Monday, January 27, 2020
Printer Friendly Version in PDF Format (12 PDF pages)
What is EPIDEMIOLOGY, and what does it offer for understanding, treating, and preventing Alzheimer's?
Deborah Blacker, MD, ScD
Professor of Psychiatry, Mass General Hospital/Harvard Medical School
Professor and Deputy Chair in Epidemiology, Harvard T.H. Chan School of Public Health
OVERVIEW
- What is Alzheimer's?
- What is epidemiology?
- Major functions
- Assess and forecast the magnitude of the problem (brief intro to Dr. Langa's talk)
- Understand risk and protective factors and their potential role in prevention (brief intro to Dr. Yaffe's talk)
- Put clinical findings in a population context
- Assess and improve methods for observational studies
WHAT IS ALZHEIMER'S?
- Alzheimer's disease (AD) dementia is a type of dementia caused by a specific neuropathology--amyloid plaques and neurofibrillary tangles
- Confusingly, AD is used both to refer to the pathology and the clinical syndrome caused by the pathology
- Dementia and Mild Cognitive Impairment (MCI) are clinical diagnoses based on cognitive and functional status and can be caused by AD pathology or other pathologies
- Also confusingly, AD and dementia are sometimes used interchangeably, in part because AD is the most common form of dementia
Clinical vs. pathological diagnosis
- A definitive diagnosis of AD requires evidence of AD pathology from biomarkers or autopsy, but diagnosis in clinical and population studies is often based on symptoms alone
- Whether this matters depends on the purpose
- Fine for understanding disease burden or costs, but problematic for targeted clinical trials, and complicates the interpretation of epidemiologic and genetic studies
Additionally complicating the interpretation of research findings...
- AD pathology often co-occurs with other pathologies, particularly cerebrovascular pathology
- The effects of these different pathologies are at least additive and may interact
- At later ages, mixed dementia is very common, and additional pathologies likely remain to be identified
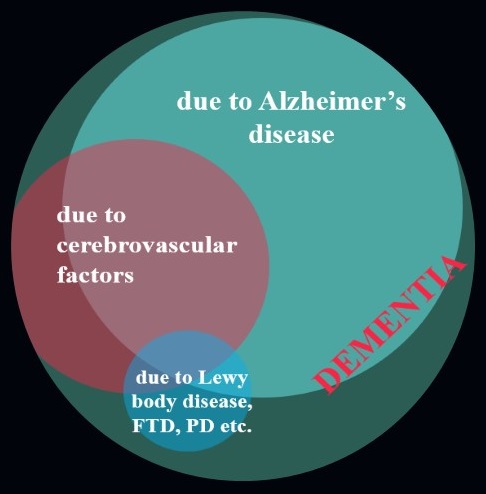 |
| Graphic courtesy of Dr. Jennifer Weuve |
WHAT IS EPIDEMIOLOGY?
- Initial focus on infectious disease-- surveillance, containment, etc.
- Later parallel focus on chronic disease-- to understand disease burden, patterns over time and space, and understand risk factors
What do epidemiologists do?
- Quantify disease in the population overall, according to demographic factors, and across time and space
- Use patterns of association and careful statistical analysis to understand risk and protective factors, offering insight into mechanism and prevention
- Assess whether findings from clinical studies hold up in the general population, with implications for screening and real world impact of interventions
- Assess and develop optimal methods for observational studies, with implications for clinical trials, screening, and health services
DESCRIPTIVE EPIDEMIOLOGY: Magnitude and patterns
- How many people have the disease now? (Prevalence)
- How many new cases can be expected... (Incidence)
- at a given age or in a given time window?
- cumulatively until a certain time ?
- over a lifetime?
- How do the above numbers change across demographic factors, geographic regions, and birth cohorts?
Descriptive Epidemiology: Magnitude and patterns
- Provides estimate of disease burden to inform care planning, policy, and research priorities
- Big picture suggests rising rates overall despite apparent fall in age-specific incidence* --and that's why we are here today!
- Stay tuned: Details from Dr. Langa
RISK AND PROTECTIVE FACTORS
- Use associations to discover factors that increase or decrease disease risk
- Risk and protective factors can be genes or diet , activities, medical conditions, or local environment
- Can identify high risk populations or select intervention strategies for clinical trials
- Can be translated into individual health recommendations and population health policy
- Can help understand mechanism and drug development
| At Baseline |
10 years later |
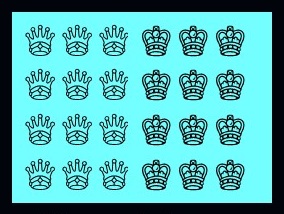 |
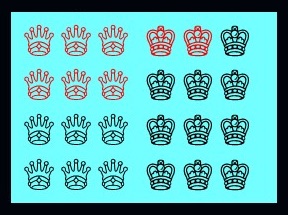 |
| Spiky crown may be a risk factor for turning red after 10 years |
Examples
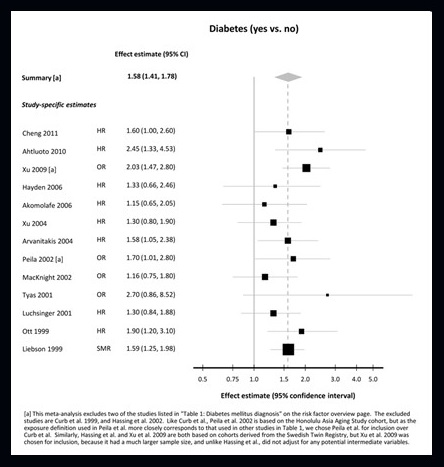
| Systematic Review of risk of dementia with diabetes |
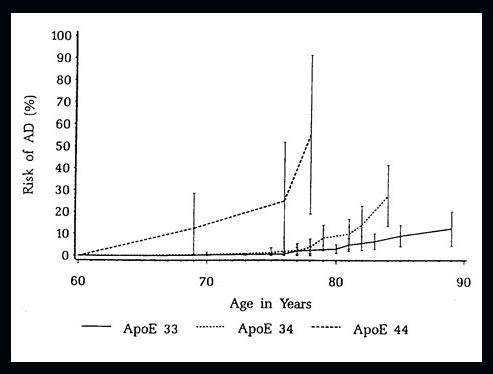
Cumulative incidence of dementia by APOE-4 dose: Framingham Study |
 |
 |
| Weuve et al., AlzRisk, Alzheimer Research Forum, http://www.alzrisk.org/ |
Myers et al., Neurology, 1996 |
Stay tuned: Details from Dr. Yaffe
PUT CLINICAL RESEARCH AND EXPERIENCE INTO A POPULATION CONTEXT
- Patients are more impaired than average for the same diagnosis (e.g., MCI, because symptoms drive care-seeking), and also have more other illnesses that may unmask decline, increase contact with doctors, etc.
- Patients are also more educated, more affluent, and have other attributes that increase access to care
- However, screening programs, publicity, or the availability of early intervention can bring those with milder illness into care
- Research volunteers are often highly educated, and more likely to have family history, subclinical symptoms, etc.
NACC vs. population samples
| Study |
NACC |
FHS |
Rotterdam |
| Description |
US volunteer, 80% white |
US pop, 1°ly white |
European pop, white |
| N |
5073 |
4078 |
6399 |
| mean (sd) age (yrs) |
68.7 (4.30) |
62.0 (1.71) |
65.4 (4.18) |
| % male |
33.6% |
43.2% |
45.2% |
| mean (sd) educ (yrs) |
15.79 (2.99) |
13.20 (*) |
12.94 (*) |
| E-4 allele freq |
0.178 |
0.117 |
0.150 |
| % w/ family history |
58.3% |
N/A |
21.7% |
| % w/ memory concerns |
24.9% |
N/A |
43.1% |
| mean (sd) MMSE |
29.0 (1.3) |
28.5 (1.0) |
28.8 (1.4) |
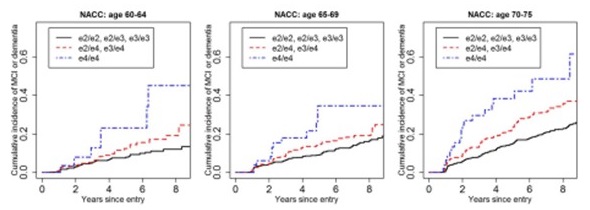
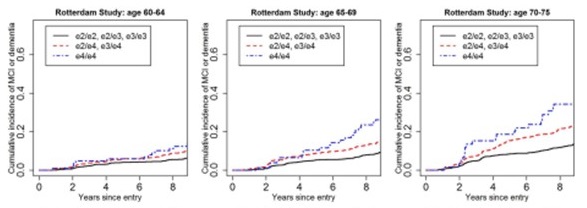
Cumulative Incidence of MCI/dementia by APOE dose
| Alzheimer Centers (NACC) |
 |
| Rotterdam Study |
 |
| Framingham Heart Study |
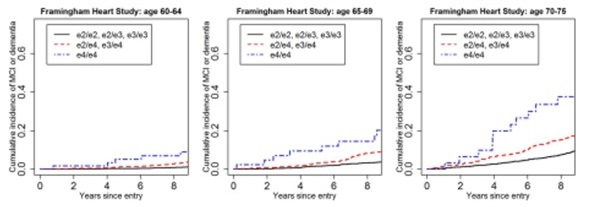 |
| Qian et al, PLoS Medicine, 2017 |
Example: 23andMe APOE Testing
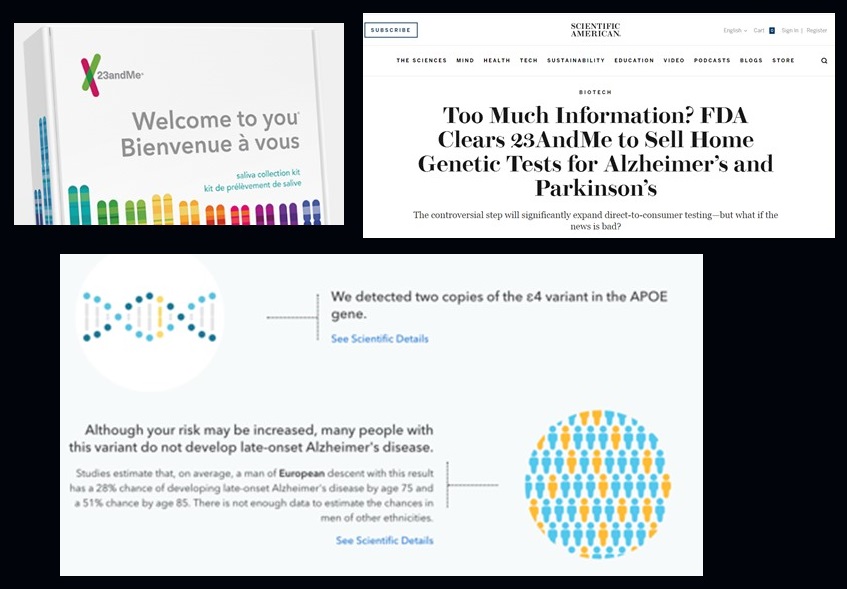 |
| Sample report courtesy of Robert Green and Debby Tsuang |
Importance of Population Context
- 23andMe's risk estimates are too high (likely because they're based on data from clinical/volunteer samples)
- Similar issues apply for imaging, biomarkers, and clinical symptoms tested in clinical/volunteer settings
- Critical issue whenever findings from one setting are applied in another; examples:
- The MCI trial of donepezil turned to community recruiting when clinical recruiting ran short, but lower onset rate of dementia in community participants reduced the study's power
- Expected rates of developing dementia based on biomarker data from clinical samples of MCI will be lower if a new treatment becomes available, as that would drive less impaired individuals to seek care
ASSESS AND IMPROVE METHODS FOR OBSERVATIONAL AND OTHER CLINICAL RESEARCH
- Caveat Auditor
- Epidemiology focuses on observational research, so has developed careful methods to guard against and quantify potential false or distorted conclusions
- The importance of these details depends on the question
- Causal questions are particularly vulnerable to biases, and are critically important to translational applications
- EPIDEMIOLOGIST: noun. [ep-i-dee-mee-ol-uh-jist] someone who solves a problem you didn't know you had in a way you don't understand. See also wizard, magician.
Key issues that can lead to bias
- Measurement error: over or under-calling dementia or MCI outcome, noise in measuring cognitive or functional status, mismeasurement of risk factors
- Sampling issues: impact of entry criteria and operational definition of non-demented at baseline, age at entry and survival bias, participant burden, and autopsy consent
- Confounding: something related to both your outcome and to your putative risk factor that creates a spurious association between the two-age and education are major confounders in AD research
- Reverse causation: an effect masquerading as a cause
- Will illustrate by raising some questions about whether cognitive activity really reduces risk of dementia
Measurement Error
- A particular concern for cognitive testing, MCI, and any diagnosis in claims or health records; mostly adds noise and reduces power, but can lead to biased findings if differentially affects each side of the question at hand
- For understanding the role of cognitive activity in risk for dementia, typical cognitive activity surveys focus on activities of the highly educated, which could make high levels of activities look protective when education is actually providing the benefit
Sampling bias
- In the examination of cognitive activity and risk of dementia, because there is a broad perception that cognitive activities are desirable, those who are inactive may be reluctant to participate (or may over-report their activity--see measurement error), or those who are very active may be too busy
- Survival bias could also distort the relationship if those with greater levels of cognitive activity live longer, as might be expected given the association of longevity and education
Confounding
- Age and education are major confounders that affect measurement, care seeking, and multiple risk factors
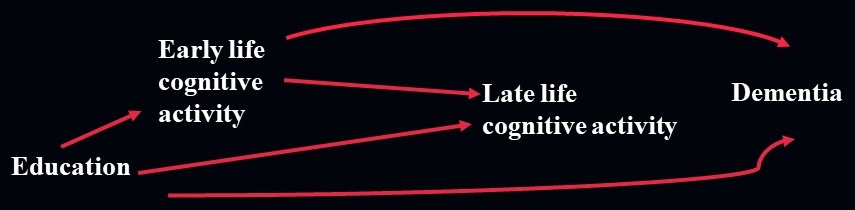
- For cognitive activity and risk of dementia, the big concern is education, which is associated with greater cognitive activity, but contributes to dementia risk in multiple other ways
- Or, early life cognitive activity might build protective "brain reserve," and later effects might be observed simply because those habits persist over time
Reverse causation
risk factor → dementia VS. dementia → "risk" factor
- Given insidious onset of dementia, incipient cognitive decline can lead to changes in physiologic state (weight, BP) or lifestyle, which can in turn be mistaken for causes
- Decline in cognitive activity in the face of early cognitive decline is highly plausible, and careful bias analysis cannot rule out reverse causation driving the apparent lower risk of dementia
 |
| Graphic courtesy of Dr. Jennifer Weuve |
Parting words on the value of epidemiological methods
Guidelines for reporting methodological challenges and evaluating potential bias in dementia research https://www.sciencedirect.com/science/article/pii/S1552526015021226
Acknowledgements
- Thanks to Brad Hyman and NAPA for the invitation, to Ken Langa and Kristine Yaffe for joining, and to all of you
- Thanks to many others for contributions and insights:
- MGH/MADRC: Brad Hyman, Mark Albers, Sudeshna Das, Yi-Han Sheu, Lidia Moura, John Hsu
- HSPH/Erasmus Epidemiology/Biostatistics: Albert Hofman, Frank Wolters, Yuan Ma, Gautam Sajeev, Sebastien Haneuse, Rebecca Betensky
- Melodem: Jennifer Weuve, Mindy Power, Maria Glymour
- ADRC Disclosure Workgroup: Ellen Wijsman, Jasmeer Chhatwal, Malia Rumbaugh
- FUNDING:
- National Institute on Aging
- National Institute of Neurological Disorders and Stroke
- Harvard Medical School
- Fidelity Foundation