
ADVISORY COUNCIL ON ALZHEIMER'S RESEARCH, CARE, AND SERVICES
Monday, January 14, 2013
- NAPA Research Progress Report
- Clinical Care Progress Report
- Long-Term Services and Supports Progress Report
- VA Dementia Initiatives
- 2013 Recommendations Presentations
NAPA Research Progress Report
Richard J. Hodes, M.D.
Chair, Research Subcommittee
Goal 1: Prevent and Effectively Treat Alzheimer's Disease by 2025
- Strategy 1.A: Identify Research Priorities and Milestones
- Strategy 1.B: Expand Research Aimed at Preventing and Treating Alzheimer’s
- Strategy 1.C: Accelerate Efforts to Identify Early and Presymptomatic Stages of Alzheimer’s Disease
- Strategy 1.D: Coordinate Research with International Public and Private Entities
- Strategy 1.E: Facilitate Translation of Findings into Medical Practice and Public Health Programs
Goal 1: Prevent and Effectively Treat Alzheimer's Disease by 2025
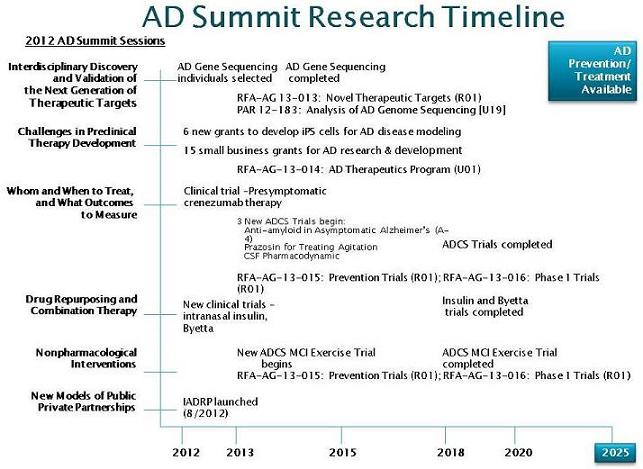
Strategy 1.A: Identify Research Priorities and Milestones
Alzheimer's Disease Research Summit 2012: Path to Treatment and Prevention
May 14-15, 2012
National Institutes of Health
U.S. Department of Health & Human Services
Bethesda, MD
AD Summit Research Timeline
 |
Strategy 1.A.4: Convene a scientific workshop on other dementias in 2013
- Alzheimer’s Disease-Related Dementias: Research Challenges and Opportunities, Natcher Auditorium, NIH Campus, Bethesda, MD May 1-2, 2013
- The workshop will define the state of the science and identify the critical opportunities and barriers in each of the dementias, whether basic, translational, or clinical.
- Open to the public. Register online.
Down Syndrome Research Update
- The Global Down Syndrome Foundation, Alzheimer’s Association and the Linda Crnic Institute for Down Syndrome hosted the workshop from September 13- 14 to bring together key scientists from the fields of Down syndrome and Alzheimer’s research in Chicago. Attendees included NIA and NICHD staff.
- NIA and NICHD have begun planning for a research workshop on Down Syndrome and Alzheimer’s disease in 2013.
1.B.2 Expand genetic epidemiologic research to identify risk and protective factors for Alzheimer's disease.
- Conduct whole genome sequencing to identify areas of genetic variation that correspond to risk factors of AD.
Alzheimer's Research Highlights -- Gene Discovery
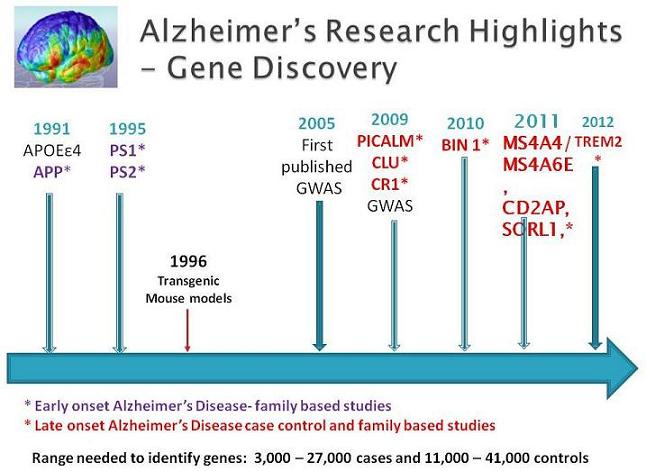 |
1.B.2. Sequencing -- Update
- Extensive cataloging of individuals from national and international studies for whom Genome Wide Assay Wide Studies (GWAS) genotyping and phenotypic data exist, and who have given consent for further research studies.
- Panels of experts are now studying cases, controls, and families to determine the priorities for sequencing and determine the most informative study possible.
- Sequencing to begin early in 2013.
Strategy 1.B.3: Increase enrollment in clinical trials and other clinical research through community, national, and international outreach
- Organize meetings to identify approaches and coordination points for these efforts.
- Implement an action plan that incorporates ideas from meeting.
AD Clinical Trial Enrollment Update
- Request for Information (RFI) released November 2012 and disseminated broadly to interested organizations (ADCs, ADCS, health professional and aging research organizations, CTSAs, RCMARs, key Federal agencies (VA, FDA), NIH Institutes and clinical research awareness working group) – responses due March 15, 2013
- Discussions underway with Federal agencies, grantees, and private organizations to assess efforts, effective strategies, registries
- Coordinating with NINDS/NIH regarding related upcoming events
- Developing workshop for Spring/Summer 2013
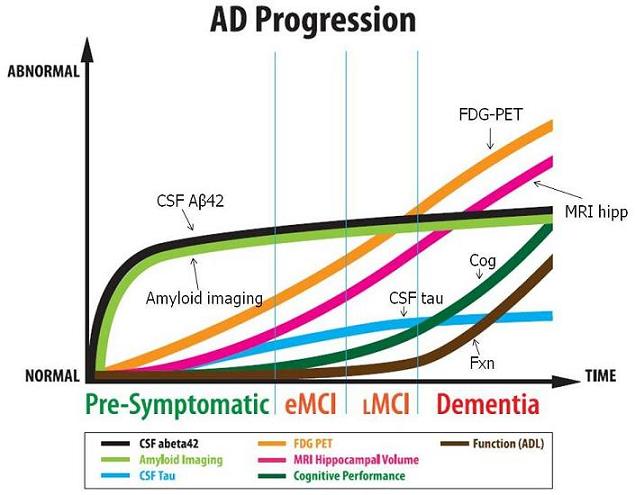
Strategy 1.C: Accelerate Efforts to Identify Early and Presymptomatic Stages of Alzheimer's Disease
- Identifying imaging and other biomarkers in presymptomatic people will facilitate earlier diagnoses in clinical settings, as well as aid in the development of more efficient interventions to slow or delay progression.
Alzheimer's Disease Neuroimaging Initiative (ADNI)
- Continues to collect data and samples to establish a brain imaging, fluid biomarker, and clinical database in order to identify the best markers or combinations of markers for following disease progression in the brain.
- Goal: Ability to utilize this information in clinical trials to monitor response to interventions focused on altering disease progression.
AD Progression
 |
Goal 1: Prevent and Effectively Treat Alzheimer's Disease by 2025
- Strategy 1.D: Coordinate Research with International, Public and Private Entities
Common Alzheimer's Disease Research Ontology (CADRO) Structure
- The CADRO is a three-tier classification system created to capture the complete range of AD research and AD research-related resources.
- The first level of classification consists of seven categories: five research and two research resources-related:
- Category A – Molecular Pathogenesis and Physiology of Alzheimer’s Disease
- Category B – Diagnosis, Assessment and Disease Monitoring
- Category C – Translational Research and Clinical Interventions
- Category D – Epidemiology
- Category E – Care, Support and Health Economics of Alzheimer’s Disease
- Category F – Resources for the research community
- Category G – Consortia and Public Private Partnerships
- Each category is divided into “research topics”; many of the topics are further divided into “research themes”.
- This detailed classification will enable funders to identify research gaps, areas of overlap/duplication of effort and opportunities for collaboration with much greater specificity.
National Institute on Aging/National Institutes of Health -- Alzheimer's Association Collaboration
Common Alzheimer’s Disease Research Ontology (CADRO)and International Alzheimer’s Disease Research Portfolio (IADRP)
- The CADRO and IADRP were developed by the National Institute on Aging at the NIH in collaboration with the Alzheimer’s Association.
- The IADRP database will enable funders of Alzheimer’s research to coordinate planning, leverage resources, avoid duplication, and identify new opportunities for collaboration.
- The database will give the public a full picture of the scale of ongoing research on AD.
- To date, the IADRP database includes funded research from all US federal agencies and Alzheimer’s Association. Funded grants from the Alzheimer’s Drug Discovery Foundation and Alzheimer’s Research UK have been coded and are in the process of being uploaded. Active efforts are underway to include more domestic and international funders.
- More information about CADRO and IADRP.
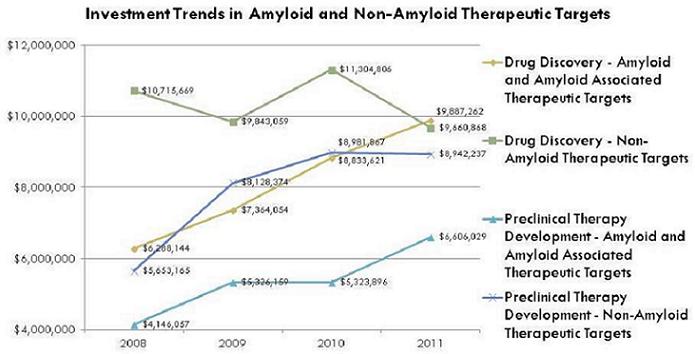
Common Alzheimer’s Disease Research Ontology (CADRO)and International Alzheimer’s Disease Research Portfolio (IADRP)
EXAMPLE: Comparative Investment Across Research Categories
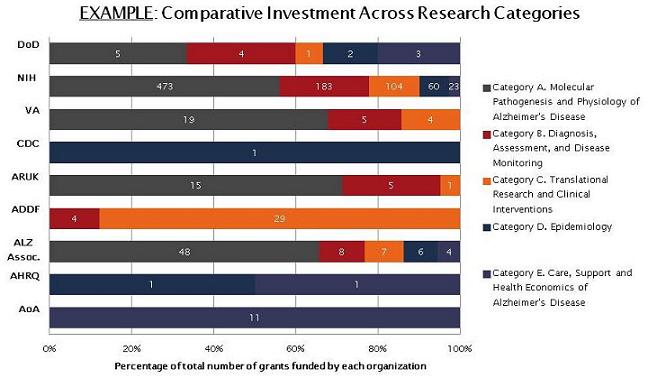 |
Category C. Translational Research and Clinical Interventions
 |
Ongoing AD and Dementia Public Private Partnerships
- Alzheimer’s Disease Neuroimaging Initiative (ADNI 2) -- over 27 federal and private partners (FNIH raised $23 million for ADNI1)
- International Alzheimer’s Disease Research Portfolio (IADRP) and Common Alzheimer’s Disease Research Ontology (CADRO)-- Alzheimer’s Association and NIH/NIA
- AD International Funders-- Alzheimer’s Association and NIH/NIA
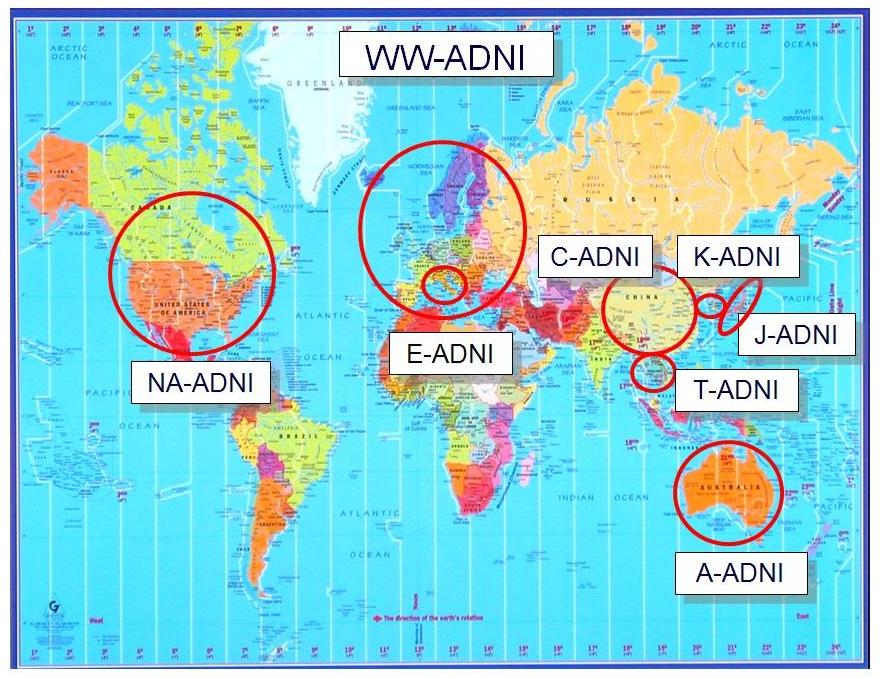
ADNI Public-Private Partnership Structure
|
WW-ADNI
 |
AD Public Private Partnership (PPP) Development Activities
Alzheimer's Disease Measurement Improvement (AD-MI)
- Alzheimer's Disease Measurement Improvement Conference held in Baltimore, MD on December 3, 2012
- More activities in planning
- Collaborators include:
- Agency for Health Care Quality (AHRQ)
- Alzheimer’s Foundation of America
- Alzheimer’s Association
- American Medical Association Physician Consortium for Performance Improvement (AMA-PCPI)
- Leaders Engaged in Alzheimer’s Disease (LEAD)
- Centers for Medicare and Medicaid Services (CMS)
- Food and Drug Administration (FDA), Foundation for NIH, Institute of Medicine (IOM)
- National Alliance for Caregiving
- National Institutes of Health /(National Institute on Aging (NIA)
- National Quality Forum (NQF), National Pharmaceutical Council and representatives from the pharmaceutical industry
- NIA will host Public Private Partnership meeting in April 2013 – academia, NIH, Pharma, potential development of a partnership to share preclinical data, drug targets, and animal models in a precompetitive space to facilitate new therapies for AD.
- Contact: Dr. Suzana Petanceska (petanceskas@mail.nih.gov)
Strategy 1.E: Facilitate Translation of Findings into Medical Practice and Public Health Programs
- Promising research and interventions are published in the research literature and provided in annual report to Congress and public.
National Institutes of Health Annual Report to Congress on Alzheimer’s Disease Research
2011-2012 Alzheimer's Disease Progress Report: Intensifying the Research Effort
Clinical Care Progress Report
Shari M. Ling M.D.
Deputy Chief Medical Officer
Centers for Medicare & Medicaid Services (CMS)
Center for Clinical Standards & Quality (CCSQ)
Outline
- Overview
- Medicare Coverage
- Measure Improvement
- Training (HRSA)
- Care Models (CMMI)
- Patient and Family Engagement Campaign (CCSQ)
- Community Care Transitions Program
- National Partnership to Improve Dementia Care in Nursing Homes
Implementation Milestones
- June 2012
- Identify and disseminate appropriate assessment tools
- Implement and evaluate new care models to support effective care transitions for people with AD
- July 2012
- Strengthen the direct-care workforce
- Collect and disseminate dementia-specific guidelines and curricula for all provider groups across the care spectrum
- Explore programmatically relevant dementia care guidelines and measures
- December 2012
- Identify and disseminate appropriate assessment tools
- Explore programmatically relevant, dementia care guidelines and measures
- Monitor, report, and reduce inappropriate use of anti-psychotics in nursing homes
- February 2013
- Patient and Family Engagement Campaign (PFEC) (12-18 months)
- September 2014
- Implement and evaluate new care models to support effective care transitions for people with AD
- July 2015
- Evaluate the effectiveness of medical home models for people with AD
- Evaluate the effectiveness of the Independence at Home Demonstration
- Explore the effects of new payment models on AD care and costs.
- Consider test of new payment or delivery model to promote the quality of AD care while reducing costs
Centers for Medicare & Medicaid Services Screen Shot
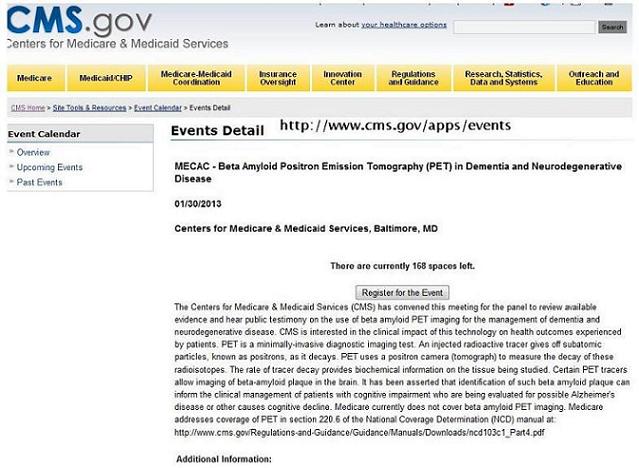 |
The Original (Ongoing) Dilemma
- Intense public interest in coverage of certain (usually new) technologies
- Published evidence base was often
- Suggestive but insufficient to reach a positive R&N decision
- Too immature for confident decision
- In general, clinical trials under-enroll subjects representative of the beneficiary population
- In general, clinical trials do not focus on clinical utility outcomes of interest to CMS
The Preferred Road to Coverage
Provide adequate evidence that...
- Diagnostics
- The incremental information obtained by new diagnostic technology compared to alternatives
- Changes physician recommendations
- Resulting in changes in therapy
- That improve clinically meaningful health outcomes
- Therapeutics
- A treatment strategy using the new therapeutic technology compared to alternatives
- Leads to improved clinically meaningful health outcomes
In Medicare beneficiaries
Screen Shot
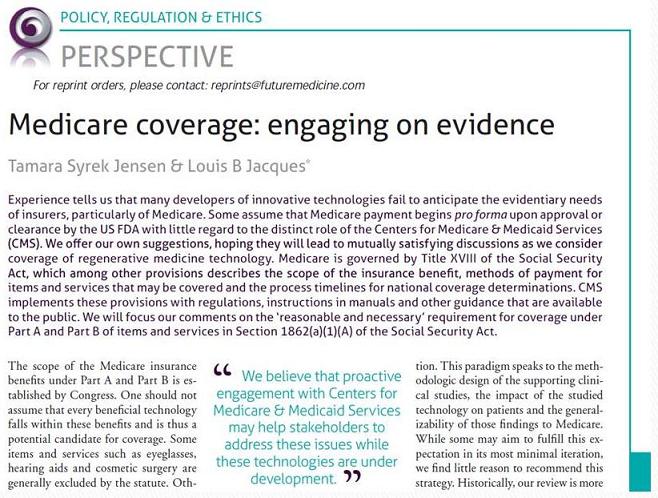 |
Abstract
Expanding the Coverage with Evidence Development Program to Drive Innovation: Reimbursement for medical treatments is a powerful driver of industry investment. Under the Coverage with Evidence Development (CED) program, Medicare reimburses for promising new technologies that do not currently meet the standard for full coverage. The CED program requires more evidence to be collected to determine full potential benefit of new technologies. The CED authority has existed for more than a decade but has been applied sparingly. The Centers for Medicare & Medicaid Services (CMS) is poised to implement the next phase of CED by better defining the parameters and guidance for CED so it can be used more widely and effectively as a driver of innovation. CMS believes that the lessons learned during the initial implementation of CED can inform its more frequent use and create predictable incentives for innovation while providing greater assurance that new technologies in fact fulfill their initial claims of benefit.
Alzheimer's Disease Measurement Improvement (AD-MI): Project Overview
- FNIH convened meeting, Aligning Outcome Measures for Alzheimer's Disease in May 2011
- Formed the Alzheimer’s Disease Measurement Improvement (AD-MI) Working Group
- AD-MI Working Group Goal: establish a “mega-community” around improving quality of care and outcomes by improving measurement in Alzheimer’s disease (AD)
- Four workgroups
- Draft a conceptual framework and translate the conceptual work into actions
- Develop a landscape inventory of relevant measures, guidelines, stakeholders
- Set a research agenda with recommendations from workgroups 1 & 2
- Oversee publication effort and summarize work of AD-MI Working Group in the 2012 meeting
- 2013 Plans
- Spring summary publication and continue to grow the “mega community”
- Develop schema of optimal care
- Address heterogeneity of patient population (diagnosis stage)
- Explore cross-cutting themes from other chronic conditions
- Working Group 1 established a conceptual framework recommending that the group:
- Prioritize AD/dementia and identify optimal systems of care
- Promote quality of care measures that rely on determining disease stage and components of disease recognition, diagnosis, care management and treatment
- Identify quality-measurement opportunities to guide the categorization and prioritization of quality indicators
- Articulate measurement development needs, including early detection and diagnosis, appropriate use of therapeutics, care management of co-morbidities and complications
- Working Group 2 conducted an environmental scan, identified existing measures and guidelines, and discovered:
- Existing measures focus on the time after diagnosis and few measures relate to detection/screening
- Existing measures are process focused, rather than outcome or structural measures
- No measures exist for accurate diagnosis or timeliness of diagnosis
- Medicare’s Annual Wellness Visit includes detection of cognitive impairment, but no specific tools, process, or reports are required for evaluation
- Working Group 3 synthesized the AD-MI work and identified gaps and future research needs:
- Care improvement will require new understanding of the epidemiology of AD
- Better diagnostics are required, driven by quality measures of care
- Better measures of disease staging will improve care
- Strategic research focus going forward should include PCP-based screening assessments and improved diagnostic algorithms
- Working Group 4 will produce a meeting summary and improve the visibility of AD-MI work through a website, partnerships with other organizations, and publications in relevant journals
Supplemental Dementia Training
- 45 Geriatric Education Centers received 2 years of supplemental funding
- $42,222 in FY12; Up to $92,684 in FY13 (depending on availability of funds)
- Educate healthcare providers to
- Work with people with AD and their families
- Link people to support services
- Identify signs of caregiver burden and depression
- Detect cognitive impairment and assess/diagnose AD
GEC Dementia Trainings
- Between 7/1/12 and 12/31/12 the 45 GECs had:
- 178 interprofessional continuing education programs
- 10,976 trainees
- Each event trained between 2 and 25 professions
- 248 community partners include
- 28 Quality Improvement Organizations
- 15 Alzheimer’s Association chapters
- 8 Area Health Education Centers
- 8 Veterans Administration hospitals
- IHS, AHRQ, AGS, AMDA, AAA
GEC Dementia Training Topics
- AD Guidelines
- Signs & Symptoms
- Assessment
- Caregiver Issues
- Managing AD with co-morbidities
- Referrals
- Understanding and accessing LTSS
- Providers training patients
- Cultural sensitivity
- HIPAA training Transitions of care Clinical trials
Innovation Center
- Awards made May - June, 2012
- Data reporting quarterly
- Metrics programmatic processes, service delivery and outcomes TBD depending on drivers & goals
- Independent evaluation RFPs or other publically advertised mechanisms
- Anticipated completion date 2015-16
- Data sharing mechanisms TBD
CMMI: Health Care Innovation Award Project (Dementia/Alzheimer's Relevant)
- Indiana University “Dissemination of the aging brain care program”
- UCLA “UCLA Alzheimer’s and dementia care: comprehensive, coordinated, patient-centered”
- University of North Texas Health Science Center “ Brookdale Senior Living Transitions of Care Program”
- University of Rhode Island “Living Rite--A Disruptive Solutions for Management of Chronic Care Disease”
Trustees of Indiana University
- Project Title: “Dissemination of the aging brain care program”
- Plan: to improve care for Medicare beneficiaries with dementia or late-life depression within a safety net health system in Marion County, IN.
- Will provide individualized and integrated care through a multidisciplinary care team; will develop patient-specific care plans, deliver evidence-based protocols, and respond to real-time monitoring and feedback
Regents of the University of California, Los Angeles
- Project Title: “UCLA Alzheimer’s and dementia care: comprehensive, coordinated, patient-centered”
- Plan: To provide coordinated, comprehensive, patient and family-centered, and efficient care for approximately 1000 Medicare and Medicaid beneficiaries with Alzheimer’s disease or other forms of dementia
University of North Texas Health Science Center
- Project Title: “Brookdale Senior Living (BSL) Transitions of Care Program”
- Goal: Prevent the progress of disease, thereby reducing complications, improving care, and reducing the rate of avoidable hospital admissions for older adults
University of Rhode Island
- Project Title: “Living Rite-A Disruptive Solution for Management of Chronic Care Disease (a focus on adults with disabilities: intellectual and developmental diagnoses and dementia patients with 2 or more chronic conditions)”
- Use Interdisciplinary care management teams to teach patients
- how to best manage their chronic diseases
- Provide comprehensive and preventive care for intellectually and developmental challenged dual eligible beneficiaries
Quality Improvement
- Quality Improvement Organizations
- 10th SOW
- 18th Month products
- Intervention effectiveness tools that outlines communities with their target populations, interventions and preliminary outcomes based on 4+ months of data
- Anticipate 200+ submissions. This will provide a good gauge for identifying communities that may be targeting individuals with dementia, what the interventions are, and can certainly follow up regarding assessment and other evaluation tools currently being used.
QIO special project in the 10th SOW -- Patient and Family Engagement Campaign (PFEC)
- Funding to Quality Improvement Organizations (QIOs) who propose fresh and original models to develop and implement local campaigns to improve person-centeredness and family engagement .
- This effort will encourage involvement of patients and families in decisions regarding health and health care to ensure consistency with patient preferences and priorities, and to empower them to take action for their own health care that could improve quality of life.
Focus & Aims
- Focus: The QIO shall design its PFEC work to target behaviors among beneficiaries that will address at least one topic below:
- Care for Individuals Diagnosed with Dementia
- Prevention of Avoidable Readmissions;
- Prevention of Falls;
- Improvement of Cardiac Health
- Aims:
- Improve quality of life for Medicare beneficiaries through patient-focused care;
- Improve beneficiary awareness of preventive care initiatives;
- Improve caregivers’ knowledge of available resources;
- Improve patients and families full participation in their own care and health, and encourage them to partner, according to their preference, with clinicians in fulfilling those expectations.
Centers for Medicare & Medicaid Services Screen Shot
 |
The Community-based Care Transitions Program (CCTP)
- The CCTP, mandated by section 3026 of the Affordable Care Act, provides funding to test models for improving care transitions for high risk Medicare beneficiaries.
- CMS is currently accepting applications on a rolling basis and will continue to award applications on a rolling basis as funding permits (50 programs and counting)
Community-Based Care Transitions Program: It's NOT a Grant -- It's Something Better!
- Community-based organizations partnering with hospitals and other providers, define and price a new cost-effective care transitions service for Medicare patients in their communities -- tailored to their own unique circumstances and capabilities!
- Conduct a thorough Root Cause Analysis and tailor intervention strategy to directly target your community’s readmissions drivers
- Payment (per eligible discharge rate, no more than 1x / 180 days) is for direct service costs, not training, overhead, other indirect costs.
- Tell us how services don’t duplicate those already required through the discharge planning process / CMS Conditions of Participation.
National Partnership to Improve Dementia Care in Nursing Homes: Project Overview
- Technical Expert Panel convened in April 2012
- Content guided the development of surveyor guidance and work of state coalitions that followed
- Outreach calls to 50 states
- Coalitions established or strengthened in all 50 states
- Work with CMS regional offices and state agencies to begin surveyor training
- New guidance development near completion
- Two new mandatory surveyor training videos completed and ready for launch in January 2013
- Individual outreach calls by CMS core team to various public and private partners
- Ombudsman, associations, behavioral health, dementia specialists, psychiatry
- Actively engaged these groups in the national work and state coalitions
- Major presentations to national, state and local groups around the country
- Provider education
- Completion of research
- 200 case studies from 25 nursing home in five states
- Focused on how decisions to use or not to use antipsychotic medications were made
Long-Term Services and Supports Progress Report
Jane Tilly, Dr.PH
Office of Supportive and Caregiver Services
Administration on Aging/Administration for Community Living
Progress
| Action # | Action Description | Method of Action | Lead Agency (Partner Agencies) | Status |
|---|---|---|---|---|
| 3.B.6 | Share lessons learned through VA caregiver support strategies with federal partners | Scheduled informational meetings | VA (Federal partners) | VA lead an interagency call that focused on presentation and discussion of the REACH-VA caregiver support program. |
| 2.A.3 | Collect and disseminate dementia-specific guidelines and curricula for all provider groups across the care spectrum | Develop dementia-specific guidelines and curricula | HRSA (VA, CMS, NIH, IHS) | HRSA worked with 45 Geriatric Education Center grantees who trained provider groups across the care spectrum. Grantees have delivered 178 programs to 10,976 providers on dementia related topics in the past 6 months. |
| Develop website with appropriate links and contact info | HRSA (VA, CMS, NIH, IHS) | HRSA identified and vetted appropriate links, but the website is not in place. | ||
| 2.A.5 | Stengthen the state aging and public health workforces | Report on progress annually | AoA, CDC | CDC is developing a new Healthy Brain Initiative Road Map for public health. Completed concept mapping process. |
| AoA/ACL conducted a webinar series on legal issues for those with dementia and their caregivers. | ||||
| AoA/ACL developed a new LTSS workforce competency model addresses cognition. | ||||
| AoA/ACL provided training materials to the National Council of Certified Dementia Practitioners | ||||
| 2.C.2 | Enhance assistance for people with AD and their caregivers to prepare for care needs | AoA will develop training materials for Options Counseling which includes best practices for working with persons with cognitive impairments and their caregivers. | AoA | AoA/ACL options counseling standards now include dementia-capability as a core competency. |
| Update tools and resources to educate caregivers about available programs and resources | AoA (CDC) | Options counseling standards include dementia-capability core competency that will be part of a new options counseling training and certification program. Tools and resources for caregivers on Alzheimers.gov have been updated. AoA/ACL presented webinar on advance health and financial planning that addresses caregiver issues. | ||
| 2.D.1 | Explore programmatically relevant, dementia care guidelines and measures | Identify 3-5 measures within the first year; submit measures and programmatically relevant guidelines to National Quality Forum | CMS (AHRQ, VA, ASPE, AoA/ACL) | CMS developed quality measures as part of the National Partnership to Improve Dementia Care in Nursing Homes for potential use in Nursing Home Compare. |
| 2.G.1 | Review evidence on care coordination models for people with AD | Meeting Summary Report | ASPE | ASPE found little rigorous evidence available to use in defining effective care coordination models for persons with dementia. Further research is necessary to develop such models. |
| 3.B.1 | Identify unmet service needs | Release report summarizing analysis of National Health and Aging Trends Study data | ASPE | ASPE reviewed methods for defining Alzheimer's/ dementia that are possible for the National Health Aging Trends Study and found major definitional issues that must be resolved before analyses can begin. |
| 3.B.2 | Identify and disseminate best practices for caregiver assessment and referral through the long-term services and supports system | Explore public-private partnership to identify best practices in caregiver assessment / referral. Examine assessment tools used in states, incl. state Medicaid waiver programs | AoA/ACL (private partners) | In partnership with the National Family Caregiver Alliance, published Selected Caregiver Assessment Measures (2nd Edition): A Resource Inventory for Practitioners. This resource provides a compendium of caregiver assessment measures that is practice-oriented, practical and addresses aspects of the caregiving experience. |
| 3.C.2 | Expand long-term care awareness efforts | Implement awareness campaign | AoA | Expansion of Alzheimer’s awareness efforts into long-term care awareness depends upon availability of additional funds. |
VA Dementia Initiatives
Susan Cooley, Pauline Sieverding, Meg Kabat
This presentation is available.
2013 Recommendations Presentations
Research Subcommittee Recommendations
Research Subcomittee Recommendations
- Voting Members
- Jennifer Manly
- Harry Johns
- Ronald Petersen
- George Vradenburg
- Non-voting Members
- Richard Hodes
- Russell Katz
- Don Moulds
Themes of original research recommendations
- Commit resources with accountability
- Accelerate basic and translational research toward development of effective treatments
- Add concrete emphasis on process of development of interim milestones and importance of including these in the next version of the Plan
- Maximizing private investment to develop treatments and improve disease monitoring technology
- Meaningfully coordinate with global partners
Recommendation 1
We support and applaud the goal of the National Plan -- to prevent and effectively treat Alzheimer’s Disease by 2025, and recommend that interim milestones be explicitly stated, through development of a clear roadmap of research and treatment discovery priorities and timelines, to assure continuing and successful progress toward achievement of this goal
Notes on Recommendation 1
- The text of the next version of the National Plan should include the outcome of the process currently underway to specify and prioritize interim milestones. Data from the International Alzheimer's Disease Research Portfolio (IADRP), and recommendations from the May 2012 Alzheimer's Disease Research Summit, private public working groups, and other scientific meetings and collaborations are being prioritized to set immediate (2013 - 2015), mid-term (2016 - 2019), and longer term (2020 - 2025) milestones to achieve the goal.
- A model of a grid with interim milestones is attached. These milestones rely on and relate to the final recommendations from the May 2012 Alzheimer's Disease Research Summit and thus represent a focused subset of potential milestones for achieving the 2025 goal. This grid is intended to be a dynamic document that will be continuously improved and refined based on the process outlined above, including input from nationally and internationally- based public and private sources. New investment in research must reflect a critical balance between basic research and the urgency of treatment discovery.
Recommendation 2
There is an urgent need for annual federal research funding to be increased to the level needed to fund a strategic research plan and to achieve the breakthroughs required to meet the 2025 goal. Initial estimates of that level are $2 billion per year but may be more. That investment would be applied to Alzheimer’s research initiatives spanning basic, translational and clinical research.
Notes on Recommendation 2
- There has been significant commitment by the Obama Administration in 2012 ($50 million) and promise of $80 million in new Alzheimer’s disease research funding in fiscal year 2013
- This commitment could represent the initial stages of a ramp-up but the urgency of getting to $2 billion or more per year is unchanged
Recommendation 3
- We recommend that HHS continue to develop, execute and regularly update a strategic research plan and priorities to accelerate breakthroughs in AD research.
Notes on Recommendation 3
- Very productive meetings have occurred, and NIA FOAs have been released as a result of the recommendations
- A comprehensive strategy of applying these recommendations across public and private funding sources has not been fully explicated
- The synchronization and coordination between the contents of the National Plan and a research plan is not yet explicit.
Recommendation 4
To address disparities, we recommend that clinical research studies and activities aimed at translation of research findings into medical practice and to the public include specific targets for outreach to specific populations by racial/ethnic group, sex, and socioeconomic status, as well as to populations at high risk for AD (e.g., people with Down Syndrome).
Notes on Recommendation 4
- Down syndrome and intellectual disability populations are not yet specifically mentioned within Goal 1 (but a 2013 Down Syndrome meeting is planned)
- The National Plan does not yet include language or strategies focused on leveraging existing resources and engaging private entities
- An emphasis on "translation of research findings" to diverse populations is not explicit in the Plan.
Recommendation 5
We recommend that HHS, in partnership with experts from the research community and industry, take steps to accelerate public access to new therapeutic interventions by compressing the current average time in the process of identification of therapeutic targets, validation of those targets, development of behavioral and pharmacologic interventions, testing of efficacy and safety, and regulatory review.
Notes on Recommendation 5
- Original recommendations 5,6,7 & 8 have been consolidated into one emphasizing acceleration of discovery and public access to treatments, with several potential arms and detailed suggestions
- Many details included in this recommendation are relevant to the implementation plan but are not yet included. This may be at least somewhat addressed by the interim milestone process described in Recommendation 1.
- The role of PPPs in enhancing scientific innovation and discovery, or progress in shortening the regulatory process is not yet uniquely emphasized in the plan
Recommendation 6
- We recommend that the HHS Secretary develop a continuing process by which research priorities aimed at accelerating the delivery of effective treatments would be set, including input from scientific experts.
- There are now existing models of joint academic and Industry Working Groups, which can serve as opportunities to create true partnerships between government and industry to inform research priorities.
- In order to accelerate the process of discovery, we recommend that Working Groups identify strategies for increasing the increased standardization, disclosure, pooling and analysis of pre-clinical, clinical and electronic health data.
Notes on Recommendation 6
- The next version of the National Plan should include a description of an overarching process by which both public and private resources will be coordinated in setting research priorities.
- Multiple ongoing PPP initiatives are already moving forward on this recommendation and thus specifics could be integrated in future versions of the plan
Recommendation 7
We recommend that HHS develop accurate and relevant metrics for assessing the impact of Alzheimer’s on the U.S. economy.
Notes on Recommendation 7
- There is general overlap between this recommendation and Goal 5, which discusses metrics
- However measurement of economic impact of AD, or the rationale for doing so, is not specifically discussed in Goal 5 or elsewhere in the Plan
Recommendation 8
We recommend that HHS commit to an effort to maximize private investment in the development of treatments and improvements in disease monitoring technology by identifying policies that would encourage private industry to invest aggressively in disease-modifying interventions, to support technologies that improve our ability to detect the disease as early as possible, and monitor the disease accurately so that the effectiveness of interventions can be tested.
Notes on Recommendation 8
- This revised item has consolidated several recommendations related to PPPs that were previously spread out across other items
- There is meaningful implementation detail within this recommendation that is not yet carried though to the Plan
Recommendation 9
We recommend that the Administration continue to expand and enhance meaningful coordination with global partners and move forward to establish a Global Alzheimer's Action Plan to respond to the global scope of the problem.
Notes on Recommendation 9
- Promising progress has been made: global partners participated in the May 2012 meeting, met with HHS at the Vancouver AAIC, and a number of bilateral efforts have begun
- However the current National Plan does not explicitly discuss a Global AD Plan, a single high level official whose responsibility it is to foster international cooperation has not been identified, and thus far there has been no coordinated discussion internationally of regulatory hurdles.
Recommendation 10
We recommend that the Administration designate specific Offices and officials within the White House and the Office of the Secretary of HHS with responsibility and accountability for effective implementation of, and timely, transparent reporting on, all aspects of the implementation of this National Alzheimer’s Plan, including responsibility for issuing statutorily required reports to Congress on behalf of the Secretary, reports to the Advisory Council, and other reports as warranted.
Notes on Recommendation 10
- Although the current implementation strategy designates specific offices responsible for Action Items in the Plan, unaddressed aspects of this item include detail about metrics, milestones, implementation steps, and accountability.
- No separate, central NAPA office in the White House & HHS is addressed in the current National Plan.
Discussion
Clinical Care Subcommittee Recommendations
Recommendation 1
Launch a nationwide public awareness campaign to promote early detection and diagnosis of Alzheimer’s disease.
Recommendation 2
Gather data on the detection of possible cognitive impairment as part of the Medicare Annual Wellness Visit.
Recommendation 3
Clarify the privacy protections under the Health Insurance Portability and Accountability Act (HIPAA) to ensure that health care providers can engage in care planning with family members of those diagnosed with Alzheimer’s disease or other dementias.
Recommendation 4
Develop a unified curriculum for primary care practitioners to become more knowledgeable about Alzheimer’s disease and enhance the skills necessary to deliver dementia capable care.
Recommendation 5
Evaluate models and demonstrations of payment and care delivery reform on the quality and cost for the subpopulation of participants with Alzheimer’s disease.
Recommendation 6
Form a blue ribbon panel of experts on advanced dementia to develop innovations in clinical care practice and quality, including palliative care, for people with advanced dementia.
Recommendation 7
Expand funding and incentives to encourage individuals to pursue careers in geriatric specialties.
Discussion
Long-Term Services and Supports Subcommittee Recommendations
Overview
- Many recommendations same as 2012; Updated and expanded where appropriate
- Recommendation 1 is primary recommendation from which many others flow
Recommendation 1
States should assure that they have robust, dementia capable LTSS systems.
Recommendation 2
HHS should provide federal funds to support a state lead entity in every state and territory. This entity will facilitate development of the state’s dementia capable systems, coordinate available public and private LTSS, conduct service gap analysis, identify opportunities for efficiency, and enable ongoing stakeholder input to address needs across all sectors and systems. HHS should use available funds to begin this process in 2013.
Recommendation 3
- HHS should engage all relevant federal agencies to include research on LTSS that addresses dementia capability in their research agendas. Topics needing further research include:
- Interventions for persons in the early stages of dementia, including those that mitigate symptoms of the disease.
- Interventions for persons with Down syndrome and other intellectual disabilities that are at high risk of acquiring dementia as they age.
- Impact of caregiving on health and quality of life of caregivers.
- Translation of interventions for persons with dementia and their caregivers into culturally appropriate programs.
- Translation of interventions for persons with dementia and their caregivers into community settings.
Recommendation 4
State education and health agencies and others should include key information about AD in all curricula for any profession or career track affecting LTSS.
Recommendation 5
State, local and private sector organizations should ensure that paraprofessional caregivers in every venue are adequately trained and compensated.
Recommendation 6
Congress and CMS should redesign Medicare coverage and physicians’ and other health care providers’ reimbursement to encourage appropriate diagnosis of AD and to provide care planning to diagnosed individuals and their caregivers.
Recommendation 7
LTSS systems should refer people to a healthcare provider for diagnosis whenever they are admitted to or assessed for eligibility for LTSS and exhibit signs of cognitive impairment.
Recommendation 8
Providers engaged in diagnosis should consider the National Institute on Aging’s 2011 guidelines for diagnosis of Alzheimer’s disease and rule out and treat any conditions that may mimic this disease.
Recommendation 9
The process of diagnosis should include engaging individual and family in advance care planning (health, legal, estate, and financial).
Recommendation 10
HHS should assure that health and related systems funded with federal resources should improve chronic disease treatment and related services for people with AD.
Recommendation 11
HHS should develop quality measures and indicators for the comprehensive care and treatment of individuals with AD.
Recommendation 12
Practice recommendations for care in every setting should be embedded in CMS’ federal and state surveillance and quality improvement systems.
Recommendation 13
Recommendations for end-of-life or palliative care should be incorporated into all CMS surveillance and quality improvement systems at the earliest possible time.
Recommendation 14
HHS should provide grants through CMS’ Center for Medicare and Medicaid Innovation (CMMI) for medical home pilot projects specifically targeted at improving medical and chronic condition management for individuals with AD, and coordination with family and community care providers in the full array of settings.
Recommendation 15
HHS should convene a blue ribbon panel of experts to recommend one or more models of palliative care for people with advanced dementia, including eligibility criteria and financing mechanisms, and provide grants through CMMI to implement and evaluate the models.
Recommendation 16
HHS should create a specific grant round of pilot projects through CMMI to implement and evaluate ways to reduce preventable emergency department visits, hospitalizations, and length of hospital stays for individuals with AD, who are living in the full array of settings.
Recommendation 17
HHS and state lead entities should partner to assure access to the full array of LTSS for specific populations of people with AD including younger people, non-traditional families, people with intellectual disabilities, such as Down syndrome, and racial and ethnic minorities who are at increased risk of acquiring AD.
Recommendation 18
- Recommended use of Federal Funds ($10.5 million) currently proposed for AoA
- HHS (AoA) should use the $10.5 million for state grants to seed the development of state action plans and state lead entities that maximize use of public and private resources to support dementia capable LTSS.
- Governors should designate the state lead entity and commit to sharing publicly a state plan with recommendations for action.
- State agencies and relevant partners should be included in the state action plan
- Legislation enacting this program should require matching funds so as to expand program impact.
- This program should be expanded in future years with additional resources.
- Additional funding available at HHS or other Operating Divisions in FFY 2013 and beyond should support this activity.
- Estimated funds necessary to fully fund all states’ action plans = $85 million.
Recommendation 19
Funding for the Alzheimer’s Disease Supportive Services Program (ADSSP) should be restored to the FFY 2003 level of $13.4 million.
Recommendation 20
Fully fund caregiver support under AoA
Recommendation 21
HHS, state lead entities, and providers should assure that caregiver physical health/ behavioral health risk is assessed and addressed regularly. Caregiver illness and mortality contribute to the enormous personal and financial cost of AD.
Recommendation 22
The Office of the National Coordinator for Health Information Technology, in partnership with the private sector, should work to assure that development of health information technology includes tools that assist caregivers of persons with AD. Tools could assist caregivers by: helping them organize the care they provide, educating them about dementia and multiple chronic conditions, and providing tools to help them maintain their own mental and physical health.
Recommendation 23
HHS should launch a nationwide public awareness campaign to increase awareness and to promote early detection of AD.
Discussion
Public Comments
Return to
National Alzheimer's Project Act Home Page
Advisory Council on Alzheimer's Research, Care, and Services Page
Advisory Council on Alzheimer's Research, Care, and Services Meetings Page