Medicaid eligibility for persons with incomes up to 75 percent of poverty and authorized the Department of Human Services to pursue waivers or changes in the state's Medicaid plan to reform the state's Medical Assistance program to achieve a variety of goals related to improving health outcomes and controlling costs.
In late 2011, the Department of Human Services began negotiations with Hennepin County to create a pilot ACO program for adults without children.
On January 1, 2012, the Department of Human Services contracted with Hennepin County to establish Hennepin Health, an integrated delivery network for adults without children with incomes up to 75 percent of poverty. Hennepin Health includes the county's public hospital, Hennepin County Medical Center, which provides inpatient, specialty, and outpatient clinic services, and the Northpoint Health and Wellness Center (outpatient clinic), as well as the county's Human Services and Public Health Department and Metropolitan Health Plan.
The vision of Hennepin Health includes a strong focus on integrating health, behavioral health, and social services to address social determinants of health, expecting to achieve savings by reducing avoidable hospitalizations and emergency department services and preventing duplication of care. This is how the county described the premise for Hennepin Health in its proposal submitted to the state in October 2011:
Treating a safety net patient's medical problems without addressing underlying social, behavioral, and human services barriers and needs produces costly, unsatisfactory results--both for the patient and the programs providing and paying for care. Conversely, addressing all of these issues and incorporating them into a coordinated patient and family-centered, comprehensive care plan should end the cycle of costly crisis care.88
Consistent with this premise, the Hennepin Health approach has been guided by an understanding that unmet social needs, including homelessness and hunger, have a significant impact on health status and the use and cost of health services for its members.
"We needed to build a system that first and foremost looks at the social determinants of health. What is wrong with my patient that I can't fix in this room but somebody else could?"
Mark Linzer, M.D., Director of General Internal Medicine at HCMC (Lowden 2012)
As Hennepin Health leaders describe their experience during the first year of implementation, they were "inventing as we go" and there was "no roadmap" for care coordination and for understanding and managing the total cost of care for these members across settings and providers. During the first year, they found that it was a bit of a challenge to "demand something different" for Hennepin Health members from the county hospital, clinics, and other programs, because the Hennepin Health members are only a subset of the low-income people served in these settings. Even at the county's Coordinated Care Clinic, which serves people with complex needs including many people experiencing homelessness, only about 30 percent of patients are Hennepin Health members.
The goals of Hennepin Health include increasing the level of engagement by the health care delivery system with patients and enrolled members, and facilitating stronger connections among health care and social services programs.
County-funded programs that serve low-income people are expected to be partners in delivering some of the services needed by Hennepin Health members. Hennepin County's planning efforts and work groups formed to support implementation of Hennepin Health have included representatives of county-funded programs serving people experiencing homelessness.
When Hennepin Health was first launched, some staff members and clinicians saw it as a standalone pilot or special population program rather than a strategy for transforming the way care is delivered for everyone who relies on the county's health care and social services systems. In the process of launching Hennepin Health and managing change within the health care system, it has been important to strike a balance between using the resources of Hennepin Health to make improvements for Hennepin Health members and pursuing opportunities to better coordinate and improve care for all of the low-income people who seek care from Hennepin County. One strategy for mitigating this challenge has been an ongoing effort by Hennepin Health leaders to identify improvements that can be made without additional funding, and to extend the learning and systems improvements of Hennepin Health to serve other people when possible.
7.3.1. Care Coordination and Housing Stabilization
Plans for Hennepin Health included an ambitious "tiering system" for matching people to the most appropriate types of clinical care at different levels, based on the complexity of their health and social needs. The program is designed to provide more-intensive services for members with high levels of need, including those with multiple emergency room visits for medical or mental health conditions or chemical dependency issues. Some staff members in public agencies, the county hospital, and clinics were assigned to new roles.
Community health workers were hired or reassigned to deliver enhanced services to Hennepin Health members, including conducting outreach, helping patients follow through on treatment recommendations, helping them make changes to harmful or risky behaviors, providing the personal attention and coaching to encourage members to stop smoking or achieve and maintain sobriety, and identifying patients with unmet needs for housing or other social supports and services. Hennepin County has provided extensive training to help workers acquire new skills, gain familiarity with resources available across health care and social services systems, and move into new roles that include increasing engagement with members outside of clinic settings.
During the first year of implementation, Hennepin Health launched several program initiatives to improve and better coordinate care for the most vulnerable and costly members, while achieving savings. Some examples are described below:
The program identified a large number of emergency room visits associated with dental pain and made arrangements for same-day dental care for patients who could be diverted from the hospital emergency department, where they could only get pain medications, to get them the right care to meet their needs.
The program determined that homeless patients often lacked transportation to visit a pharmacy to get prescribed medications, so it implemented a system for delivering medications to shelters, reducing the need to provide transportation vouchers and increasing timely prescription refills and medication compliance.
The program recognized the consequences of fragmentation across health care and behavioral health services, and worked on strategies to co-locate care, embedding behavioral health clinicians in primary care clinics and developing primary care services that can be delivered in behavioral health clinics. The program has worked to create a process for "warm handoffs" and more seamless transitions among programs.
Housing navigators play an important role in serving Hennepin Health members whose homelessness or residential instability has a significant impact on health-related vulnerabilities and service use. The housing navigators are employed by the county's Human Services and Public Health Department. They play a broker role--they do not work directly with clients but instead work with the social workers and community health workers who are part of the teams based in clinics or the county hospital. Clinical teams and the housing navigators use the Hennepin Health "tiering system" to target assistance to the most vulnerable patients who are homeless or unable to return to a safe and stable living situation and at (or close to) tier 3, meaning the person has had multiple emergency department visits or detox stays, or two or more hospital admissions for medical conditions, mental health, or substance use disorders in the past year, or acute medical needs. The goal is to focus on those whose lack of housing is contributing to escalating medical costs, prioritizing housing for those for whom it is likely to have the greatest impact not only on quality of life but also on cost reductions, providing a return on investment that can help make the case for funding the necessary supports.
About 75 percent of the people referred to the housing navigators are currently unsheltered or staying in homeless shelters, and many have been experiencing long-term homelessness. Through the referral process, the housing navigators, community health workers, social workers, and clinical team members are developing a shared understanding about how to identify and describe housing status and needs, including the definition of homelessness and eligibility criteria for housing programs, as well as what housing options are available to offer patients. Housing options include both emergency or short-term options as well as permanent supportive housing. Housing navigators know about all of the housing options in the county, and they know which programs use a housing-first approach and which have rules about sobriety.
The community health workers and social workers who make referrals gather information about patients and then work with the housing navigators to identify options that offer the best fit for each individual in terms of eligibility, needs, and preferences. The housing navigators track information about housing program characteristics, including application procedures and vacancies, and then offer up to three options for the community health workers or social workers to discuss with their clients. The community health workers or social workers are responsible for helping clients follow through to complete applications and get into housing. If the client is rejected by a suggested housing provider, the housing navigators keep trying to find other options. The housing navigators also provide information that community health workers can use to follow up on their own to assist other patients who have lower levels of need.
Hennepin Health community health workers, social workers, and housing navigators have helped to achieve significant improvements in the well-being of members who were experiencing chronic homelessness, and they can point to success stories like the person with diabetes who was able to manage meals and diet after getting into housing, reducing the need for hospital care. Another Hennepin Health member who was experiencing homelessness frequently visited the emergency room for pain management, but had been unable to get needed surgery without a home in which to recover. With help to get housing, the person was able to have surgery and recover at home, reducing costs for avoidable emergency room visits and providing a significant improvement in quality of life.
For people experiencing homelessness who are hard to engage, the county's Health Care for the Homeless program and a nonprofit partner, St. Stephens Human Services, do street outreach and collaborate with Hennepin Health housing navigators. Hennepin Health also has a social services navigator who is out in the field and can help to locate vulnerable Hennepin Health members. This person coordinates with Health Care for the Homeless and local shelters to find people when they come in for service, to let them know they need to follow up on a housing option the housing navigators have found for them.
During the time frame for this study, Hennepin Health had not been able to allocate new resources directly for PSH. But by providing supports and working to coordinate care for its members, Hennepin Health helps to supplement the services in PSH and to help some very vulnerable people who were experiencing homelessness to succeed in housing. In addition, the county already provides funding and administers state and federal funding for a wide range of housing and residential programs. Housing providers that receive funding through the county are encouraged to give priority to people who are referred by Hennepin Health housing navigators, and the county is trying to find ways to create incentives for housing providers to prioritize members when there are openings. For example, when the county issued a request for proposals for new housing development, the project selection criteria awarded extra points for providers that agreed to prioritize housing applicants referred by Hennepin Health.
Some housing providers are calling the housing navigators when they have vacancies. Although Hennepin Health does not fund PSH services, the housing providers recognize that Hennepin Health members come with a connection to health care and other services, and these connections and supports can help a homeless person be a more successful tenant. The county also has some leverage to advocate for changes in the tenant selection criteria used by housing providers who receive funding through the county. The process of using the housing navigators to facilitate housing placements for Hennepin Health members has provided an opportunity to focus on some housing providers who have been highly selective, sometimes offering housing only to people already participating in their programs and screening out many people experiencing homelessness. When these barriers are identified, the program manager for the county's Housing and Homelessness Initiatives can advocate for changes to improve access to housing for those with the greatest needs and barriers.
During the first year of Hennepin Health implementation, the housing navigators expected to facilitate about 100 housing placements. Already they have been seeing some good outcomes in terms of reducing use of the most costly inpatient and crisis health services and improving health outcomes. The housing navigators reported that they sometimes hear from social workers who say that the clinical teams are recognizing the health impacts of housing solutions.
7.3.2. How the Finances Work
Hennepin Health receives Medicaid funding on a capitated basis, meaning a fixed payment per-member per-month for the total cost of care including all Medicaid-covered health services with the exception of long-term care. Social services are funded through other existing sources and are not included in the capitation rate.
Hennepin County had hoped to receive a risk-adjusted capitated rate for a package of covered health, mental health, and chemical dependency services. "We already have the highest risk patients," say county staff, who had hoped the rate would reflect this high level of risk and need. The rates negotiated with the state were not risk-adjusted, but instead were the same as the rates the state negotiated with insurance companies to cover newly eligible people. They included only four rate cells with different rates based on gender and age (21-40 and 41-64). Rates may be renegotiated in future years.
Hennepin County's health plan, the Metropolitan Health Plan, provides administrative services for Hennepin Health, including payments to providers at contracted rates for covered services. The County is tracking revenues and claims data, as well as other data in electronic health records, to evaluate the total cost and quality of care. A shared savings pool is funded from savings that result from a more efficient care model that reduces expensive and avoidable hospital admissions, re-admissions, and health complications.
At the end of its first year, Hennepin Health leaders reported that they had achieved savings "all over the place," including a 29 percent reduction in inpatient hospitalizations and a 24 percent reduction in emergency department visits, and they had adopted a re-investment strategy for 2013. The goal of this strategy was to further reduce costs by continuing to reduce inpatient and emergency department utilization while increasing primary care engagement and improving health outcomes. Priorities for reinvestment in 2013 included funding start-up costs and motivational interviewing training for a new 30-bed sobering center to divert chronic inebriates from the emergency room; developing interim housing units through a partnership with the Minneapolis Housing Authority to provide placement alternatives with wraparound services for persons "stuck" at Hennepin County Medical Center or other institutional facilities at county cost; expanding the capacity of the Coordinated Care Clinic; and creating a new program of community support and linkage for the most frequent users of hospital emergency room care.
7.3.3. Information Technology and Data Sharing
Hennepin Health was launched with ambitious plans to create for all enrollees "a single, comprehensive electronic record that is inclusive of many facets of their treatment, tells their story, tracks their goals, includes the care plan and outcomes data, and evaluates their responses to interventions across a continuum of care."89 The county uses the Epic electronic health record for most of the care system and is working to enhance that system to provide the capacity to link primary care, specialty care, behavioral health care, and social services into one seamless system that can provide real-time data for clinical teams to support the delivery and coordination of care.
The Hennepin Health partners have worked to allow Metropolitan Health Plan to have direct access to the patient's electronic health record for inputting critical health plan information into the chart for provider action, including data about member calls, hospital alerts, and referrals. This shared information helps to support care planning. It also reduces duplication of assessments, referrals, and some interventions, and provides real-time alerts to primary care providers about hospitalizations. Hennepin Health also provided access to the county health care system's patient record system (with client consent) to allow community behavioral health care providers to have more timely information to support hospital discharges and prevent re-admissions.
An analysis of pharmacy data allowed Hennepin Health to identify the highest users of the plan's pharmacy benefit, including some members who were seeing and getting prescriptions from more than ten providers and filling prescriptions with seven or more pharmacies.90 Through outreach to these members and other interventions, Hennepin Health helped to facilitate connections to health care homes, reducing medications costs significantly as well as reducing health risks associated with medication side effects and complications.
For busy health care professionals, more data from multiple providers and systems can be a mixed blessing, and providers have limited time to review other records to find the information they need to make good decisions about care. Hennepin Health created provider dashboards to make it easier for providers to find critical data.
Progress toward data sharing across systems of care has been challenging. Hennepin Health has encountered some barriers in provisions of state law that govern the privacy of health care and social services, but do not include provisions for information sharing across systems to facilitate collaborative care. Hennepin County has advocated for the state to enact legislation to allow providers working within an accountable care system to share data among partners, specifically to share data across health care and welfare entities. Hennepin Health would like to obtain consent for systematic data sharing as part of the process of enrolling members in these public programs.
While the implementation of Hennepin Health has been challenging, there were very significant accomplishments in improving and coordinating care for its members during its first year. Housing navigators have worked to facilitate access to housing for the most vulnerable homeless members, and the services provided by Hennepin Health have promoted housing stability and recovery for some PSH tenants. This has not yet translated into a way to finance the services that are part of PSH, which are still funded by a variety of federal, state, and county programs. Hennepin Health is not paying for PSH at this time, but can provide or facilitate linkages to some additional services such as nursing or home health workers to enhance the capacity of supportive housing providers to house Hennepin Health members who have more significant health needs. Hennepin Health leaders expressed an interest in using Medicaid financing to cover services within PSH for medically fragile persons experiencing homelessness. They anticipate that the return on this investment would be reductions in other health care costs, but they are uncertain about what types of PSH services could be covered using capitated Medicaid funding.
As noted in an earlier chapter, one of the biggest challenges facing Hennepin Health during its first two years was the significant monthly turnover in enrollees, as an average of 15 percent of its members became disenrolled each month primarily because they failed to complete recertification paperwork. For many of Hennepin Health's members, who had been uninsured and living with incomes significantly below poverty before the expansion of Medicaid eligibility, staying enrolled in a health plan had not been either possible or a priority. Maintaining enrollment in Hennepin Health was particularly challenging for members with incomes far below the federal poverty level who were experiencing homelessness and ongoing crises. Recertification notices failed to reach as many as half of Hennepin Health's members because they lacked a stable address at which to receive mail. As a result, members did not know they were no longer enrolled until they sought care and discovered that there was a lag time for processing applications to renew or restore coverage.
Hennepin Health does not receive monthly capitation payments for the months during which a member is not enrolled. The problems Hennepin Health experienced with churning enrollment not only jeopardize the financial viability of an ACO model because the gaps in coverage reduce payments to the plan, but they also make it difficult for the plan to deliver continuity of care and to achieve and track outcomes for its members. Hennepin Health leaders were hopeful that some of these problems could be reduced when Affordable Care Act provisions for streamlined and automated Medicaid eligibility determinations and redeterminations are fully implemented starting in 2014.
7.4. Together4Health
T4H is an example of an Accountable Care Organization-like entity under development. It is an innovative care coordination model made possible by the Illinois Medicaid program's response to a requirement imposed by the Illinois state legislature to "move at least half of recipients eligible for comprehensive medical benefits to a risk-based care coordination program by January 1, 2015."91 Having started in 2010 with a pilot program involving traditional Health Maintenance Organizations in the ring counties around Chicago, by the end of 2011 the state wanted to see what other structures might work to achieve the same ends.
In early 2012, the state issued a "Solicitation for Care Coordination Entities and Managed Care Community Networks for Seniors and Adults with Disabilities (Innovations Project/2013-24-002)." Participating state agencies included the Department of Healthcare and Family Services (which administers the state's Medicaid program); the Office of the Governor; the Department of Human Services, Divisions of Mental Health, Rehabilitation Services, and Developmental Disabilities; the Department on Aging; and the Department of Public Health. The solicitation's introduction states its purpose:
to allow Providers to design and offer care coordination models other than traditional Health Maintenance Organizations (HMOs). The Department invites innovative Proposals to demonstrate that Providers can provide equal or better care coordination services, produce equal or better health outcomes and render equal or better savings than traditional HMOs (p. 1).
Although this Solicitation specifies minimum requirements for the composition of a collaboration, Bidders should understand that the State is looking for the most comprehensive models that take a holistic approach to individuals served and attempts to coordinate services for all of their needs. The State encourages models that attempt to coordinate social services beyond those covered by the Medicaid program (p.1).
In response to this solicitation, Heartland Health Outreach, a component of Heartland Alliance, took the lead in assembling potential partners and setting forth a vision of how the partners could collaborate to create a Care Coordination Entity that served the people the partners were already serving--seniors and persons with disabilities with the most complex and interacting needs, including those who had chronic patterns of homelessness. The selection of T4H and four other Care Coordination Entities was announced in mid-September 2012.
7.4.1. Governance Structure During Development and After Award
The 37 organizations involved in developing the T4H proposal came from all parts of Chicago and included Erie Family Health Center, AIDS Foundation of Chicago, Thresholds, Cook County Health and Hospital Systems, Northwestern Memorial Hospital, Lutheran Social Services, the Alliance of Chicago Community Health Services, Mercy Housing Lakefront, Heartland Human Care Services, and many more.
In addition to hospitals and hospital systems, Federally Qualified Health Centers, mental health, substance use, social service, and housing providers, advocacy organizations, and a pharmacy chain, the collaboration also included entities that provide training and technical assistance, data analytics, clinical decision support, and management of T4H's potential data warehouse.
Work groups for the proposal had substantive focuses, including Care Coordination, Finances, Information Technology, and a Leadership Advisory Board. Also meeting during proposal development were constituency groups based on provider type, including groups for hospitals, Health Centers, behavioral health, and social services.
Together4Health LLC
Staff of Heartland Health Outreach, along with potential partners, developed the structure by which the organization would be governed once the T4H proposal was accepted. This is a for-profit limited liability company through which each partner would own a share of the company and have the right to participate in guiding the company's development and direction. By mid-December 2012, 34 partner agencies had signed the operating agreement and paid their ownership share.
T4H LLC has a governing Board of Managers elected from among the members. Six Board committees oversee various aspects of the agency's operations--Executive; Finance; Care Coordination and Quality; Network Development and Provider Relations; Risk Policy; and Planning, Policy, and Evaluation. Working groups include Information Technology and Health Information, Marketing, Care Coordination Policy and Advocacy, Chicago Health and Social Innovation Research Group, and the Contract Negotiation Team. Constituency groups include hospitals, primary care providers, community behavioral health providers, social services providers, other member organizations (not direct services), and businesses. There are also plans to form a Consumer Advisory Board. T4H is run on a day-to-day basis by its management company, Heartland Health Outreach, which staffs the committees, working groups, and constituency groups and performs the many functions associated with each aspect of operations.
In addition to participating in the ownership structure, each partner agency has a service contract with T4H LLC. As of this study's final site visit, the Heartland Health Outreach team was developing the template for these contracts. Partner contracts will cover such things as commitments to the following:
Contribute patient data to the T4H database.
Serve a certain number of T4H clients, using funding from existing contracts or other reimbursement mechanisms, at least initially.
Make changes in their own organization so they can:
- access the T4H data system;
- work collaboratively with other T4H members in their local hub; and
- have their service staff work with the T4H Care Coordination teams to move toward integrated care.
7.4.2. Care Coordination
T4H's care coordination structure is designed to assure that consumer needs are known and their interactions appreciated, a comprehensive plan is developed, needed services are delivered, outcomes are monitored and plans adjusted as needed, and unnecessary care in crisis or emergency settings is minimized. The structure directly provides, and the Illinois Medicaid program is expected to pay for, the care coordination that we so often found was not covered in the service structures described in earlier chapters.
Care will be coordinated through a central team and also in care coordination teams located in three hubs in different parts of the city to which nearby T4H member agencies will be attached. The team at each hub will have a nurse, a mental health expert, and community health workers. Care coordination staff will be employees of T4H LLC and will coordinate with case managers and similar staff in each agency from which a member needs service.
Links to housing and supportive services to help people maintain housing are built into the care coordination function. The graphic below depicts the central team (large gray circle at upper right) and a detailed schematic of one hub.
T4H staff, which includes team members from all the hubs, does intake, population management, data analysis to monitor care delivery and outcomes, and general oversight.
The hub-based care coordination teams will work with consumers, develop individual care plans, establish a coordination team for each consumer that links care delivery staff of each member organization involved in the consumer's care, and work to assure that the plan is carried out or modified as needed. The hub teams in their role as members of the central care coordination team also have the responsibility for making the overall system work, by identifying gaps and bottlenecks and bringing them to the attention of the Health Hubs and Care Coordination and Quality Committee for resolution. For individual care coordination, the Hub teams will connect to the clinicians, case managers, and other service providers in partner agencies, who are likely to remain somewhat siloed unless, as is true for some, they already do major care coordination work. They are expected to facilitate access to and coordination of all aspects of the care an individual needs and to assure that during its delivery the person is treated holistically and the effects of each type of care on other interventions is considered and accommodated.
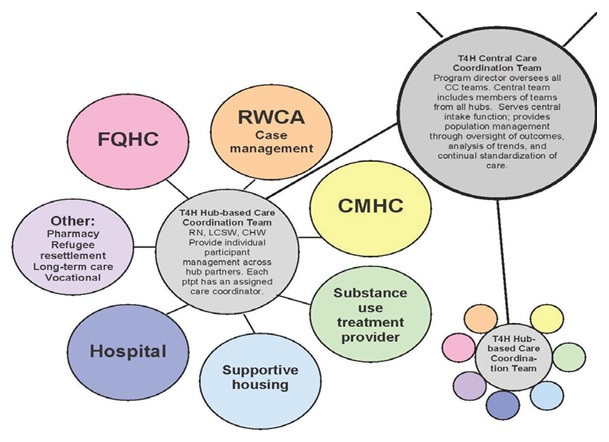
Early on, the group realized that it needed an overarching value framework to drive the entire enterprise, covering assessment, engagement, staffing, and integrated service delivery. This framework has been critical to everything that followed, providing a constant frame of reference each time the details threatened to overwhelm the whole.
Starting with its early work on the T4H proposal, the Care Coordination Work Group has focused on how these teams will function and how the hubs and the actual care provider organizations will interact. Representatives of many partner agencies have attended this work group from the beginning. Initially they shared information about their own agencies (the services they offer, what their clients need, and what gets in their way). Quite a few improvements in communications evolved just from these meetings. The group recognized how big a challenge it would be to include hospitals in this open communication--something that had mostly not happened before.
The group also recognized that many individual member agencies do a lot of care coordination work already, and often with at least some other member agencies. But more would be needed, through more formalized structures, and tied to outcomes. Inevitably this would mean that agencies would need to modify some of their own established procedures to integrate their care with other agencies and the T4H care coordination teams. Further, once the proposal was accepted and the care coordination team realized it now had to make the plans work, it became clear that intra-organizational communication had to catch up. For the most part, executive directors were the agency staff working on the T4H conceptualization and proposal. With funding, clinical and casework staff, data system personnel, privacy officers, and all manner of employees had to be introduced to the T4H concept and convinced to cooperate. For most organizations, this meant that many people who did not participate in T4H's planning phase had to now understand the T4H vision and values and become engaged in the many start-up tasks required to make the plan operational.
Collaboration between two key members of T4H, the Cook County Health and Hospital System and Heartland Health Outreach, is evolving, with several emerging opportunities for working together to improve the delivery of health services for some of Cook County's most vulnerable people. In addition to CountyCare (see Chapter 3), which enrolls people who are currently uninsured, the Cook County Health and Hospital System and Heartland Health Outreach are also partners in Together4Health.
The two initiatives will serve different target populations, at least initially, while the two provider networks include some of the same organizations. At the time of our final site visit, the Cook County Health and Hospital System and Heartland Health Outreach were negotiating an agreement to place Heartland Health Outreach staff in the emergency department at Stroger Hospital to engage people who are homeless and connect them to more appropriate care. Over the coming months and years, the organizations will likely have a complex and evolving set of relationships, sharing responsibility for coordinating care for many people experiencing homelessness and PSH tenants.
7.4.3. How the Finances Are Expected to Work
T4H's goal is to operate as a Care Coordination Entity for three years and then transition in the fourth year to operating as a Managed Care Community Network. These networks are essentially ACOs or ACO-like entities with risk-based managed care financing. T4H will use this financing to pay other providers for all covered services.
As a Care Coordination Entity, T4H receives a Care Coordination fee from the state's Medicaid program. During the first three years as T4H operates as a Care Coordination Entity, all health and behavioral health care and other services received by T4H consumers, other than the activities of the care coordination teams, will be paid for in the same way they would have been paid for before T4H. This could be Medicaid reimbursements paid on a fee-for-service basis; federal, state, or county grants and contracts; housing subsidies for supportive housing providers; and other payment mechanisms. Initially, the contract between the state and T4H LLC pays for Heartland Health Outreach's management functions and for staff of the care coordination teams. T4H has budgeted a small portion of its income from Care Coordination fees to pilot services that are expected to have an impact on client outcomes. The hope and expectation is that as care through T4H results in savings in the costs of Medicaid-covered health care and behavioral health services over the first 2-3 years of the initiative, and the state shares those savings with T4H as one component of a pay-for-performance mechanism, these revenues will be used to improve T4H's infrastructure and also ultimately to contract with its members to fill gaps in services that are not covered by Medicaid reimbursements.
But for the organizations that deliver services in permanent supportive housing and to other people with chronic patterns of homelessness, T4H will not provide an immediate solution for the gaps they experience in financing the services they deliver. While this reality caused some tensions and debate during the planning process, the partner organizations that provide services to people with chronic patterns of homelessness recognize that they need to participate as co-owners of T4H as it develops; they need to have a seat at the table and work within the organization to figure out how services in PSH will be financed as new ways of delivering and paying for health care emerge over the next few years.
While this case study was underway, the state was expecting to amend its state Medicaid plan to use the health home option, available under the Affordable Care Act, to provide Medicaid reimbursement for the Care Coordination fees it pays to Care Coordination Entities, including T4H, to cover management functions and care coordination. As of early 2014, the state had not yet submitted a state plan amendment to CMS to add a health home benefit, and was considering other Medicaid financing approaches to cover these costs. Existing Medicaid benefits will still pay for other covered services in the usual way, including hospitalizations, nursing home stays, and community mental health services, outside the Care Coordination Entity framework.
The state expects to realize savings when care coordination leads to fewer or shorter hospitalizations and nursing home stays and lower related costs. The expectation is that savings in hospitalizations and other health care costs will be comparable to (or greater than) those the state achieves through other types of managed care arrangements, with appropriate risk-adjustment to reflect differences in the characteristics of people enrolled in each Care Coordination Entity. Ultimately, subject to CMS approval, the state expects to return a portion of those savings to T4H as part of a pay-for-performance mechanism that will also incorporate quality measures. T4H may use the funds to expand infrastructure, purchase types of care that would otherwise be unavailable, distribute some funds to members, including incentive payments for achieving targets for volume and quality of services and outcomes, and so on, as the Board of Managers decides.
T4H financing is based on the organization receiving a per-consumer monthly care coordination fee from the Department of Healthcare and Family Services for all enrolled members, regardless of the specific services the consumer actually receives. A great deal of the work leading up to the T4H proposal involved analyses to determine whether T4H could afford to do what it wanted to do--it had to develop a defensible expectation of how much that fee needed to be.
With foundation support, Heartland Health Outreach was able to hire an actuarial firm to help analyze the state Medicaid claims data to develop a realistic fee proposal. The analysis required the firm to take everyone in the Medicaid data living within a certain geographical area who was a high user of covered services, look for top diagnoses, top expenses, and similar information, and map these against the types of people that T4H was expected to target. The firm looked at service use patterns, diagnostic codes, age, and various social determinants of health such as poverty and neighborhood.
Four target groups emerged from this analysis for purposes of setting rates for care coordination fees: (1) Medicaid-only with serious mental illness; (2) Medicaid-only without serious mental illness; (3) dualeligibles (Medicaid and Medicare) with serious mental illness; and (4) dual-eligibles without serious mental illness. Initially, the state has allowed T4H to enroll only people in the two Medicaid-only groups, and T4H has not been permitted to enroll people who are dual-eligible for both Medicaid and Medicare.
Actuaries combined the Medicaid claims data with data from years of Heartland Health Outreach records for the types of clients T4H would be targeting. The analysis was also informed by publications by the Corporation for Supportive Housing that summarized research findings of cost reductions in crisis and emergency health services once people experiencing homelessness are stably housed. The actuaries used the data to stratify the likely T4H population into risk categories and attach likely savings from care coordination. Also, using Heartland Health Outreach data, they looked at service, cost, and use patterns for each of the T4H target groups and projected them by quarter for all 12 quarters of T4H's first three years, during which T4H is expected to function as a Care Coordination Entity. These actuarial analyses were used to justify the T4H cost proposal to the state.
Costs that T4H has identified to start up and operate as a care coordination entity, and considered in developing its cost proposal to the state include the following:
The Care Coordination Teams.
Information technology--the data supports, infrastructure, software, and staffing to run T4H's integrated data system (being developed).
Running T4H--management through Heartland Health Outreach, which contracts with Heartland Alliance for some services.
Ongoing actuarial analyses for many purposes.
The budget covering these activities is for running the company, not for development costs and not for any of the costs to transition to operating as a full-risk Managed Care Community Network entity or Accountable Care Organization.
T4H has already benefited from substantial foundation support to pay for start-up costs, including work with consultants (such as the actuarial firm that did the cost analysis) to help it develop its design and strategy. In addition T4H received valuable pro bono legal assistance to create the LLC and its governance structure, including operating agreements.
T4H will be trying to gain access to other resources, aiming at state-only funds designated for serving Medicaid populations. Currently, funds are technically available but restricted, and some programs pay for services that might be more effective if better integrated and aligned with other benefits. T4H member agencies will advocate for redirecting some funds that are currently administered by state agencies and allocated to T4H member organizations to be used by T4H with fewer restrictions on who can receive care using these dollars. Potentially some of the state funding can be used for federal funding match for services that could be covered through Medicaid. Foundation grants and commitments from social investment funds are other funding options T4H is pursuing to augment available resources to invest in infrastructure.
7.4.4. Information Technology and Data Sharing
One of the greatest challenges any care coordination or integration effort faces is assuring that patient information can be shared easily and accurately, while also fully respecting data privacy and confidentiality. Performance monitoring and outcome measurement is a second, hugely important use for good information, without which individual agencies and the system as a whole cannot document the benefits of coordination and integration. With these imperatives in mind, the T4H partners established a Health Information and Information Technology Work Group.
As would be true for any group of agencies, the T4H members use a variety of data systems, none of which were interoperable before T4H began. These include Centricity (a GE product), Epic, ClientTrack, and Service Point (HMIS). In addition, Illinois state agencies are in the process of developing the Illinois Health Information Exchange to comply with Affordable Care Act requirements. The Illinois Health Information Exchange will be: (1) a central repository containing a master patient index of anyone who gets care anywhere in the state; and (2) a conduit through which information can move among health care providers. It will not, however, be a data warehouse. T4H will have access to this state data structure once it is up and running. Current plans for the Illinois Health Information Exchange do not include providers of behavioral health care services, although the state may be using SAMHSA grant funding to add some capacity for shared data, including a core data set and information about behavioral health care that could be important in planning care transitions. Illinois state law contains some data privacy provisions that create barriers to sharing some behavioral health information, and efforts are under way to modify some provisions that are more restrictive than required by federal law or regulations.
T4H is working to establish a centralized data warehouse system where multiple types of data will reside and be available to partners. T4H has purchased a care coordination software and data analytics package that will be integrated with claims data. Eventually the warehouse will have the capacity to pull clinical data from electronic health records maintained by T4H member organizations. The T4H central data system will take both clinical and financial data, and will have the capacity to send routine reports to member organizations and also to respond to specific requests.
T4H has put in place an integrated tool and process for care coordination assessments. The assessments done by T4H care coordination teams do not duplicate information gathered by T4H providers, but rather focus on care coordination needs. These assessments will be electronic and available through the data system. T4H members will thus be able to share information across partners, with the appropriate broad consents and releases.
T4H has ambitious goals for its data system, hoping that eventually it will support care coordination, avoiding duplication and simplifying the client's life by consolidating care in fewer places (e.g., if it turns out that a client gets care from agencies in two different hubs, seeing if the client wants to switch to have everything come through one hub, which would be geographically more concentrated and easier to access).
The Health Information and Information Technology Work Group has a huge amount of work to do, but it has a coherent strategy and the envisioned system will provide major advantages to all T4H members. The devil will, as always, be in the details.
7.5. Housing for Health
The Los Angeles County Department of Health Services is responsible for running the county's seven hospitals and associated clinics and contracting with and supervising scores of other health care providers that are part of its health services safety net.
The availability of federal funding for health care services covered through Healthy Way LA under the terms of California's Medicaid waiver (described in Chapter 3) has freed up some of the county funding that was paying for uncompensated care in county hospitals and clinics. This has created opportunities for the Department of Health Services to invest in innovative programs to better respond to the health needs of some of the county's most vulnerable residents, including people experiencing chronic homelessness. The department's director came to Los Angeles after serving as the director of the San Francisco Department of Public Health, where he had provided leadership in creating the Housing and Urban Health Section and the Direct Access to Housing (DAH) permanent supportive housing program. That program uses a housing-first approach to provide PSH to more than 1,000 people who were previously homeless. The San Francisco experience demonstrated the potential for using housing to reduce avoidable hospitalizations and improve health for vulnerable people experiencing homelessness.
7.5.1. Care Coordination and Housing Stabilization
The Los Angeles Department of Health Services is working to create thousands of housing and other residential options through Housing for Health, including but not limited to PSH, for people who are homeless and who receive care through department hospitals, clinics, and community partners. The team believes that the system needs both permanent housing and temporary housing options with varying levels of support, including medical respite or recuperative care, PSH that incorporates a housing-first approach, interim housing where people can stay while completing the application process for permanent housing, temporary housing for people experiencing a short-term crisis, and licensed residential care for those who need more-intensive care and supervision.
The team has been exploring many options for acquiring housing for the people to whom the department gives priority status. The team is talking with nonprofit housing developers and others who may have an appropriate housing or residential option for people experiencing homelessness served by the county's health care system. In exchange for access to housing opportunities, the department commits to attaching appropriate supportive services to each unit. This offer is very attractive to PSH developers and operators, who often find it difficult to get the flexible, ongoing funding needed to deliver supportive services to their tenants.
Funding from the Department of Health Services budget will be used to establish contracts for both property management and supportive services (Housing for Health will not pay for the cost of housing itself). The department used a Request for Qualifications process to select and prequalify vendors with the capacity to deliver one or both types of services, and established master contracts with eight companies for property management services and about 20 service provider organizations with experience working with people in supportive housing. Once housing becomes available and the Department of Health Services places its priority people into it, the department adds specifics to those master contracts, entering into agreements for the number of people to receive supportive services or the number of units to receive property management services.
This just-in-time approach to putting property management and supportive services in place contrasts with the usual time frame for real estate transactions, which can be slow and unpredictable.
The first Housing for Health PSH units were created by attaching department-funded service teams to tenant-based Housing Choice Vouchers designated for chronically homeless persons. The city and county public housing authorities have allocated Housing Choice Vouchers to Department of Health Services use, and the department also partnered with the city's housing department to acquire and renovate about a dozen small apartment buildings or houses that were in foreclosure, containing a total of 56 units. People experiencing homelessness and prioritized by the department will occupy these units, with supportive services provided by one of the agencies under a contract with the department.
Other short-term and permanent housing options, including several PSH projects, are in development or on the drawing board. The Department of Health Services hoped to have about 1,000 units of housing available by the end of 2013. The department has also negotiated with the city housing department to include provisions in its funding competitions for PSH projects to require developers to set aside housing units for people experiencing homelessness who are referred by the department, the Los Angeles County Department of Mental Health, or the Department of Public Health's substance abuse treatment system. These housing units will become available starting in 2014.
When the local public housing authorities had to stop issuing new housing vouchers because of federal funding reductions (due to sequestration) in early 2013, this slowed progress in expanding the Housing for Health program. Working in collaboration with other government partners, including the Los Angeles County Board of Supervisors and the Conrad N. Hilton Foundation, in February 2014 the Department of Health Services launched a new $18 million Flexible Housing Subsidy Pool to provide housing subsidies lined with wraparound intensive case management services for at least 2,400 persons.92
To identify residents for referral to the Housing for Health program, the department is working with a group of Designated Referral Entities, including four of the county's hospitals, the county's large ambulatory care centers, and designated county clinics and recuperative care programs. As more units of housing become available, Community Partner clinics that serve people experiencing homelessness will also become referral entities. The program's primary target population is people experiencing homelessness who are extremely vulnerable because of their health conditions or who are frequent users of county hospital emergency rooms or inpatient care.
The Department of Health Services also participated with community-based housing and service providers in a pilot coordinated entry initiative for Skid Row. One of the goals of the coordinated entry pilot was to align multiple systems for prioritizing vulnerable people and develop a strategy for linking them to the housing option that best matches their needs, taking into consideration applicable eligibility criteria. With support from the United Way and a network of public and private funders and other agencies involved in the countywide Home for Good campaign, efforts to implement a Coordinated Entry System were later expanded beyond Skid Row in late 2013. In early 2014, the Home for Good Funder Collaborative provided funding to expand the Coordinated Entry System to all areas of Los Angeles County. Some funders, including the Housing Authority of the City of Los Angeles, are beginning to require that new PSH units or vacancies be filled with people who are referred for housing from the local Coordinated Entry System.93
The Department of Health Services is now working to align or balance several strategies for prioritizing people for housing opportunities in the Housing for Health Program, including those who are prioritized by the emerging Coordinated Entry System, those who have been identified by the Designated Referral Entities, and those who are being served by a program that is identifying and engaging the most frequent users of hospital care and other high-cost services.94 With time, experience, and an expanded supply of housing options, the hope is that trusted partners will be able to work out a shared approach to finding the best fit between homeless people with the greatest needs and the available housing options.
In the short term, department leadership is committed to the idea that some of the resources in the county's large system of hospitals and clinics can be better used to finance some of the costs associated with PSH for people who would otherwise have frequent and avoidable emergency room visits, inpatient hospitalizations, and stays in other high-cost settings, including jails and nursing homes. The future financing strategy for this approach is still uncertain, in part because it is not yet clear how Medicaid managed care plans (discussed in Chapter 6) or capitations the department receives from the managed care plans can contribute to paying for the services in PSH.
7.5.2. How the Finances Work
The Department of Health Services uses departmental (county) resources to pay for property management attached to the buildings where its dedicated units are located and for supportive services, including intensive case management for each tenant it places in one of its dedicated units and some nursing services. While keeping the same budget of about $4 billion a year for its hospital and clinic system, the department leadership team is working to improve the whole system's efficiency and effectiveness, make more appropriate use of hospitals, and make the funding go farther, provide better care, and achieve better patient outcomes. The new director was able to obtain a favorable approval structure from the county Board of Supervisors, including the authority to negotiate master contracts and make other arrangements for service delivery. Thus the department can do what it feels is needed for several years, without returning to the Board for approval for specific items or strategies.
Most of the resources being used for Housing for Health were already in the departmental budget, where they were covering the costs of care delivered in the department's health service facilities that were not reimbursed through insurance.
The advent of Healthy Way LA and its federal Medicaid match for the costs of care, freed up some of those local resources, making them available for the department to cover the cost of the supportive services that it expects will contribute to major reductions in spending for emergency department use, hospitalizations, and rehospitalizations because a person's homelessness interfered with getting appropriate follow-up care after an inpatient episode.
7.5.3. Information Technology and Data Sharing
The Department of Health Services is committed to incorporating two data technology tools into its operations. The first was well on its way during the study--an Electronic Medical Records system and patient registry that was being rolled out to all primary care clinics. This is an electronic tool that tracks everything a provider might want to know about a patient. It is used to prepare for each patient visit wherever the patient might receive care, to review case history, and to let anyone dealing with the patient know what is happening in all aspects of the patient's care.
The electronic medical records system will be used for quality assurance, and to establish the baseline for outcomes. In addition, it can help to make the case for how housing and other practices are stabilizing clients, and rationalizing the system of care. The system will finally bring all Department of Health Services components into one unified system that uses the same data fields and data definitions and can share information across components. This will be a vast improvement over the historic reality of the department's seven different computer systems that did not talk to each other, used the same data fields but not the same coding categories within fields, and had important information in nonelectronic notes.
The second electronic tool is the e-consult, which the department had already begun to roll out at the time of our last site visit in January 2013. The department's own primary care clinics and the jail were using it, and some partner agencies were using it as well. Staff like e-consult because it gives a primary care physician almost immediate access to a specialist. The primary care doctor sends the specialist all the case information, the specialist evaluates it and either sends back recommendations for care or decides that the situation is urgent and that the patient should see the specialist immediately. If the latter, there is no long wait for an appointment and the specialist has immediate access to all the relevant information. The specialist can order tests to be done before the consult, or could suggest another specialist if appropriate.
Departmental staff said they did not know how well e-consults will work with people who are homeless because it is not certain they would return for further treatment, but even the information gained during the initial meeting should be of value to the patient as it would give the primary care physician a better sense of what to do for the patient.
7.6. Summary
This chapter has examined three emerging models for the kind of integrated and coordinated care that evidence shows has promise for people with complex needs and histories of chronic homelessness. The ACO model is based on diverse participating providers addressing needs holistically and sharing savings from improved efficiency and quality of care.
Hennepin Health, Together4Health, and Housing for Health are in the early stages of implementation, but each offers lessons for what it takes to create a provider organization across a large and diverse metropolitan area with differing needs and capacities across the service area. Hennepin Health is countyrun, as is Housing for Health; Together4Health (T4H) is a for-profit company made up of providers. All three examples target users of safety net services and include significant emphasis on the social determinants of health. All include homelessness as one of the social determinants; none limits participation to people with serious mental illness.
All three initiatives are designed to overcome three of the most persistent gaps in care for chronically homeless people with disabilities that we identified during this research.
First, they pay for many of the activities we sometimes call "the glue," the things that help connect people to care and ensure that they get what they need in ways that take the whole person into consideration.
Second, all cover people with and without serious mental illness--although access to specific types of Medicaid-reimbursed behavioral health care will still depend on a consumer meeting the relevant eligibility criteria.
Third, the models include the full extent of services a chronically homeless person or PSH tenant with complex and interacting health and behavioral health conditions might need, from primary care to specialty care to mental health and substance use disorder treatment to social services and housing (although no single source pays for all of these in any of the models).
8. Challenges and Opportunities
Chapter 8 Highlights
Olmstead. In 1999, the Supreme Court issued a decision in Olmstead that prohibits the unjustified segregation of people with disabilities. This decision was made based on an appeal of a case brought on behalf of two women in Georgia who alleged that their rights under Title II of the Americans with Disabilities Act (ADA) were violated.
The ruling creates a mandate for states and other public entities to reduce the isolation and segregation of people with disabilities in institutional settings and instead provide community-based services. It requires that people with disabilities be housed in "a setting that enables individuals with disabilities to interact with nondisabled persons to the fullest extent possible."
Lawsuits brought based on Title II of the ADA and Olmstead are stimulating Medicaid and other state agency officials to re-balance their long-term care systems and expand the availability of home and community-based services linked to housing and employment for people with disabilities who were institutionalized or at-risk of institutionalization.
Depending on the alleged violations and rulings, states are typically obligated to expand housing resources for the affected class. This presents significant challenges to states. These challenges include: (1) the sheer availability of supportive housing units, which may not be sufficient to meet the level of demand created by Olmstead in addition to the needs of people not covered, including individuals experiencing homelessness; and (2) the requirement that new resources be developed in the most integrated setting possible.
Despite the challenges, states and community providers have been working hard since Olmstead to develop financing strategies for delivering the services and supports called for by the court decision. Medicaid's home and community-based services are often an essential part of these strategies, including waiver services authorized under Section 1915(c) and state option services authorized under 1915(i).
Efforts to meet the requirements of Olmstead can be reasonably well-aligned with efforts to reduce chronic homelessness, or they can be separate efforts that reflect competing visions and values. Two case study sites, Louisiana and the District of Columbia, have followed the first path, while three others--California, Minnesota, and Illinois--have followed the second. In these latter cases, approaches to financing and organizing housing and services for people with disabilities coming from homelessness and those living in institutional settings are not well-aligned.
Workforce Capacity. As expanded eligibility swells the Medicaid rolls, newly eligible people may find it difficult to locate a provider or get care in a timely manner, due to a shortage of primary care providers as well as providers of specialty medical services. To translate coverage into meaningful access to care will require not only more medical providers in some communities, but also changes in the ways that health care is delivered to improve efficiency and the quality of care.
Team models using personnel such as nurses and community health workers as "care extenders" are likely to be important strategies.
Training, skill development, upgraded credentials, and increased supervision are likely to be needed to safely respond to some people's complex medical and behavioral health conditions. Movement to begin these processes is already under way in many places.
Increasing emphasis on care coordination and multidisciplinary team approaches create another challenge, as even highly trained clinicians rarely learned to work across disciplines or as members of teams.
Gaps. Current gaps in services include the need for more flexibility in services to address substance use disorders, alone and in the context of co-occurring medical and mental health conditions; and the need to address challenges in serving "dual-eligibles"--those who receive both Medicare and Medicaid. These challenges lie primarily in aligning the very different payment mechanisms and covered services between the two programs.
New Opportunities. Health homes under the Affordable Care Act, with federal funding at 90 percent for the first two years of operation, offer an important new opportunity to incorporate care coordination services for people with complex health needs into Medicaid state plans. Some states are also working with CMS to find a way to include housing stabilization services as a covered benefit.
8.1. Introduction
Preceding chapters focused on a specific care delivery strategy and discussed the Medicaid benefits and financing mechanisms. During the study, we also encountered issues of a more general nature that will affect developments regardless of which service delivery and Medicaid financing mechanisms are chosen. Actions and decisions related to the Supreme Court's 1999 Olmstead decision are one of these, directly affecting programs in several of our case study sites and potentially affecting every state and community in different ways.
A second global challenge is workforce adequacy--whether enough and the right kinds of workers will be available to serve the newly eligible Medicaid population in general and special needs populations in particular. Additional global challenges concern two special populations: people whose disabling health conditions and challenges to housing stability are primarily related to substance use disorders, for whom there are relatively few Medicaid-covered services available in PSH, even for Medicaid beneficiaries, and recipients of both Medicare and Medicaid (dual-eligibles), for whom service coordination is extremely difficult despite coverage by two health insurance programs.
We also identified approaches with particular promise that are still on the drawing board or were submitted to CMS and awaiting approval or comment during the study period. Most of these involved designs for health homes to serve persons with specific health conditions, as enabled by the Affordable Care Act. Also of great interest are the efforts of some states to include housing stabilization services as a covered benefit.
8.2. Olmstead Compliance and Consent Decrees
8.3. Workforce Capacity
In several of the communities included in this study, health care providers and other stakeholders have been thinking about the workforce implications of the expansion of eligibility for Medicaid, coupled with potential changes in payment mechanisms as states increasingly move toward managed care arrangements for financing health care. Many communities will likely experience a shortage of primary care providers, as well as providers of specialty medical services. People obtaining coverage through Medicaid and subsidized insurance in 2014 under the provisions of the Affordable Care Act may find it difficult to locate a provider or get care in a timely manner. To translate coverage into meaningful access to care will require not only more medical providers in some communities, but also changes in the ways that health care is delivered to improve efficiency and the quality of care.
Team models using personnel such as nurses and community health workers as "care extenders" are likely to be important strategies. Some of the innovative providers of health care who met with us as part of this study talked about encouraging all of their staff members and partners to "work at the top of" their credentials, and to help other team members increase their skills and take on greater responsibility for providing some services to consumers, within appropriate limits related to "scope of practice." This can be challenging, however, because Medicaid reimbursement rules can create incentives to use physicians or mid-level practitioners to deliver some services that might otherwise be provided by a nurse or other health worker, but reimbursement may not be available if services are delivered by staff members who have different types of credentials.
For organizations delivering services in PSH and those serving people experiencing chronic homelessness, this creates both challenges and potential opportunities. By reducing resources spent on avoidable hospitalizations, re-admissions, and emergency room visits, PSH frees up those resources to be used to provide access to health care for those who need it. Multidisciplinary teams can extend the reach of clinicians, and help them serve the most challenging and complex clients more effectively.
But as some communities increasingly prioritize the most vulnerable people for access to PSH, some service providers have reasonable concerns that their current staff lack the skills and credentials required to safely respond to some tenants' complex medical and behavioral health conditions without additional clinical consultation or supervision. Some service providers are adding nurses to their teams, and others are training case managers or other paraprofessional staff to be more involved in helping PSH tenants and other clients monitor their blood pressure or follow-through on other tasks related to monitoring and managing chronic illnesses such as diabetes.
Other workforce challenges arise because even highly trained clinicians are often not trained to work across disciplines or as members of teams. Primary care providers may have little training about substance use disorders or mental health, while most workers in mental health or substance use treatment programs do not speak the language of health care. Providers of services in PSH report that cross-training is important, and training on specific skills and approaches such as motivational interviewing can help to create a common language and shared approach for serving shared clients.
8.4. Coverage for Services to Address Substance Use Disorders
In states that have expanded Medicaid eligibility under the provisions of the Affordable Care Act, a significant number of adults who are eligible because their incomes are low enough to qualify (up to 133 percent of the federal poverty level) are likely to have substance use disorders. The Affordable Care Act includes services for substance use disorders as one of the ten essential health benefits that state Medicaid programs must provide to newly eligible adults; all health insurance plans that are sold on Health Insurance Exchanges must also include all ten elements.
Some states are making changes to provide enhanced Medicaid benefits to cover substance use disorder treatment services for newly eligible adults, including people experiencing homelessness, to meet the requirements of the Affordable Care Act. Depending on how states define and implement these benefits, these changes could potentially reduce some existing obstacles to the integration of services to address substance use disorders with mental health or primary care services. States could, for example, choose to cover the costs of multidisciplinary team models that provide mobile, flexible services to people experiencing chronic homelessness. Alternatively, if states continue to define and administer Medicaid benefits through separate systems for medical care and mental health and substance use disorder services, without other efforts to facilitate integration of care for people with co-occurring conditions, or for people whose untreated substance use disorders have an impact on their health and health care costs, those policy decisions may result in maintaining or exacerbating existing obstacles.
One of our case study sites is already taking action to address coverage of substance use disorder services. In 2013, with support from the governor and the state legislature, the California Department of Health Care Services decided to expand Medicaid coverage for some substance use treatment services, for both newly eligible people (the expansion population) and adults already eligible for Medicaid. Before 2014, California offered only three Drug Medicaid benefits for most adults: methadone maintenance, naltrexone for opioid dependence, and Outpatient Drug-Free Services. Other covered services included intensive outpatient treatment for pregnant and post-partum women, children, and youth; and residential treatment for pregnant and post-partum women. Beginning in 2014, California is making these additional services available to the general adult population. To qualify for Medicaid reimbursement, these services must be delivered in settings that are certified as treatment facilities.
The expansion of coverage for treatment services is expected to make it easier for PSH tenants to have access to residential treatment or intensive outpatient treatment services. However, the requirement that treatment occur only in certified facilities is expected to be an obstacle to using Medicaid to pay for services that are delivered in PSH, including the services that help to engage people whose substance use problems are a threat to their safety or housing stability and the services that motivate people to participate in treatment. Most PSH service providers are not currently certified as providers of Drug Medicaid services, although some are now working to establish programs that can meet the requirements for certification so they can tailor programs to meet the needs of the people they serve and have access to Medicaid reimbursement.
For states not expanding their Medicaid programs, serving individuals with substance use disorders will still be difficult. The major reason for the limitation in Medicaid is that persons whose disabilities are primarily attributable to substance use are not eligible for Supplemental Security Income, and as a result they will generally not be eligible for Medicaid in nonexpansion states.105 Historically, most Medicaid state plans had limited coverage related to substance use disorder treatment services.
In every case study site, PSH providers and other stakeholders involved in efforts to end chronic homelessness reported that Medicaid benefits for services to address substance use disorders are very limited, and often provide coverage only for treatment services delivered in designated facilities. This makes it extremely difficult, if not impossible, to use Medicaid to pay for some of the services and supports needed to implement a housing-first strategy for people with histories of chronic homelessness and the most severe, long-term substance use disorders. Even for persons with serious mental illness who have co-occurring substance use disorders, mental health service providers frequently describe limitations that prevent them from using Medicaid to pay for the services they deliver when they are directly addressing substance use problems. Without the ability to use Medicaid to pay for services that focus on substance use using interventions that can be delivered in PSH and other community settings, providers working with people experiencing chronic homelessness and those who are living in PSH have limited options for helping clients overcome their addictions sufficiently to get and keep the housing that is critical to their recovery and stability.
8.5. Integrating Services Under Medicare and Medicaid
Service providers working with PSH tenants and people experiencing chronic homelessness reported that a relatively small but growing number of the people they serve are eligible for both Medicare and Medicaid. These "dual eligible" individuals are among the costliest patients enrolled in both Medicare and Medicaid, and they often receive very fragmented care despite having multiple and disabling physical and behavioral health conditions and insurance coverage from both programs. Integrating Medicaid and Medicare benefits is extremely complicated, but given the extraordinary costs associated with health care for this group of beneficiaries, integration is increasingly a priority for the Federal Government and for many states.106
So far, most providers of services in PSH have not been very involved in emerging efforts to integrate care for dual-eligibles, but a few are beginning to recognize the need to do so. The number of people who experience chronic homelessness and are eligible for both Medicare and Medicaid is likely to rise as the average age among people experiencing chronic homelessness increases.
The Illinois Care Coordination Innovations project and Together4Health, described in Chapter 7, will include a focus on enrolling and coordinating care for dual eligible adults. Implementation began in late 2013.
During the study period, California was preparing to launch a demonstration program to integrate care for dual eligible adults using the state's Medicaid managed care plans and requiring greater coordination between those plans and county mental health and substance use disorder services as well as long-term services and supports. In March 2014, CMS approved an amendment to California's 1115 waiver to authorize the state to begin providing coverage under the Coordinated Care Initiative.107 Implementation will begin no sooner than April 2014 in eight counties (Alameda, Los Angeles, Orange, Riverside, San Bernardino, San Diego, San Mateo, and Santa Clara). This may create new opportunities for coordination between the managed care plans and the programs that have been funded and managed through the county mental health system. These include PSH and other services funded through the Mental Health Services Act for people with serious mental illness who are experiencing homelessness.
8.6. Health Homes
The Affordable Care Act created a new optional Medicaid benefit that states may use to create "health homes" for people with chronic conditions, including mental health conditions, substance use disorders, and chronic physical conditions.108 States may develop more than one health home benefit program for different target groups of beneficiaries. As an incentive for states to add health home benefits to their Medicaid plans, the Affordable Care Act provides an enhanced federal matching rate of 90 percent for health home costs during the first two years (eight quarters) of implementation for each defined benefit. The goal of this new benefit is to integrate and coordinate all primary, acute, behavioral health, and longterm services and supports for each beneficiary assigned to a health home, with the intent to treat the whole person.
Some PSH providers and advocates engaged in efforts to reduce chronic homelessness hope that this new benefit could provide a way to pay for a limited service benefit provided in PSH, particularly for people who have complex health needs related to chronic illness and mental health or substance use disorders.109 As of early 2014, 14 states had already received CMS approval to provide Medicaid-covered health home benefits for health conditions that are present among people experiencing chronic homelessness. However, none of the states involved in this study have yet developed state plan amendments that would create health home benefits designed to cover the services needed by people experiencing homelessness and PSH tenants; four are in the process of doing so.
In Illinois, the state expects to submit a proposal to CMS for health home benefits that would cover many of the care coordination services that will be delivered by the Care Coordination Entities described in Chapter 7, including Together4Health. State Medicaid officials have not yet begun to develop a draft state plan amendment to cover these services, and they indicated that they are reluctant to move forward too quickly because they want to ensure that when the state adopts the new optional benefit, a sufficient number of people will be ready to enroll in health homes to make the best use of the opportunity for a higher federal matching rate during the first eight quarters.
California received a federal planning grant to begin developing an approach to covering health home services as an optional benefit. Progress on this planning appeared to have stalled in 2013, however, despite considerable interest among stakeholders. This stall was due, in part, to state officials' focus on tasks related to preparing for the expansion of Medicaid eligibility in 2014, on planning for implementation of the Coordinated Care Initiative, and on other efforts related to implementation of the Affordable Care Act. Advocates for supportive housing and health care for people living in poverty, including people experiencing homelessness, worked hard to help pass legislation authorizing the state's Department of Health Care Services to design and seek federal approval for a health home program consistent with federal law, if this can be accomplished without any cost to the state. The governor signed this legislation in 2013. The legislation directs the state to target health home services for persons with chronic co-occurring physical health, mental health, or substance use disorders that are prevalent among frequent hospital users and persons who meet additional criteria to be developed by the department using one or more of the following indicators:
- Frequent inpatient hospital admissions, including hospitalizations for medical, psychiatric, or substance use related conditions.
- Excessive use of crisis or emergency services.
- Chronic homelessness.
The legislation provides that local governments or foundations would be responsible for covering the nonfederal share of costs for these services, if permitted under federal law. One foundation, the California Endowment, has offered to provide funding to cover the nonfederal share of costs for the first two years of implementation if California implements Medicaid health home services.
In January 2010, before the Affordable Care Act became law and as directed by state legislation enacted in 2008, Minnesota created a rule related to health care homes (also known as medical homes). The state established standards and criteria for certifying health care homes as part of a statewide, multipayer initiative.110 Minnesota's approach to health care homes is informed by the recognition that a small percentage of patients drive a large percentage of health care costs. The state legislation directed the state to consider psychosocial risk factors in addition to diagnoses in setting rates for health care home services as part of contracts with managed care plans. As a result, there is a "complexity-adjusted" payment methodology for certified health care homes, with higher rates paid for services provided to persons with serious mental illness and those whose primary language is not English, as well as for persons with multiple chronic health conditions. Currently there is no adjustment for homelessness or other risk factors, such as serious substance use disorders or involvement in the criminal justice system, although those circumstances are recognized as having an impact on consumers' needs for health care home services.
For Medicaid managed care plans, the highest rate paid for health care home services is a little more than $60 a month.111 State officials recognize that this is "a drop in the bucket" compared with the cost of delivering the services needed by the most vulnerable and complex individuals, including those experiencing chronic homelessness. Currently these services are not covered as Medicaid health home services under the optional benefit created by the Affordable Care Act, although the state has received a federal planning grant and may be exploring the opportunity of obtaining the enhanced federal match that would be available if the state pursues this approach. The Minnesota Department of Health also created a statewide learning collaborative that convenes "Learning Days" for health care homes and state agencies to exchange information and enhance their understanding of best practices.
The District of Columbia received a federal planning grant to develop a health home benefit for persons with mental illness and those with HIV/AIDS. People experiencing homelessness are not a specific focus of planning for these benefits, but could be included if they have the covered health conditions. The local government agency with primary responsibility for PSH and efforts to end chronic homelessness had not been engaged in this planning process during the study period.
Connecticut and Louisiana were not engaged in planning or developing Medicaid health home benefits during the study period.
8.7. Minnesota Medicaid Waiver Proposal Included Housing Stabilization Services
While many of the financing and service delivery approaches described in this report have significant implications for the services available to people experiencing chronic homelessness and PSH tenants, including services that are delivered in PSH settings, for the most part the Medicaid benefits we have described were not specifically designed to cover the services that focus on helping people get and keep housing. In August 2012, Minnesota submitted a proposal to CMS for a Medicaid 1115 waiver to implement the state's Reform 2020 Medicaid reform package. The waiver proposal, which emerged from months of planning by state agency officials and stakeholders, contained several proposed changes to Minnesota's Medicaid program as part of a demonstration program, including a new Housing Stability Services Demonstration.
As proposed, the Minnesota waiver would have established a new benefit called Housing Stabilization Services, with the goal of better serving adults with chronic medical conditions who are homeless or experiencing housing instability and who frequently use high-cost medical services. During the study period, state officials, PSH providers, and other stakeholders engaged in efforts to reduce homelessness were hoping that CMS would approve this demonstration program as part of the state's waiver application, and that this would provide an opportunity to learn about the impact of housing stability services using data that can be tracked at the state level. In negotiations with CMS in 2013, state officials decided not to pursue this component of the waiver proposal because of competing priorities and concerns about meeting federal requirements related to cost neutrality in the federal Medicaid program. State officials and stakeholders were disappointed, but hoping to find another way to use Medicaid financing to cover the proposed housing stabilization services. They are considering other approaches, including the possibility of creating an optional benefit under Section 1915(i) similar to the approach taken in Louisiana to cover some of the services in its Permanent Supportive Housing Program.
The Minnesota proposal remains an interesting example of an approach to using a Medicaid waiver to provide coverage for services that support housing stabilization for people with disabling health conditions who experience homelessness. As it was proposed in the state's waiver application, for some PSH service providers and residents, the new housing stabilization benefit would take the place of the payment mechanism for services currently funded through Minnesota's Group Residential Housing program. Group Residential Housing is now funded by the state without any federal match. For other program participants, including people who are currently experiencing homelessness, the proposed new benefit would expand access to services in PSH. The state proposed defining eligibility for the new service using risk factors that indicate functional need rather than relying solely on specific diagnoses. The target population for housing stability services includes two groups of Medicaid recipients. The state proposed providing this benefit to 1,500 people in each of these two groups:
Target Group One: Homeless, using a definition that is consistent with the HUD definition of homelessness (including people living on the streets or in shelters, as well as people who are exiting an institution after a stay of less than 90 days if they had been living on the streets or in shelter before entering the institution) and eligible for the state's General Assistance program based on illness, incapacity, SSI/SSDI pending or appealing denial, or advanced age.
Target Group Two: Aged, blind, or disabled people who are eligible for benefits provided by the state's Group Residential Housing program and living in Group Residential Housing "conforming settings"--meaning "a housing and services establishment" (as defined in state law) that usually includes five or fewer beds or uses scattered housing locations--for which Group Residential Housing is paying for services. For these projects or housing units, the Medicaid benefit would replace Group Residential Housing-service rates now paid by the state.
The housing stabilization service benefits proposed in the waiver would include service coordination activities designed to facilitate stable health and well-being across multiple systems including medical, mental health, chemical health (substance use), employment, and legal. Service coordination activities would include assessment, service plan development, connection and coordination of services and benefits, monitoring, personal advocacy, transportation to appointments, and assistance with application for benefits. The package of benefits would also include one or more of three additional components:
Outreach/Inreach services to identify eligible people, complete a risk assessment, engage them in a trusting relationship, provide stabilization services to address immediate and basic needs, and transition them to resources and supports to address ongoing needs.
Tenancy Supports including housing navigation to identify individual housing needs and preferences, assess barriers and develop a person-centered plan for getting and keeping housing, provide assistance to overcome barriers, and help with searching and applying for housing and negotiating with landlords, setting up a household, understanding tenant responsibilities, budgeting and financial education, and negotiating conflicts with landlords and neighbors.
Community Living Assistance to support basic living and socialization skills, household management, medication education and assistance, monitoring of overall well-being and problem solving, and tenancy stabilization supports.
The budget assumptions in the waiver proposal reflected a per-person monthly rate of $600 for these services. The state budget staff used the findings from peer-reviewed research on the impact of PSH to estimate the cost savings associated with reductions in the use of other Medicaid-reimbursed health care (such as hospitalization). They estimated that housing stabilization services would be associated with a reduction averaging 25 percent of other Medicaid costs, calculated on a per-member per-month basis using cost data from the Minnesota Medicaid program for beneficiaries who are in the two target population groups. The analysis also included a lag time from the initiation of services (and costs) to achieving savings. Based on available data, estimates of health costs and potential savings are greatest for members of group one, which includes people who are homeless and not yet receiving services or housing through the state's Group Residential Housing program.
During the study period, while government officials and PSH providers were waiting for CMS to respond to the state's waiver proposal, many details had not yet been worked out. Providers of services in PSH had plenty of questions about how the benefit would be implemented if approved by CMS, and state officials were beginning to engage stakeholders in discussions about provider qualifications, more detailed service definitions, and state expectations for the quality of services. The proposed housing stabilization services benefit and payment mechanism was expected to be a significant change for many PSH providers who currently receive funding through the Group Residential Housing program. With the existing Group Residential Housing funding mechanism, the state does not specify the kinds of services to be provided, and both program models and the quality of services vary significantly. State officials anticipated that some Group Residential Housing funding would remain available because some current Group Residential Housing providers do not have the capacity to become providers of Medicaid-covered services.
Many providers serving PSH tenants and their partners in local government and nonprofit intermediary organizations such as the Corporation for Supportive Housing were active participants in the planning process that helped to shape this component of the state's Medicaid waiver proposal, and they are likely to stay involved in efforts to find other ways to use Medicaid to cover these proposed benefits. They believed that the proposed housing stabilization services would address the needs of people experiencing chronic homelessness. One limitation of Group Residential Housing has been that PSH service providers are paid only when a person is housed, while providers who work with people who have experienced chronic homelessness recognize that much work must be done before a person moves into housing and, if a person loses housing, it is important for the service provider to maintain a relationship and help the person find housing again. One big advantage of the proposed housing stabilization benefit is that it would cover services provided during the process of engagement, stabilization, housing search, and follow-through, and offer the flexibility needed to cover supports to improve housing stability and consistency of care for participants. After all of the work that went into designing the benefit and demonstration program as part of the waiver proposal, these stakeholders are likely to continue working to find a way to move forward with this approach.
8.8. Summary
This chapter has highlighted some of the challenges in providing integrated housing and services for people with histories of chronic homelessness as well as some of the opportunities to use innovative strategies to meet their needs. The next chapter includes a summary of some of the emerging practices this research has followed that show promise for meeting these challenges.
9. Conclusions
The past few years have been a time of great ferment in the health care world, with the next few years promising to see even more evolution and change. Medicaid is an important part of these changes, as states design and implement the coverage expansion aspects of the Affordable Care Act while also looking for ways to get better results from the health care delivery system and control the growth in Medicaid program costs.
For all the pressure for change, however, change comes very slowly for something as complex as health care, even as states, providers, and advocates try to be innovative and take bold steps. Medicaid is one of the most complex safety net programs, and this study's focus--how Medicaid is being and might be used to cover health-related costs for people with disabilities who have experienced chronic homelessness and need permanent housing with supportive services--is a small part of the Medicaid scene. It is, however, a very important element in the mix of assistance and supports that will help the United States end chronic homelessness, and in doing so, achieve savings in costs for avoidable hospitalizations, crisis care, and nursing home stays. This final chapter reflects on our findings and what they say about the role that Medicaid might play in the future in covering the mix of health, behavioral health, and supportive services that people need if they are to leave homelessness and improve their health status.
9.1. The Medicaid Context
This research has sought to identify the many ways that our case study states and communities are moving forward, using and modifying their Medicaid programs and health care delivery systems to better serve people with histories of chronic homelessness. Our findings indicate that Medicaid's configurations up through 2013 offered opportunities for covering a considerable array of the services needed by PSH tenants before and after they move into housing, with more possibilities becoming available through the implementation of the Affordable Care Act in 2014 and beyond.
Previous chapters described ways that our case study sites have worked with Medicaid since 2010, when this study began, to pursue innovative strategies for working with people who experience chronic homelessness and those who have moved from homelessness into PSH. They also reveal the challenges encountered during efforts to carefully articulate an integrated approach to physical health care, behavioral health care, and support services in the context of existing structures of state Medicaid programs, benefits, and provider networks. These structures have evolved over many years following priorities that also changed over time, usually within their own organizational silos. From the perspective of patients with multiple health care needs and the providers who try to treat them in a holistic manner, existing structures can be fragmented, governed by inconsistent rules and procedures, and difficult to bring together to support integrated care. The system as a whole and each patient with multiple interacting health conditions would greatly benefit from a concentrated effort by state Medicaid officials and their health care partners to bring some greater coherence to the rules and regulations, to facilitate greater continuity of care and more rational and effective delivery of health services.
While the innovations described in this chapter were all in different stages of implementation at our study's end, with none having reached a final or even a steady state, they nevertheless show promise of successfully addressing one or more pieces of the Medicaid puzzle for people with disabilities who are now or have been homeless for a long time.
9.2. The Homelessness Assistance System Context
Agencies involved in providing PSH may offer only the housing part of the package, only the services part, or both. The most common configuration is some amount of partnering, as even the providers with the most integrated and comprehensive approaches to delivering housing and services will still develop relationships with other agencies offering additional services and supports, and help link their tenants to them.
For Medicaid to be a funding source for services that PSH tenants need, the agencies offering those services must be or become Medicaid providers, the tenants must be eligible for and enrolled in Medicaid, and the services they need must be covered through the Medicaid state plan or approved waivers and available to the tenants. On the service side, most behavioral health service providers are likely to be Medicaid providers, offering supports to people whose mental illnesses, with or without cooccurring disorders, qualify them to become clients of public mental health systems. As we saw in Chapter 5, people who are homeless and meet this criterion are the most likely to benefit from services covered by Medicaid, although some of the supports they need will remain outside the scope of Medicaid and may need to be covered by other resources.
Agencies that offer mostly the housing component of PSH are rarely Medicaid providers, and appear more likely to establish collaborative relationships with one or more Medicaid providers than to become one themselves. Given the changes in Medicaid that began in January 2014, many such agencies are assessing the feasibility and value of becoming Medicaid providers themselves or strengthening collaborative partnerships with other providers who are able to obtain Medicaid financing for services they deliver to PSH tenants.
Even with collaborative relationships in place, however, different PSH tenants will have access to different levels and types of Medicaid-reimbursable services, depending on their eligibility for Medicaid and, within Medicaid-covered benefits, for specialized mental health services.
9.3. Many Alternatives Available, and Useful
Chapters of this report have described many strategies being used in our case study sites to expand and integrate health and behavioral health care under Medicaid for our target population, and often for far larger groups such as all poor people (coverage expansion waivers, Accountable Care Organization), or all people with complex interacting disabilities (Together4Health). These strategies could be used alone or in combination--most of our sites are working on more than one. We review them briefly here.
9.3.1. Health Centers
Health Care for the Homeless (HCH) programs and other Health Centers receive Medicaid reimbursement as Federally Qualified Health Centers (FQHCs). They are obvious agencies to consider as providers of health care for people experiencing homelessness. Given their mission to serve low-income people and, for HCH programs, homeless people in particular, Health Centers could be a great force for linking primary care, behavioral health, and other services and supports for people experiencing homelessness who have complex chronic conditions and those who have become PSH tenants.
The enhanced Medicaid reimbursement rates FQHCs receive seem to offer resources sufficient to work successfully with people whose health conditions are complex and require more time and coordination to address.
We saw some promising models of Health Center involvement in our research. These include co-locating FQHCs or staffing satellite FQHCs that operate for a few hours a week in or near PSH (Chicago, Los Angeles, and Minneapolis) or in offices where many PSH tenants come (District of Columbia), using multidisciplinary mobile teams (Los Angeles), and having special initiatives targeted to frequent users of crisis care (Chicago and Los Angeles). All require Health Center staff to work "outside the walls" of their clinics, collaborating with staff of housing, behavioral health, and other agencies to deliver care where people live. Several of these efforts include outreach on the streets to serve people who are still homeless.
As promising as Health Center involvement is, we learned of significant challenges facing any Health Center that wants to serve people experiencing chronic homelessness or people with disabilities and histories of homelessness who live in PSH. Contacts in the community, either on the streets during outreach and engagement or in people's homes once they are housed, are difficult for some Health Centers to fit into their business model, particularly if they have limited experience serving people with mental illness or substance use disorders who are experiencing chronic homelessness. Other Health Centers have recognized the need to adjust productivity expectations for clinicians who deliver more flexible and integrated services as part of mobile teams or in satellite clinics serving PSH tenants and people experiencing chronic homelessness, and they have made the case to state auditors and Medicaid officials to recognize that per-visit costs associated with delivering this sort of care may be higher than health care services delivered in clinic settings.
Other challenges involve making partnerships work, dealing with the shifting landscape of managed care, and covering aspects of care that are essential but often are not covered by Medicaid payments to Health Centers (e.g., some outreach and case management services). As partnerships and new models of care are being developed to integrate the delivery of primary care and behavioral health services, Health Centers face additional administrative and billing complexities, particularly if Medicaid benefits and payment mechanisms for primary care, mental health, and substance use disorder services have not been fully aligned. Health Centers in our study sites offer examples of substantial progress in overcoming these challenges to develop strategies that help people who are or were chronically homeless to become Medicaid beneficiaries and to provide them with needed care both before and after they obtain housing.
Mental Health Care Systems
People experiencing homelessness and PSH tenants for whom providers are most able to access Medicaid coverage for needed services are those with mental illnesses serious enough to result in extensive functional impairment. All case study sites had well-developed systems of care under Medicaid's rehabilitative services option, and some also used other Medicaid provisions to support the care needed by PSH tenants and people experiencing chronic homelessness if they have serious mental illness.
Mental health agencies in case study sites offer their homeless, formerly homeless, and never-homeless clients a wide range of services. Eligibility for specific types of services depends upon the client's diagnosis and level of functioning. Each study site offers a range of mental health services that provide flexible and individualized supports and are often used to serve people in PSH. Called different things in different states--Community Support Services/Teams, Adult Rehabilitation Mental Health Services, Field Capable Clinical Services, Assertive Community Treatment, and Full Service Partnerships--all are intended to provide supportive services to keep people stable in the community and restore skills and functioning impaired by mental illness. As states have defined these benefits and service models, some have included provisions that allow or require delivering services in a range of "natural" settings outside of clinics or treatment facilities, and using staff who have personal experience with mental illness and recovery to provide peer support, with appropriate clinical supervision. Targeted case management, another Medicaid option, is used in some states to cover the services needed to help people with complex health conditions and histories of homelessness get housing and other benefits.
All case study sites reported similar challenges with providing full and appropriate care to even this bestserved population. The good news is that state Medicaid offices and service providers in several sites have worked together to develop strategies to reduce or eliminate gaps in payment availability for certain types of care by working to expand: (1) the services Medicaid will cover; (2) the group that can receive the expanded services; (3) the staff that can deliver the services; (4) the locations where they can be delivered; and (5) for how long they can be delivered. Changes negotiated in some sites include simplified documentation requirements and coverage related to a client's co-occurring substance use disorder, chronic health conditions, other needs related to health, wellness, and housing stability, and care coordination. Some key services that these sites have been able to include in Medicaid coverage involve helping people find, move into, stabilize, and keep housing; going to court and otherwise helping clients with justice system involvement; and collateral contacts on the client's behalf when the client is not present. Most importantly, some of the newer approaches include the costs of case management and services integration (e.g., team meetings, case conferencing) that evidence increasingly shows are effective to treat the whole person. States thinking about how to use their Medicaid programs to support PSH tenants and people still experiencing chronic homelessness will want to consider how these strategies might best be incorporated into their own plans.
Managed Care
Managed Care Organizations (MCOs) act as administrators and coordinators of care, paying for health care delivered by providers in many different agencies with which they have contracts or through other payment arrangements. Most families receiving Medicaid have been enrolled in managed care plans for years. Recently, a nationwide movement has begun to use managed care for seniors and persons with disabilities as well, which would include Medicaid beneficiaries who are homeless and those living in PSH.
Most of our case study sites saw a lot of changes in this regard starting in 2010. In that year, Illinois established MCOs for seniors and persons with disabilities in Chicago's ring counties; California began requiring MCO enrollment for most Medicaid beneficiaries in this population in Los Angeles and most other urban counties; and the District of Columbia established early expansion under the Affordable Care Act and enrolled all newly Medicaid-eligible persons into MCOs. Minnesota began enrolling seniors and persons with disabilities in Medicaid managed care in 2011. Louisiana switched most of its children and adults receiving behavioral health care to a new statewide behavioral health managed care organization in 2012. States expanding their Medicaid eligibility in 2014 are expected to place many if not all of the expansion population into managed care, for both medical and behavioral health care.
As with all other care structures we have examined in this study, the ability of MCOs to improve service comprehensiveness and coordination for people who are experiencing chronic homelessness and people living in PSH depends on many things. These include the types of care they can provide (depending on service definitions and other provisions in the Medicaid state plan as well as provisions in state contracts with MCOs that allow for re-investment of savings), the rates they are paid, the degree to which those rates are appropriately risk-adjusted, and the availability of agencies in the community with which the plans can contract to obtain covered services.
When Medicaid MCOs operate as full-risk entities, meaning they are at risk for paying for hospitalizations and other health care costs, it is in their financial interest to establish care structures that keep use of these expensive crisis and inpatient services to a minimum. Here their interests line up with the expertise of PSH programs, which have been well-documented as doing exactly that. Mental health service providers in Minnesota say the plans covering seniors and persons with disabilities have generally been good for mental health clients, including both currently homeless people and PSH tenants. The MCOs offer transportation to medical appointments, and some also offer fitness, health promotion, nutrition, dental, and care management services for their members.
Also in Minnesota, state contracts with MCOs serving seniors and persons with disabilities allow the plans to provide "in lieu of" services--meaning some services that are not defined in the state Medicaid plan but "make sense" because of the needs of members and the potential to achieve cost offsets. One Minnesota MCO, recognizing this alignment of interests and having on its rolls a significant number of currently and formerly homeless people with complex health and behavioral health care needs thanks to the state's early expansion of Medicaid eligibility, is contracting with community agencies to provide care designed to get people into housing and help them stay there (Medicaid does not pay for the housing itself). Recognizing that "If people aren't housed they cannot focus on health care," plan representatives believe that helping people get housing now will help keep them from becoming high-cost, frequent users in the future. These calculations are paying off in reduced medical costs.
In many states separate government agencies or divisions administer benefits for medical, mental health, and substance use disorder services, each with different rules and procedures governing provider qualifications and payment mechanisms. As a result, many community providers have not developed the capacity to offer fully integrated care for medical and behavioral health conditions. To the extent that PSH service providers are engaged in partnerships and capacity-building to offer more comprehensive and integrated care and care coordination, this may create opportunities for them to collaborate with MCOs.
MCOs usually receive a certain capitated payment, per-member per-month, and must cover an extensive package of Medicaid services used by enrolled members. Rate-setting for MCOs that serve people with complex health and social needs can be challenging. State Medicaid offices and MCOs have long been familiar with rate-setting for the average Medicaid recipient--a relatively young, relatively healthy, family with children. The new enrollees in Medicaid MCOs, including seniors and persons with disabilities and some of the adults who are newly eligible for Medicaid, have quite different health care service needs and different utilization patterns, creating a much broader range of costs for people within this group. Yet little systematic or realistic adjustment to capitation rates based on the complexity of a member's health conditions has been provided so far. There is still work to do to identify the risk factors most useful for adjusting rates (in addition to the age and geographic location factors that are the most commonly used today), but it is clear that much more sophisticated differential rate-setting will be needed if MCOs and providers are to survive financially while caring for and producing better health outcomes for seniors and persons with disabilities who have more complex health needs. This also applies to persons who are currently homeless and PSH tenants who have been prioritized for access to housing because of their vulnerability and patterns of high-cost service utilization.
9.4. Accountable Care Organizations, Care Coordination Entities, and Similar Structures
Three of our case study sites--Hennepin Health in Minnesota, Housing for Health in Los Angeles, and Together4Health in Chicago--were mounting innovative approaches for the integrated and coordinated care that evidence shows has promise for people with complex needs and histories of chronic homelessness. All link Medicaid-funded services with housing and other resources to create housing-service networks. County health departments are at the center of the first two, while the third is a newly created limited liability company with a membership that includes hospitals, community clinics, behavioral health agencies, housing and supportive service providers, and advocates. All bring diverse participating providers together to address each member's needs holistically and improve efficiency and quality of care, at the same time expecting to realize savings that can be re-invested to improve the model.
Hennepin Health has been operating since January 2012, while Housing for Health and Together4Health were in the early stages of implementation at the end of this study. All offer important lessons for what it takes to pull together provider organizations of differing expertise and capacity across a large and diverse metropolitan area. All are designed to address the needs of users of safety net services and all include social determinants of health (e.g., poverty, housing) as factors their care must address if it is to help clients resolve their issues and become or remain stable community residents. All recognize homelessness as a social determinant of health, and all accept (or will accept) clients whose disabilities or care needs are primarily related to physical health conditions and substance use disorders, along with those who have a serious mental illness. All are organized to address complex and interacting needs for care and support.
These three approaches also are designed to overcome three of the most persistent gaps in care for PSH tenants and people with disabilities and histories of chronic homelessness. First, they pay for many of the activities that we sometimes call "the glue," the things that help connect people to care and assure that they get what they need in ways that take the whole person into consideration. Second, they cover people with and without serious mental illness--although access to specific types of Medicaid-reimbursed behavioral health care will still depend on a consumer meeting the relevant eligibility criteria. Third, they offer the full extent of services a chronically homeless person or PSH tenant with complex and interacting health and behavioral health conditions might need, including primary and specialty medical care, mental health and substance use disorder treatment, and solid links to social services and housing.
9.5. Olmstead and Other Challenges
9.6. Conditions Ripe for Integration, But It Will Take Work
If the promise of new and emerging approaches to integrated and cost-effective care for people experiencing chronic homelessness and PSH tenants is to be realized, many aspects of Medicaid state plans will have to be brought into alignment. Service definitions will need to be updated, examining them to assure that they can accommodate the evidence-based practices and emerging, more-integrated models of care that are particularly important for people who have co-occurring behavioral health and chronic health conditions or other medical needs. Administrative silos (involving, for example, physical health care, mental health care, and substance use disorder treatment) will have to be breached so service providers can treat people holistically, sharing medical records, requesting payment, reporting performance, and performing similar tasks through streamlined and coordinated mechanisms.
Gaps in covered services (e.g., outreach and engagement, collateral contacts, and services that explicitly focus on helping people get and keep housing as a social determinant of health and a driver of health care utilization and costs) will have to be closed to the extent possible under Medicaid, and alternative funding mechanisms identified if possible to fill those gaps. Given the enormous pressures currently facing state Medicaid agencies working to implement changes consistent with Affordable Care Act requirements, in the short term it may not be easy for them to find the time to focus on the needs of the relatively small population of PSH tenants and people still experiencing homelessness who could benefit from PSH.
Although our target population is a very small part of all Medicaid-eligible people, the population has some of the most complex needs, and it is no simple matter to design programs within Medicaid that meet those needs. For this reason, it makes sense to work with other constituencies who need home and community-based services to develop care structures that work across a wider range of populations.
Louisiana has taken an approach that seems on the verge of working for the population of interest in this research. It is concentrated in one Medicaid state plan amendment using 1915(i) authority, but it is embedded in a wholesale restructuring of the state's Medicaid system for health and behavioral health. The restructuring involves many waivers and plan amendments, and is likely to have taken at least five years by the time all the pieces are in place. The many state agencies that have participated and are still participating in this overhaul have devoted their attention to both the proverbial forest and the trees, which has provided the opportunity to determine where this target population fits in and what plan amendments are needed to allow the appropriate array of services to the range of people who need them. Minnesota did the same extensive, multifaceted planning in preparation for its Health Care Delivery System Demonstration that began in 2011, and continued those planning activities for its Reform 2020 waiver request.112
The optional health home benefit for people with chronic illnesses, a new opportunity for states under the Affordable Care Act, shows great promise as a vehicle for accommodating the care coordination needs of persons with complex health needs, including people who are or have been homeless. Several of the states included in this study were considering how to design health home services, but at the end of the study period none had completed the planning process or submitted a Medicaid state plan amendment to establish these optional benefits for a target population likely to include people who are chronically homeless and PSH tenants.
During this study, as states and health care delivery systems were preparing to meet important deadlines associated with the implementation of major provisions of the Affordable Care Act, including streamlining and expanding Medicaid eligibility and launching health insurance exchanges, we frequently heard about the "bandwidth" challenges they face. The agency leaders and planners working in state Medicaid programs, as well as other state and local government agencies and health care provider organizations, often described the need to focus their time and attention on the tasks most critical to ensuring that policies and systems would be in place by January 2014 and ready to deliver health coverage and ensure access to care for millions of Americans who will benefit from implementation of the Affordable Care Act. Simultaneously, many of these same individuals, public agencies, and provider organizations were also being challenged to implement other ambitious changes in response to budget reductions, lawsuits, and other pressures. In this context, it is remarkable that so many of them have made it a priority to work on using Medicaid to improve care for people experiencing homelessness, and to find ways to better integrate care and connect housing and services to better serve a small number of the most vulnerable people, including those with the most complex needs.
As attention focused on the activities that were most critical to being ready for 2014, stakeholders involved in Medicaid were often reminded that this has been an important deadline for some major activities, but it is not the finish line. While the enrollment of millions of Americans into Medicaid or subsidized insurance coverage began in October 2013 for coverage starting in 2014, the work of ensuring that coverage and care delivery systems work well for the most vulnerable people, including those experiencing homelessness or living in PSH, will require sustained attention in the coming years. Rather than a finish line, 2014 is a beginning of the next phase of work to achieve the goals of health reform.
References
Burt, M.R. 2008. "Evolution of PSH in Taking Health Care Home, 2004-2007: Tenants, Programs, Policies, and Funding at Project End." Oakland, CA: Corporation for Supportive Housing.
Burt, M.R. and C. Wilkins. 2012a. "Health, Housing, and Service Supports for Three Groups of Chronically Homeless People." Washington, DC: HHS/ASPE. Available at http://aspe.hhs.gov/daltcp/reports/2012/ChrHomls1.shtml.
Burt, M.R. and C. Wilkins. 2012b. "Establishing Eligibility for SSI for Chronically Homeless People." Washington, DC: HHS/ASPE. Available at http://aspe.hhs.gov/daltcp/reports/2012/ChrHomls3.shtml.
Burt, M.R, C. Wilkins, and D. Mauch. 2011. "Medicaid and Permanent Supportive Housing for Chronically Homeless Individuals: Literature Synthesis and Environmental Scan." Washington, DC: HHS/ASPE. Available at http://aspe.hhs.gov/daltcp/reports/2011/chrhomlr.htm.
Burt, M. et al. 1999. "Homelessness: Programs and the People They Serve." Washington, DC: The Urban Institute. http://www.urbaninstitute.org.
Caton C., C. Wilkins, and J. Anderson. 2007. "People Who Experience Long-Term Homelessness: Characteristics and Interventions." In Toward Understanding Homelessness: The 2007 National Symposium on Homelessness Research. Washington, DC: HHS and HUD.
Crawford, M. and S.M. McMahon. 2014. "Alternative Medicaid Expansion Models: Exploring State Options." Center for Health Care Strategies.
Kaiser Commission on Medicaid and the Uninsured. 2012. "Emerging Medicaid Accountable Care Organizations: The Role of Managed Care." Available at http://kaiserfamilyfoundation.files.wordpress.com/2013/01/8319.pdf.
Kaiser Commission on Medicaid and the Uninsured. 2013. "Community Health Centers in an Era of Health Reform: An Overview and Key Challenges to Health Center Growth." Available at http://kaiserfamilyfoundation.files.wordpress.com/2013/03/8098-03.pdf.
Lewis, V., B. Kennedy Larson, A.B. McClurg, R. Goldman Boswell, and E. Fischer. 2012. "The Promise and Peril of Accountable Care for Vulnerable Populations: A Framework for Overcoming Obstacles." Health Affairs, 31(8): 1777-1785.
Lowden, T. 2012. "On the Path to ACOs: Providers and payers test new care delivery and payment models." Minnesota Medicine (November). Available at http://www.minnesotamedicine.com/PastIssues/November2012/ACOs.aspx.
Lytle E.C., D.H. Roby, L. Lucia, K. Jacobs, L. Cabezas, and N. Pourat. 2013. "Smooth Transitions into Medi-Cal: Ensuring Continuity of Coverage for Low Income Health Program Enrollees." Los Angeles, CA: UCLA Center for Health Policy Research (April). Available at http://healthpolicy.ucla.edu/publications/search/pages/detail.aspx?PubID=1191.
Sommers, B.D., E. Arntson, G.M. Kenney, and A.M. Epstein. 2013. "Lessons from Early Medicaid Expansions Under Health Reform: Interviews with Health Officials." Medicaid and Medicare Research Review, 3(4).
Sowers, W, C. George, and K. Thompson. 1999. "Level of Care Utilization System for Psychiatric and Addiction Services (LOCUS): A Preliminary Assessment of Reliability and Validity." Community Mental Health Journal, 35(6): 545-63, http://www.ncbi.nlm.nih.gov/pubmed/10863991.
U.S. Department of Housing and Urban Development. 2012. The 2012 Annual Homeless Assessment Report to Congress.
U.S. Department of Housing and Urban Development. 2013. The 2013 Annual Homeless Assessment Report to Congress.
Wilkins, C. and M.R. Burt. 2012. "Public Housing Agencies and Permanent Supportive Housing for Chronically Homeless People." Washington, DC: HHS/ASPE. Available at http://aspe.hhs.gov/daltcp/reports/2012/ChrHomls4.shtml.
Wilkins, C., M.R. Burt, and D. Mauch. 2012. "Medicaid Financing for Services in Supportive Housing for Chronically Homeless People: Current Practices and Opportunities." Washington, DC: HHS/ASPE. Available at http://aspe.hhs.gov/daltcp/reports/2012/ChrHomls2.shtml.
Notes
PSH is a phenomenon of the 1990s and 2000s, when homelessness assistance systems evolved and their goals shifted and changed. PSH beds available to end people's homelessness went from about zero in the late 1980s to estimates of 114,000 beds in fall 1996 (Burt et al. 1999), about 188,000 beds in January 2007, and 284,298 beds in January 2013 (HUD 2013, 54).
The State of Connecticut; the District of Columbia, the State of Illinois and city of Chicago; the State of Louisiana and the greater New Orleans area; Los Angeles County, California; and the State of Minnesota and Hennepin County.
The IMD payment exclusion is in Section 1905(a) of the Social Security Act (the Act) in paragraph (B) following the list of Medicaid services. The definition of an IMD is in Section 1905(i) of the Act and in 42 CFR 435.1010 of the Code of Federal Regulations. The exclusion for individuals aged 65 and older is in Section 1905(a)(14) of the Act, and 42 CFR 440.140. The exception for individuals under age 21 is in Section 1905(a)(16) of the Act and 42 CFR 440.160. Medicaid guidance can be found at Section 4390 of the State Medicaid Manual.
42 U.S.C. § 1396a(a)(10)(B).
PSH is a phenomenon of the 1990s and 2000s, when homelessness assistance systems evolved and their goals shifted and changed. PSH beds available to end people's homelessness went from about zero in the late 1980s to estimates of 114,000 beds in fall 1996 (Burt et al., 1999), about 188,000 beds in January 2007, and 284,298 beds in January 2013 (HUD 2013, 54).
The State of Connecticut; the District of Columbia, the State of Illinois and city of Chicago; the State of Louisiana and the greater New Orleans area; Los Angeles County, California; and the State of Minnesota and Hennepin County.
Readers may find helpful background information in five papers prepared in an earlier phase of this study, which describe how Medicaid and PSH function and the terminology used (Burt, Wilkins, and Mauch 2011; Burt and Wilkins 2012, 2012a; Wilkins, Burt and Mauch 2012, Wilkins and Burt 2012). In addition, a Primer on using Medicaid to help pay for services for people eligible for or living in PSH is being published simultaneously with this report. All may be found at the end of this report or at http://aspe.hhs.gov/daltcp/reports.htm.
Final Rule published December 5, 2011, Federal Register, p.7595.
More information about the housing-first approach is available in the USICH Solutions Database at http://www.usich.gov/usich_resources/solutions/explore/housing_first.
For more information on variation in eligibility requirements, see http://www.medicaid.gov/AffordableCareAct/Medicaid-Moving-Forward-2014/Downloads/Medicaid-and-CHIP-Eligibility-Levels-Table.pdf.
Some people will still be ineligible because they are undocumented or because they have not been permanent residents for a sufficient number of years.
Connecticut expanded up to 56 percent of FPL in April 2010, the District of Columbia went up to 133 percent of FPL in July 2010 and to 200 percent later that year under an additional Section 1115 waiver, and Minnesota went up to 75 percent of FPL in March 2011. Three other states took some approach to early expansion: California in July 2011 for up to 200 percent of FPL varying by county; New Jersey in April 2011 for up to 23 percent of FPL; and Washington for up to 133 percent of FPL but only for people already enrolled in the state's low-income health plan (Sommers et al. 2013).
The Childless Adult Medicaid plan prevailed between April 2010 and January 1, 2014, when the District of Columbia adopted an Alternative Benefit Plan equal to its Medicaid state plan.
For example, Massachusetts has had an 1115 demonstration program in place since 1996 that establishes Medicaid eligibility based on low-income alone, and Maine has an 1115 program that allows it to enroll a limited number of "noncategorical" beneficiaries. In both states, people experiencing homelessness have been able to qualify and receive needed health care.
Mandatory benefits include inpatient and outpatient hospital services; nursing facility, rural health clinic, FQHC, prenatal and freestanding birth center services; physician, nurse-midwife, and certified pediatric and family nurse-practitioner services; home health, family planning, tobacco cessation, laboratory, X-ray services; and early and periodic screening, diagnostic, and treatment services for children under age 21.
Optional benefits include clinic services; prescription drugs; rehabilitative services; case management; home and community-based services as an alternative to institutionalization; physical, occupational, speech, hearing, and language therapy; diagnostic; screening; and a variety of other services that may be approved by CMS.
Alternative Benefit Plans may be based on coverage available in the private sector from large managed care plans, federal employee health coverage, the package of health insurance coverage provided to state employees, small group coverage available in the state, or the Medicaid state plan. For more information about the issues related to Alternative Benefit Plan benefits and coverage of the range of services needed by chronically homeless people, including services to address mental health and substance use problems, see this analysis by the National Council for Community Behavioral Healthcare http://homeless.samhsa.gov/ResourceFiles/Medicaid%20Benchmark%20Coverage%20Health%20Reform.pdf.
Rehabilitation helps people recover lost skills, while "habilitative" services help people acquire new ones. The difference is subtle but can be important. For example, rehabilitation can help people with schizophrenia improve social skills that allow them to resume participation in activities that had been a part of their lives before the onset of their mental illness. Assessment for rehabilitation services includes a focus on identifying the level of functioning people had "at baseline," before they became disabled. Habilitative services are services generally designed to assist individuals in acquiring, retaining, and improving the self-help, socialization, and adaptive skills necessary to reside successfully in home and community-based settings. Habilitative services can be covered by Medicaid through a home and community-based (HCBS) waiver or optional HCBS State Plan services. Habilitation is one of the essential health benefits that must be offered when a state adopts an Alternative Benefit Plan to provide coverage to people who have become newly eligible for Medicaid in 2014. States have some flexibility to determine how to design and implement these benefits and plans, consistent with rules established by the Federal Government. On July 15, 2013, HHS and CMS issued a Final Rule that includes several changes in the Medicaid program, including requirements to ensure that Medicaid benefit packages include essential health benefits and meet certain other minimum standards. This Final Rule can be found at https://www.federalregister.gov/articles/2013/07/15/2013-16271/medicaid-and-childrens-health-insurance-programs-essential-health-benefits-in-alternative-benefit#h-14.
During the study period, states were awaiting additional guidance from HHS regarding the implications of parity requirements for the package of Medicaid benefits that will be available to both currently and newly eligible groups of beneficiaries. In January 2013, CMS released a letter to State Medicaid Directors describing the applicability of parity requirements to Medicaid managed care organizations and benchmark plans. See http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SHO-13-001.pdf. Additional federal guidance is expected, and this could potentially lead to some changes in the scope of services that will be available to people experiencing chronic homelessness and formerly homeless people living in PSH.
Final regulations implementing the essential health benefit provisions of the Affordable Care Act were published in the Federal Register (78 Fed. Reg. 12834-12872) on February 25, 2013. These regulations give states significant flexibility in defining some covered benefits.
For more information about Express Lane Enrollment in California's Medicaid program see http://www.dhcs.ca.gov/services/medi-cal/eligibility/Pages/ExpressLane.aspx.
2013 SOAR Outcomes Summary, available at http://soarworks.prainc.com/sites/soarworks.prainc.com/files/SOAR_Outcomes_2013.pdf.
For further information on SOAR, see http://www.prainc.com/soar/.
The Affordable Care Act stipulates one year as the period for recertification, and states are using electronic data matching to streamline recertification and continued coverage if the beneficiary's circumstances have not changed.
For more information, see http://www.kff.org/medicaid/upload/8046-02.pdf.
According to the UCLA Center for Health Policy Research, nearly 94 percent of the state's population resides in a county with a LIHP (Lytle et al. 2013).
California's 1115 waiver also allowed the county LIHPs to include a second group of enrollees with incomes between 133 percent and 200 percent of FPL. This group of enrollees became eligible for subsidized health coverage through the health insurance exchange starting in 2014. Statewide, only about 5 percent of all LIHP enrollees fell into this group, as did less than 0.1 percent of Los Angeles LIHP enrollees.
Community partner clinics received reimbursement at the FQHC rate when they served people enrolled in Healthy Way LA.
Healthy Way LA was first established in 2007 to serve a smaller group of people with selected chronic conditions who were enrolled through a Health Care Coverage Initiative authorized by an earlier California 1115 waiver. (That waiver also made other changes to the state's approach to Medicaid financing for hospitals.) Before Healthy Way LA, the county had a unique ten-year waiver that provided Medicaid financing to support LA Department of Health Services' contracts with Community Health Centers and free clinics to provide outpatient health care services for low-income people through the Public Private Partnership Program.
In most California counties, people who enroll in Medicaid (Medi-Cal) must select or be assigned to a Medi-Cal managed care plan. In most counties Medicaid beneficiaries can choose between at least two plans, but in some counties there is only one plan. A list of Medi-Cal managed care plans in each county is available at http://www.dhcs.ca.gov/individuals/Pages/MMCDHealthPlanDir.aspx.
These challenges are described in more detail in a report published by the Insure the Uninsured Project, Preparing for the Affordable Care Act: An Examination of Coverage Expansions in LA County: Outreach, Enrollment, Retention and Utilization (January 2013) available at http://itup.org/wp-content/uploads/downloads/2013/01/LAHA-enrollment-paper-FINA2L.pdf.
With California's expansion of Medicaid eligibility in 2014, eligibility verifications became annual instead of every six months, and the process is being simplified considerably, relying on electronic verification of income as required by the Affordable Care Act.
For more information see http://www.countycare.com/files/members/CCHHS_County_Care_Fact_Sheet.pdf.
Under the Social Security Act, three types of organizations are eligible to participate in Medicaid and Medicare as Federally Qualified Health Centers. They are: (1) Health Centers that receive grants under Section 330 of the Public Health Service Act; (2) Health Centers that meet all the requirements to receive a Section 330 grant but do not receive such funding; and (3) outpatient facilities associated with tribal organizations and Urban Indian Health Organizations. The first two categories are overseen by the Health Resources and Services Administration (HRSA) within HHS and in this report are jointly referred to as "Health Centers." Health Care for the Homeless providers are a subset of those Health Centers who receive Section 330 grants. This publication does not directly address Native American providers that are enrolled as FQHCs. "Community Health Centers" are one of four distinct subsets of "Health Centers." Health Care for the Homeless grantees are a second subset; the two others are Health Centers targeting migrant and seasonal farmworkers and residents of public housing.
See http://bphc.hrsa.gov/healthcenterdatastatistics/index.html.
It is important to recognize that many Health Centers provide mental health services to meet the needs of their patients who have depression, anxiety, or other mental health disorders and who can be effectively treated in a primary care setting, but many of these Health Centers may not have the capacity to provide services to people with SMI.
HRSA, 2011 National Homeless Data, http://bphc.hrsa.gov/uds/datacenter.aspx?year=2012&fd=ho.
HRSA, 2012 National Data for Homeless: Table 4--Selected Patient Characteristics, http://bphc.hrsa.gov/uds/datacenter.aspx?q=tall&year=2012&state=&fd=ho.
These issues are described in more detail in Medicaid Coverage and Care for the Homeless Population: Key Lessons to Consider for the 2014 Medicaid Expansion. Kaiser Commission on Medicaid and the Uninsured. September 2012.
Some of these promising approaches and program models have been described in previous reports prepared as part of the first phase of this study (Burt and Wilkins 2012; Wilkins, Burt, and Mauch 2012).
LA Christian Health Center became a community partner clinic during the case study period. This status entitled the center to receive payment from the county (financed through the state's Medicaid waiver) for many of the previously uninsured people it serves who gained coverage through Healthy Way LA. In 2014, most of these people are becoming enrolled in Medicaid.
For more information see: http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/1115/downloads/ca/ca-bridge-to-health-reform-fs.pdf.
For more information see Martha R. Burt, The Skid Row Collaborative 2003-2007: Process Evaluation. Washington, DC: Urban Institute, 2007. http://www.urban.org/publications/411546.html.
Before 2014 California's Medicaid plan (Medi-Cal) provided coverage for a limited array of substance use disorder, or "Drug Medi-Cal" services, including residential treatment for pregnant and parenting women, but not for other adults. Beginning in 2014, California is expanding these substance use disorder benefits to make them available to other Medi-Cal beneficiaries who need them.
In addition to this team, described in detail here as an example, partners in the other Integrated Mobile Health Teams include Mental Health America of Los Angeles and the Children's Clinic in Long Beach; St. Joseph Center, OPCC, and Venice Family Clinic in Venice and Santa Monica; JWCH, South Central Health and Rehabilitation Program, and Behavioral Health Services in South Los Angeles; and Step Up on Second, Special Services for Groups, and Saban Free Clinic in Hollywood. Representatives from all of the teams provided valuable input for the case study.
Almost half of the project's clients are in the fifth or sixth decile, where annual costs average $22,000 or $32,000. The other participants are in deciles with significantly higher average costs.
For more information see "Hospital to Home: Triage Tool II for Identifying Homeless Hospital Patients in Crisis," Economic Roundtable, 2012, http://www.economicrt.org/summaries/10th_Decile_Triage_Tool_v2.html.
HRSA Policy Information Notice 2008-001 provides guidance to Health Centers regarding how to define the scope of project for purposes of defining the activities funded by federal grants and FQHC Medicaid reimbursements. This includes guidance regarding service sites, home visits, mobile teams or "portable clinic care," and other activities that are included in the scope of a project at locations that do not meet the definition of a service site or offer a limited activity from within the full complement of Health Center activities. For more information see http://bphc.hrsa.gov/policiesregulations/policies/pdfs/pin2008-01.pdf.
See USICH profile of Motivational Interviewing, http://usich.gov/usich_resources/solutions/explore/motivational_interviewing.
Visiting nurses for homebound patients are defined by federal law as covered FQHC services in areas where CMS has determined there is a shortage of Home Health Agencies, but this is not usually the case where Health Centers are involved in PSH. With respect to nurses, federal regulations consider only nurse-practitioners to be "essential medical personnel" capable of generating billable hours; nurses with other credentials cannot do so.
See Chapter 7 for an example of how a Chicago collaborative effort involving five hospital systems, eight Health Centers, and numerous behavioral health care and other providers is moving in this direction.
Described more fully in Burt and Wilkins 2012a.
This is in theory. In reality many requirements and barriers often make the path to becoming an SSI beneficiary long and uncertain. See Burt and Wilkins 2012b.
Our two other sites, Connecticut and New Orleans/Louisiana, had special arrangements to serve formerly homeless people with SMI living in PSH, but during this study's time period neither used Medicaid to help cover the cost of services in PSH projects. Louisiana's switch to Medicaid funding for supportive services for some PSH residents is described in Chapter 6. In Connecticut as well as in Louisiana, some PSH tenants are Medicaid recipients and thus are likely to receive Medicaid-reimbursed health and behavioral health services through clinics or programs in the community.
In California, these are referred to as "specialty mental health services," meaning the Medicaid-covered services that are delivered through county-administered mental health systems, as distinct from the more limited interventions that might be offered by a primary care provider or managed care health plan for persons with less severe mental health disorders.
See Section B.6 of Appendix B of the "Results from the 2002 National Survey on Drug Use and Health: National Findings." SAMHSA, Office of Applied Studies, National Survey on Drug Use and Health, 2002.
Illinois Department of Human Services Medical Necessity Criteria and Guidance Manual available at http://www.dhs.state.il.us/OneNetLibrary/27896/documents/By_Division/MentalHealth/brittan2/MNCGManualFinal010711.pdf.
Interviews with caseworkers in Los Angeles indicated that this happens, while some respondents reported that scores on the Vulnerability Index often reflect the same problem; people "don't tell us half of what is going on with them," with the result that their scores are too low to put them at the top of the list for getting PSH even when they really need it.
A broader range of services, including both more-intensive and less-intensive types of care, are available in some public mental health systems in addition to clinic-based outpatient care. In the District of Columbia, for example, the Department of Mental Health's Mental Health Rehabilitation Services covers diagnosis/assessment, medications/somatic treatment, counseling, community support, crisis/emergency, day services, intensive day treatment, community-based intervention (a time-limited, intensive intervention to prevent out-of-home placement), and Assertive Community Treatment, http://dmh.dc.gov/node/120742.
Lousiana's new Medicaid behavioral health managed care plan, described in detail in Chapter 6, covers these same services with a 1915(i) home and community-based services state plan amendment.
For more information about ACT, see http://store.samhsa.gov/product/Assertive-Community-Treatment-ACT-Evidence-Based-Practices-EBP-KIT/SMA08-4345.
See California Department of Mental Health, Clarification on Requirements for Full Service Partnerships (FSP) under the Mental Health Services Act (MHSA), April 10, 2009 available at http://www.dhcs.ca.gov/services/MH/Documents/FSP_FAQs_04-17-09.pdf.
See http://file.lacounty.gov/dmh/cms1_159312.pdf for LA County's Full Service Partnership (FSP) guidelines.
The others are Field Capable Clinical Services--described in the next section of the chapter--outpatient clinic services, where clients can see a psychiatrist for medications and/or receive individual or group counseling, and peer-run wellness centers, which provide support for recovery, self-management, and living with mental illness.
For more information see http://www.hfs.illinois.gov/assets/cmhs.pdf.
42 CFR 440.169.
California's MHSA Housing Program was established in 2007 with an initial allocation of $400 million of MHSA funds dedicated to the development of PSH for people with serious mental illness who are homeless or at risk of homelessness. Funding is used for capital and operating subsidies. Through an assignment letter, participating counties assign their MHSA Housing Program funds to the California Housing Finance Agency, and that agency has jointly administered the program with the Department of Health Care Services. Statewide by the end of 2013, the program has provided funding to 163 projects that include over 8,900 affordable housing units and over 2,000 units specifically housing MHSA tenants in over 40 counties. Only about $54 million of the initial allocation of MHSA funds remains uncommitted; additional funding for units is only available when counties assign their local funds to the state housing finance agency. For county mental health departments, assigning local MHSA funds to the state agency significantly streamlines the process of investing in the creation of new PSH units for their clients.
Some tenants of this organization, which offers a wide variety of mental health services, do receive their supportive services from the agency, making it an example of "one agency does both" as well as an example of "clients come with their own services."
Note that this refers to the difficulty that mental health service providers have with getting reimbursed for these scenarios under the rehabilitative services option. There may be other ways to cover such services, such as through state plan personal care or through the 1915(i) state plan option.
Chapter 4 describes similar structural challenges with regard to the involvement of Community Health Centers (FQHCs) in mental health care.
California is expanding some Medicaid benefits for substance use disorder treatment services for adults, including residential treatment and intensive outpatient treatment services, beginning in 2014. These services must be provided in certified treatment facilities. Some providers of mental health services for people experiencing homelessness are exploring the potential for obtaining certification as providers of Medicaid substance use disorder services to better meet the needs of their clients who have co-occurring disorders.
Minnesota managed care program enrollment data is available at http://www.dhs.state.mn.us/main/idcplg?IdcService=GET_DYNAMIC_CONVERSION&RevisionSelectionMethod=LatestReleased&dDocName=dhs16_141529#.
See Chapter 5 for a description of Minnesota's use of Medicaid-reimbursed TCM services as part of the supportive services in PSH for persons with severe mental illness.
California's Medicaid program is called Medi-Cal, but for consistency across all case study sites this report uses Medicaid for it and other state programs known locally by unique names.
The California HealthCare Foundation published a report describing some of these challenges and lessons learned. A First Look: Mandatory Enrollment of Medi-Cal's Seniors and People with Disabilities into Managed Care. August 2012. http://www.chcf.org/~/media/MEDIA%20LIBRARY%20Files/PDF/F/PDF%20FirstLoo....
A full discussion of risk-adjustment is beyond the scope of this report. For more information, see:
LA Care directly manages care for most of its members, but also works with several partner health plans--including Anthem Blue Cross, Care 1st Health Plan, and Kaiser Permanente--that manage care for some members who are enrolled in Medicaid. In most California counties, Medicaid managed care is implemented using a "Two Plan Model" that offers Medicaid beneficiaries a choice of health plans. Health-Net Community Solutions is the other Medicaid managed care plan operating in Los Angeles County. In some California counties Medicaid managed care is implemented through a County-Operated Health System (COHS). For more information about Medicaid managed care plans in California see http://www.dhcs.ca.gov/individuals/Pages/MMCDHealthPlanDir.aspx#lacounty.
Adult services described in the LBHP Member Handbook (p. 3) include psychiatrist, community psychiatric support and treatment, psychosocial rehabilitation, substance use disorder treatment, crisis intervention, emergency room services, and psychiatric hospital. Additional services are also available. Case conferencing and treatment planning are covered services in several of these care components.
Louisiana's Permanent Supportive Housing Program is described in some detail in a brief by the Technical Assistance Collaborative, Taking Integrated Permanent Supportive Housing (PSH) to Scale: The Louisiana PSH Program, February 2012, available at http://www.tacinc.org/knowledge-resources/publications//issue-briefs/louisiana-permanent-supportive-housing-brief/. From its inception in 2008, PSHP has offered its clients flexible supportive services as well as a rent subsidy to end their homelessness, help them maintain housing, and address their health and behavioral health care needs. Community Development Block Grant funds covered the supportive services component of the program, while Shelter + Care certificates and Housing Choice Vouchers supply the rent subsidies. PSHP staff also worked with clients to establish SSI (and therefore Medicaid) eligibility, achieving SSI beneficiary status for upwards of 80 percent of their clients.
See Chapter 5 for definitions of these service types.
SPA LA 11-13.
See Chapter 5 for description of LOCUS.
Per the CMS approval letter, p. 14, dated December 19, 2011, "This particular 1915(i) was written to support the Louisiana Permanent Supported Housing (PSH) program's goals. The PSH is by nature small, scattered-site housing aimed at person-centered planning for individuals enjoying all aspects of the community. The settings that most individuals will reside in will be PSH or other similar settings. These settings are home and community-based, integrated in the community, provide meaningful access to the community and community activities, and individuals have free choice of providers, individuals with whom to interact, and daily life activities."
Since the PSHP began, a private company, Quadel Consulting, has been entering into Housing Assistance Program contracts with private landlords, including set-aside units managed by nonprofit and for-profit tax credit development units. Quadel assigns these units as they come on line to PSHP local lead agencies according to an established plan, and the local lead agencies release them to PSHP service agencies as those agencies' clients qualify for them. Local lead agencies vary in type across the parts of the state participating in the PSHP, but are usually local offices of the state's Aging and Adult Services Department or local Human Services Authorities. None are housing agencies or public housing authorities.
As noted earlier in this report, Minnesota is one of the states that moved to expand Medicaid eligibility before 2014. Minnesota expanded eligibility to adults with incomes below 75 percent of the federal poverty level (FPL) in 2011. It further expanded eligibility in 2014 to persons with incomes below 133 percent of FPL.
While Medicaid does not have an ACO authority within statute, CMS has released guidance on integrated care models and quality considerations in Medicaid and Children's Health Insurance Program (CHIP). See for example SMDL #12-001 available at http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD-12-001.pdf, and SMDL #12-002 available at http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD-12-002.pdf.
See http://www.hennepin.us/files/HennepinUS/HSPHD/Department/Hennepin%20Heal....
From Hennepin Health proposal submitted to the state; available at http://www.hennepin.us/healthcare.
Hennepin Health leaders recognized that this pattern of pharmacy use was likely a sign that some members were addicted to or misusing prescription drugs, while some members were receiving multiple prescriptions from different health care providers, including providers of mental health services and specialists who were treating multiple medical conditions without adequate coordination.
The Department of Healthcare and Family Services (HFS) oversees the Illinois Medicaid program. Solicitation for Care Coordination Entities and Managed Care Community Networks for Seniors and Adults with Disabilities, Innovations Project, 2013-24-002, http://www2.illinois.gov/hfs/PublicInvolvement/cc/Documents/Innovations%20Solicitation.pdf.
For more information see http://www.hiltonfoundation.org/18-million-fund-to-provide-housing-for-high-need-homeless-patients-in-los-angeles-county.
Beginning with a pilot in the Skid Row area and expanding to other areas in Los Angeles County during late 2013 and 2014, the Coordinated Entry System is using an assessment instrument called the Vulnerability Index and Service Prioritization Decision Assistance Tool (VI-SPDAT) that has been developed by Community Solutions and the 100,000 Homes Campaign. For more information see http://www.unitedwayla.org/home-for-good/about/ces/.
The Corporation for Supportive Housing in Los Angeles is leading the Frequent Users System Engagement (FUSE) Program, which facilitates partnerships among hospitals and providers of housing assistance, health care and other services and supports to engage and house people experiencing chronic homelessness who are among the most costly users of public services. For more information see http://www.csh.org/csh-solutions/serving-vulnerable-populations/health-systems-users/local-complex-health-needs-work/los-angeles-fuse/.
28 C.F.R. pt 35 app. A (2010).
U.S. v. Georgia. 10-CV-249. (N.D. GA 2010), http://www.ada.gov/olmstead/olmstead_cases_list2.htm.
In 2011, DOJ released a statement with a series of questions and answers on the ADA's integration mandate and Olmstead enforcement. See http://www.ada.gov/olmstead/q&a_olmstead.htm.
HUD's Supportive Housing Program Desk Guide identifies the PSH component of the program as "Supportive Housing for Persons with Disabilities" and defines it as, "the SHP component that provides long-term, community-based housing and supportive services for homeless persons with disabilities." https://www.onecpd.info/resources/documents/SHPDeskguide.pdf, p. 8.
Statement of the Department of Housing and Urban Development on the Role of Housing in Accomplishing the Goals of Olmstead. http://portal.hud.gov/hudportal/documents/huddoc?id=OlmsteadGuidnc060413.pdf.
See http://medicaid.gov/Federal-Policy-Guidance/Downloads/CIB-06-18-12.pdf. This informational bulletin contains links to additional HUD and HHS guidance and resources to support Olmstead implementation.
More information is available in a brief prepared by the Technical Assistance Collaborative, Taking Integrated Permanent Supportive Housing (PSH) to Scale: The Louisiana PSH Program, February 2012, available at http://www.tacinc.org/media/10896/Louisiana%20Brief.pdf.
In the District of Columbia, a lawsuit related to the need for community alternatives to St. Elizabeth's Hospital was filed before passage of the Americans with Disabilities Act or the Supreme Court's Olmstead decision. Beginning in 2000, changes were made to the District of Columbia Medicaid state plan to add optional benefits that have been used to create a system of services and supports linked to housing in the community for people coming from institutional settings as well as people experiencing homelessness.
A link to the Final Rule as well as links to several fact sheets and summaries prepared by CMS are available at http://medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Long-Term-Services-and-Support/Home-and-Community-Based-Services/Home-and-Community-Based-Services.html.
HUD requires persons receiving rent subsidies through its Shelter + Care program to see a case manager at least once a month.
See Section 223 [42 U.S.C. 423] (d)(2)(C).
For more information about some of these issues and opportunities, see the Integrated Care Resource Center at http://www.integratedcareresourcecenter.com.
More information about California's Coordinated Care Initiative is available at http://www.calduals.org.
For more information about Medicaid's Health Home benefit see http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Long....
The National Alliance to End Homelessness describes some of these opportunities in the 2012 brief Medicaid Health Homes: Emerging Models and Implications for Solutions to Chronic Homelessness, available at http://b.3cdn.net/naeh/7a2ef4b455106166c7_trm6i2xg7.pdf.
More information about this initiative is available at http://www.health.state.mn.us/healthreform/homes/ and in the Annual Report on Implementation available at http://www.health.state.mn.us/healthreform/homes/legreport/2011HCHLegReport.pdf.
State law also requires all private health plans to reimburse certified health care homes using an approach that is consistent with the state's approach to paying for public programs.
At the end of the study period, in response to questions from CMS, the State of Minnesota decided to withdraw some components of this Medicaid waiver proposal.