
Monday, November 9, 2020
Printer Friendly Version in PDF Format (22 PDF pages)
A Team-Based Intervention for Distress Behaviors in Dementia: Lessons Learned in VA Community Living Centers
Kim Curyto, PhD
Western NY VA Healthcare System, Center for Integrated Healthcare
Michele J. Karel, PhD, ABPP
National Mental Health Director, Geriatric Mental Health, Office of Mental Health and Suicide Prevention, VA Central Office
STAR-VA intervention and training program
- STAR-VA[1] is a person-centered, inter-disciplinary, behavioral approach to managing challenging behaviors among CLC[2] residents with dementia
- A CLC Mental Health (MH) Professional ("Behavioral Coordinator") and Registered Nurse ("Nurse Champion") work with entire team, including direct care staff
- Four core components
- Realistic expectations
- Effective communication
- ABC[3] problem-solving
- Pleasant events
- Training Program:
- Competitive site selection process
- Intensive virtual workshop, 6 months of consultation, competency based
-
- 2010: Pilot program
- 2013-2018: Annual training - 17-23 sites/year
- 95/134 CLCs trained at least once
- Retraining 2014-2018: 41 CLCs, 9 retrained 2X
- Adapted from Staff Training in Assisted Living Residences (STAR; Teri et al., 2005)
- Community Living Center
- Activator-Behavior-Consequence
STAR-VA TRAINING PROGRAM EVALUATION OUTCOMES
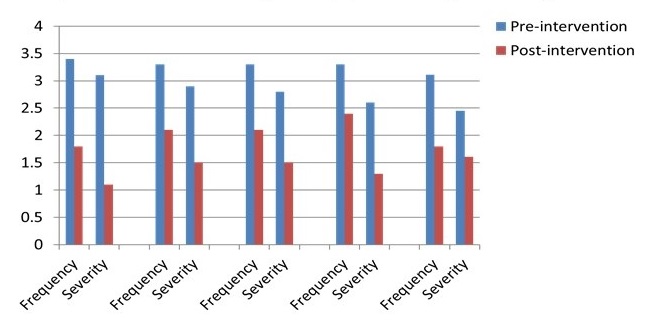
- Pre-post clinical outcomes for STAR-VA Veteran cases, 2013-17
- Significantly decreased frequency, severity of target behaviors
- Significantly decreased symptoms of depression, anxiety, agitation
- Increased self-reported confidence among trainees
 |
FURTHER EVALUATION NEEDED
- Positive training program outcomes; however...sustaining a new care approach is challenging
- E.g., staff turnover, teamwork challenges, resistance to new approaches, time, varying leadership priorities
- Many facilities requesting retraining -- not sustainable
- Facilitators and barriers to local program sustainment?
- Need for evaluation of program impact on key system outcomes
- Challenges given national roll-out, no controlled study
- STAR-VA evaluation grant
PARTNERED QUERI EVALUATION: team and acknowledgements
This study was funded by the U.S. Department of Veterans Affairs, Quality Enhancement Research Initiative (QUERI) PEC 16-35. Partnered QUERI evaluation: Offices of Mental Health and Suicide Prevention and Geriatrics and Extended Care
- Kim Curyto, PhD
- Kevin McConeghy, PharmD, MS
- Jennifer Sullivan, PhD
- Jenefer M. Jedele, PhD, MSc
- David Mohr, PhD
- Orna Intrator, PhD
- Laura O. Wray, PhD
- Jim Rudolph, MD
- Vince Mor, PhD
- Mark Kunik, MD
- Jennifer Mach, MD, MPH
- Linh Dang, MSc
- Omonyele L. Adjognon, ScM
- Jacqueline Pendergast, BS
- April Eaker, BA
- Kelly Vance, MD
- Ilse Wiechers, MD
- Michele J. Karel, PhD, ABPP
- Lisa Minor, RN, MSSL
Partnered queri evaluation: aimS
- Develop and validate
- Aim 1: Develop and validate a quality indicator for monitoring the prevalence of Distress Behaviors in Dementia (DBD), using Minimum Data Set (MDS) items, validated by STAR-VA measures
- Evaluate
- Aim 2: Evaluate the longitudinal impact of STAR-VA by comparing site and resident outcomes at trained and untrained CLCs on DBD, psychotropic use, staff injuries
- Examine
- Aim 3: Examine variations in the sustained implementation of STAR-VA using qualitative methods with a purposeful sample of trained CLCs using Knowledge Reservoir (KR) domains
- Goal
- Goal: Use outcomes to develop a strategy to implement and evaluate a tailored intervention to support CLC teams in sustaining STAR-VA/positive outcomes
AIM 1: Develop MDS 3.0 distress behavior in dementia indicator
- MDS behavior items factor analysis result in two internally consistent factors:
- Distress Behavior in Dementia Indicator (DBDI)
- Wandering scale
- MDS Distress Behavior in Dementia Indicator (DBDI) is:
- significantly related across administrations when given closer in time
- significantly related to validated measures (Cohen-Mansfield Agitation Inventory) as predicted
- sensitive to change
MDS 3.0 Distress behavior in dementia Indicator (dbDi)
| IF I4200 Alzheimer's Disease or I4800 Dementia, THEN ADD: | ||
|---|---|---|
| + | E0200A Physical behavior symptoms directed toward others | 0-3 |
| E0200B Verbal behavior symptoms directed toward others | 0-3 | |
| E0200C Other behavior symptoms not directed toward others | 0-3 | |
| E0800 Rejection of Care | 0-3 | |
| + | E0500A Put the resident at risk of physical illness/injury | 0,1 |
| E0500B Significantly interfere with the resident's care | 0,1 | |
| E0500C Significantly interfere with the resident's participation in activities/social interaction | 0,1 | |
| + | E0600A Put others at significant risk of injury | 0,1 |
| E0600B Significantly intrude on the privacy or activity of others | 0,1 | |
| E0600C Significantly disrupt care or living environment | 0,1 | |
| = | Total Score | 0-18 |
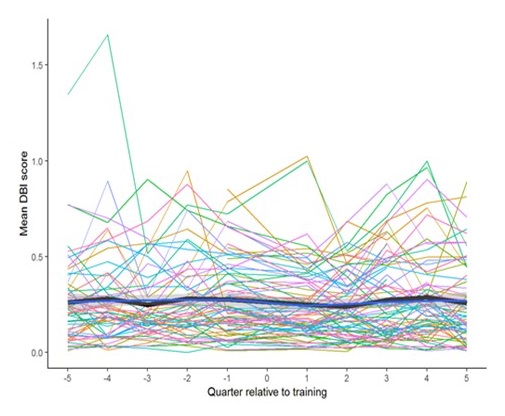
AIM 2: Impact on MDS 3.0 distress behavior in dementia indicator
- STAR-VA impact on MDS DBDI:
- MDS DBDI decreased from pre- to post-intervention
- No significant difference over time in routine MDS DBDI for STAR-VA cases compared to eligible residents at untrained CLCs
- Routine CLC administration of MDS DBDI records fewer behaviors compared with STAR-VA administered DBDI
- Missing data, misaligned assessments
- Little change captured over time
 |
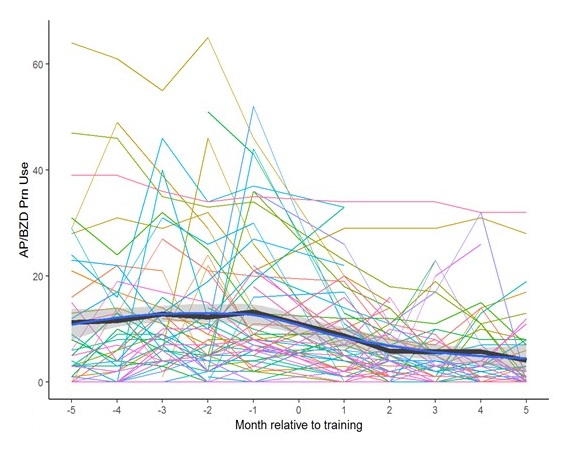
Aim 2: Impact on psychotropic prescribing
- Compared training cases to matched comparison residents at untrained CLCs, accounting for baseline medication use and other factors
- Significant decrease in dose equivalents of as-needed antipsychotic and benzodiazepine meds prescribed for agitation/anxiety in STAR-VA cases (figure) versus comparisons
- Less significant decreases in total antipsychotic and benzodiazepine medication dose equivalents for STAR-VA cases and overall for CLCs trained compared with untrained CLCs
 |
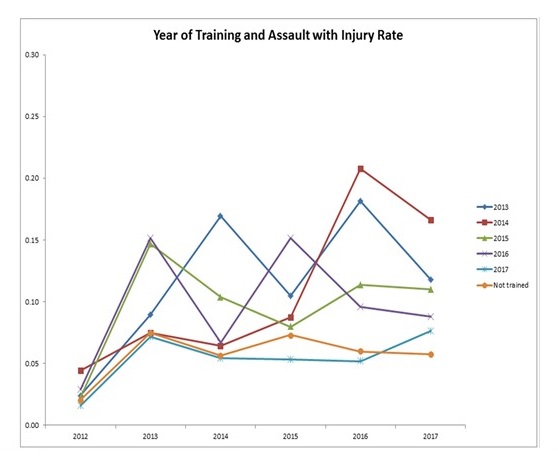
Aim 2: Impact on clc staff injury rates
- Compare staff injury rates due to assault in CLCs that completed STAR-VA training relative to untrained CLCs, accounting for baseline staff injury rates and other factors
- STAR-VA CLCs start with higher rates of staff injury, disruptive behavior reports, DBDI, prevalence of dementia, depression, anxiety, ADC and MH FTE
- Assault with staff injury rates significantly decrease the year of and following completion of STAR-VA training, compared to CLCs not trained
 |
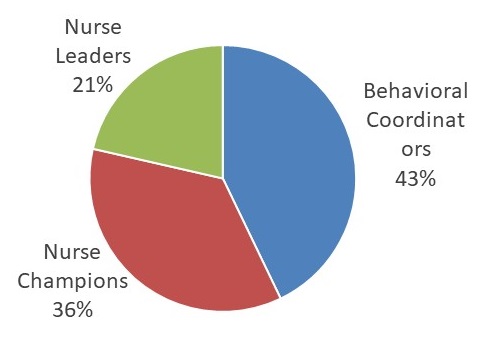
AIM 3: Variation in Sustainment Interview Sample
- 20 CLCs recruited
- 39 interviews conducted from Dec 2018-June 2019
- 42 respondents
- STAR-VA sustainment
- 30% fully sustained implementation
- 65% somewhat to mostly sustained implementation
- 5% very little
 |
Aim 3: Knowledge reservoir Sustainability Framework
- "Sustainable change refers to the continual presence in an organization of all or most of the practices/ activities of an intervention or program" (p. 89)
- "Organizational memory refers to the storage or embodiment of knowledge in various knowledge reservoirs within the organization...the ability of an organization to sustain new initiatives, to institutionalize the initiatives in the organization's standard operating procedures and to ‘routinize' the initiatives to make them a permanent component of the organization" (p. 90)
Verani, T., Lemieux-Charles,L., Davis, D. A., & Berta, W. (2009). Sustaining change: Once evidence-based practices are transferred, what then? Longwoods Review, 6, 89-96.
Knowledge Reservoir Sustainment Framework
| Knowledge Reservoir | Definition |
|---|---|
| People | Organizational members carry information about organization best practices, who knows what, past experience, knowledge from social network, etc. |
| Relationships | Relationships between people, how organizational members interact |
| Organizational Information Space/Tools | Physical and temporal space that allows for organizational members to share information with each other (e.g., emails, conference room) |
| Structure of Performance | Roles (expectations of individuals, correct behaviors), reporting relationships and departmental or project responsibilities |
| Routines and Procedures | Usual routines members use to do their work, standard operating procedures |
| Artifacts and Policies | Documents such as policies and procedures, documenting systems, information technology, reports, educational manuals, etc. |
| Culture | Values, beliefs and attitudes that get reflected in stories, language, behavior and interactions, organizational priorities |
AIM 3: Usefulness/Helpfulness
| For Staff | |
|---|---|
|
" it gave me guidance how to address and deal with behavior problems. It was a learning process for me... it really allows me to structure some of the way in which we can incorporate these behavioral interventions" |
| For Veterans | |
|
"When STAR-VA is no longer a tool, staff turn to medication" "listening to residents really helps lower anxiety, it gives them something to do in these situations where they feel helpless and having that intervention reduces their [anxiety], it makes for a more pleasant environment " "I have seen a tremendous decline in behaviors...once [staff were] more educated on dementia and its expectations and those behaviors, things started getting better and we have come a long, long way" |
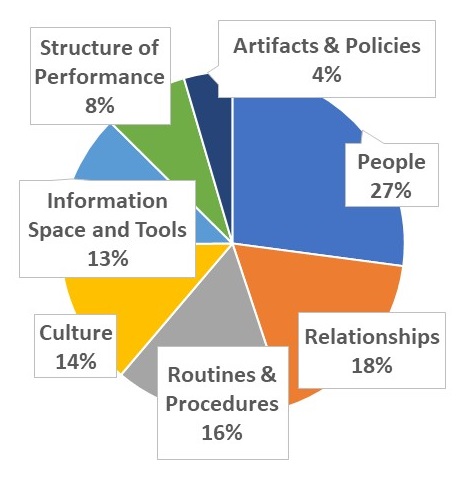
AIM 3: Variations in sustained implementation of STAR-VA
- Qualitative analysis of interview data using the knowledge reservoir (KR) framework for EBP sustainability
- Common themes supporting sustained implementation:
- People -- champions, leaders, direct care workers, the whole team
- Relationships -- team meetings, 1:1 in the moment discussions
- Routines and Procedures -- routine meetings, trainings, documentation
- Culture -- commitment to person- centered care, relative priority, collaborative team
 |
Aim 3: Barriers and Facilitators to Sustained STAR-VA Implementation
| Key Barriers | Key Facilitators |
|---|---|
|
|
Sustaining STAR-VA Queri: summary
- STAR-VA implemented more often in CLCs with higher rates of dementia, MH diagnoses, DBDI, disruptive behavior reports, staff injuries
- Teams view STAR-VA useful and helpful
- MDS Distress Behavior in Dementia Indicator (DBDI) is reliable, valid, and sensitive to change
- Routine MDS DBDI under-reports and not aligned with timing of intervention
- STAR-VA results in significant decreases in staff injuries and use of as- needed antipsychotic and benzodiazepine medications
- STAR-VA does not impact current routine behavior measures
- Relationships, People, Routines and Procedures, Information Sharing, and Culture are key to sustainability
- Matching barriers to strategies based on expert consensus -- needs assessment, implementation blueprint, network weaving
Star-VA program: next steps
- Use MDS DBDI to provide routine feedback to CLC teams to guide care (supplement with more frequent assessment)
- Develop STAR-VA sustained implementation guide and checklist
- Readiness assessment, implementation steps, sustainment strategies
- Encourage teams to select and track Quality Improvement (QI) outcomes
- Partner with ongoing CLC QI/teamwork initiative
- Engage and empower direct care staff
- Use huddles for communication, problem-solving
- Foster supportive leadership and work culture
- Champion succession planning, ongoing consultation
- Regional communities of practice
STAR-VA Resources
For information about STAR-VA, including link to the intervention manual, citations, and an on-line broadcast providing a program orientation, see: https://www.mentalhealth.va.gov/healthcare-providers/docs/STAR-VA_Overview.pdf
Points of contact:
Kimberly.Curyto@va.gov
Michele.Karel@va.gov