
U.S. Department of Health and Human Services
High Service or High Privacy Assisted Living Facilities, Their Residents and Staff: Results from a National Survey
Catherine Hawes and Charles D. PhillipsTexas A&M University System Health Science Center
Miriam RoseMyers Research Institute
November 2000
PDF Version: http://aspe.hhs.gov/daltcp/reports/hshp.pdf (90 PDF pages)
This report was prepared under contracts #HHS-100-94-0024 and HHS-100-98-0013 between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging, and Long-Term Care Policy (ASPE) and Research Triangle Institute. Additional funding was provided by American Association of Retired Persons, the Administration on Aging, the National Institute on Aging, and the Alzheimer's Association. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Gavin Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail address is: Gavin.Kennedy@hhs.gov
This report was prepared under contracts HHS-100-94-0024 and HHS-100-98-0013 from the Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation (ASPE), U.S. Department of Health and Human Services. AARP, the Alzheimer's Association and the National Institute on Aging have also provided support for this project. The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
A. Emergence and Growth of the Assisted Living Industry
B. Defining Assisted Living
C. Expansion of State Policy Concerning Assisted Living
D. Lack of Information on the Assisted Living Industry
E. The Current Study
F. Organization of the Report
II. STUDY METHODS
A. Defining Assisted Living Facilities: Overall Study Eligibility
B. Rationale for Exclusions for Eligibility
C. Data Collection in Eligible Facilities
D. Identifying Facilities for Site Visits
E. Sampling
F. Analytic Strategy
III. RESIDENTS IN ASSISTED LIVING FACILITIES (ALFs) OFFERING HIGH SERVICE OR HIGH PRIVACY
A. Demographic Characteristics
B. Entry Into Facilities and Length of Stay
C. Health and Functional Status
D. Unmet Needs
E. Health Conditions and Service Use
F. Resident Experiences and Ratings of Facility Performance
G. Summary
IV. STAFF WORKING IN HIGH PRIVACY AND HIGH SERVICE ASSISTED LIVING FACILITIES
A. Staff Characteristics and Training
B. Staff Activities and Tasks
C. Staff Knowledge of Aging and Care
D. Staff Satisfaction
E. Salaries and Workload of Aides/Assistants
F. Summary and Conclusions
V. RESULTS OF THE WALK-THROUGH OBSERVATIONS IN HIGH PRIVACY OR HIGH SERVICE ALFs
A. Safety and Supportive Features in High Privacy or High Service ALFs
B. Community Rooms and Dining Areas
C. Outdoor Areas in High Privacy or High Service ALFs
D. The Neighborhood and Exterior Appearance of the ALFs
E. Summary of Walk-Through Observations
VI. FACILITIES, ADMINISTRATORS, AND POLICIES
A. Ownership and Operations in High Service and High Privacy ALFs
B. Facility Policies and Resident Autonomy
C. Resident Case Mix in High Privacy or High Service ALFs
D. Resident Turnover, Length of Stay, Admission and Discharge Policies
E. Staffing
F. Price and Services in High Privacy or High Service ALFs
G. Administrators' Concepts of Assisted Living
H. Summary
VII. CONCLUSIONS
A. How Impaired Were Assisted Living Residents?
B. What Types of Services Were Available to ALF Residents?
C. Was Staffing Adequate in ALFs?
D. Were Policies in High Privacy or High Service ALFs Generally Consistent with ALF Philosophy?
E. Could ALF Residents Age in Place?
F. Could ALFs Substitute for Nursing Home Care?
G. What Did Residence in an ALF Cost?
EXHIBITS
EXHIBIT II.1: Tier Classification of Survey-Eligible Facilities by Level of Privacy and Level of Service
EXHIBIT II.2: Distribution of ALFs by Mix of Services and Privacy
EXHIBIT III.1: ALF Resident Characteristics
EXHIBIT III.2: Entry Into an ALF
EXHIBIT III.3: Cognitive Impairment of Residents in High Privacy or High Service ALFs
EXHIBIT III.4: Cognitive Impairment and Type of ALF
EXHIBIT III.5: Physical Function
EXHIBIT III.6: Physical Health
EXHIBIT III.7: Positive Resident Ratings of Staff
EXHIBIT III.8: Activities
EXHIBIT III.9: Living Arrangement and Meals
EXHIBIT III.10: Resident Report on Arrangements When Temporary Nursing Care was Needed
EXHIBIT IV.1: Staff Characteristics
EXHIBIT IV.2: Staff Duties
EXHIBIT IV.3: Staff Views of What is a Normal Part of Aging
EXHIBIT IV.4: Staff Opinion of How to Manage Resident with Memory Loss
EXHIBIT IV.5: Staff Satisfaction
EXHIBIT IV.6: Wages of Personal Care Assistants in High Privacy or High Service ALFs
EXHIBIT V.1: Resident Use of Communal Spaces in ALFs
EXHIBIT V.2: Facility Outdoor Area
EXHIBIT V.3: General Impressions of Facility
EXHIBIT VI.1: ALF Ownership
EXHIBIT VI.2: Facility Ownership and Affiliation
EXHIBIT VI.3: Facility Policies and Resident Autonomy
EXHIBIT VI.4: Facility Admission Policy
EXHIBIT VI.5: Full and Part-Time Licensed Nurses in High Privacy or High Service ALFs
Exhibit VI.6: Distribution of Monthly Basic ALF Price
EXHIBIT VI.7: Services Provided and Arranged by ALFs and, if Offered, Whether Included in the Basic Monthly Rate
EXHIBIT VI.8: Facility Policies When Private Funds are Exhausted
EXHIBIT VI.9: Administrators Concepts of Assisted Living
EXECUTIVE SUMMARY
Background
The most rapidly growing form of senior housing in recent years has been a form of supportive housing or residential long-term care known as assisted living. This growth has been a response to several factors, including the aging of the population, the preferences of the elderly for settings other than nursing homes, the availability of private financing for development and construction of assisted living facilities (ALFs), and public policies aimed at containing use of nursing homes.
The Office of the Assistant Secretary for Planning and Evaluation (ASPE), in the U.S. Department of Health and Human Services, has a long-standing interest in the ability of residential and community-based service providers to meet the needs of the elderly and people with disabilities. As a result, ASPE has funded several studies of residential long-term care, including this first national study of ALFs for the frail elderly. ASPE's interest in assisted living and its ability to meet the needs of the frail elderly has been heightened during the study by a series of reports and a Congressional hearing that raised concerns about quality and consumer protection in assisted living (U.S. General Accounting Office, 1997 & 1999).
The Study
Despite growing interest and a rapidly expanding industry, the knowledge base available to those interested in assisted living is quite limited. Most prior and on-going research has been confined to a relatively small number of facilities and states. However, this study, A National Study of Assisted Living for the Frail Elderly, is based on data collected in a nationally representative sample of ALFs. Several reports based on the data collected about these facilities are available, and each provides data on a sample that is representative of a nationwide universe of ALFs, residents and staff. Those reports include:
-
The results of a telephone survey of approximately 1500 ALFs that describes the universe of ALFs nationwide;
-
A description of the policies and practices, residents, and staff in that segment of the ALF industry that provides the highest level of services and privacy;
-
A description of residents who were discharged from the high service or high privacy ALFs within six months of our initial interview;
-
A report that examines the effect of different environmental and service configurations on such issues as resident satisfaction, the ability of residents to age in place, and the price of assisted living; and
-
A final report that summarizes the findings across all the reports and specifically addresses key study questions, such as the degree to which the current assisted living industry exhibits the philosophy of assisted living and the effect of the mix of services and privacy on residents.
This report is the second of those mentioned above. It reports data on a nationally representative sample of residents and staff in ALFs classified as providing relatively high services or offering a high privacy environment. These facilities, which comprise about two-fifths (41%) of the places calling themselves assisted living, were selected for more extensive and in-depth data collection because they seemed to most effectively exhibit key elements of the philosophy of assisted living.
Study Methods
The national population of ALFs sampled for this study included only certain types of residential care settings. The population included all residential care facilities with 11 or more beds that primarily served the frail elderly and that publicly represented themselves as providing assisted living. It also included facilities that did not specifically identify themselves as assisted living but that appeared on some listing of residential care providers and met study criteria for size, mission, privacy and service.1 A telephone survey of a national probability sample of such facilities, representing nearly 11,500 facilities across the nation, formed the basis for our first study report (Hawes, Rose, & Phillips, 1999a and 1999b).
| Distribution of ALFs Nationwide and Those Included in This Report | |||
| High Services | Low Services | ||
| High Privacy | 11% of all ALFs IN | 18% of all ALFsIN | |
| Low Privacy | 12% of all ALFsIN | 59% of all ALFs EXCLUDED | |
As noted, this report focuses on a subset of two-fifths (41%) of the original sample. The facilities in the original sample were divided into groups, based on the level of privacy (i.e., high and low/minimal) and the level of service (i.e., high and low/ minimal) that they provided. An explanation of the way in which these groups were defined is discussed in detail in Section II of the report. Facilities in three of these groups (i.e., high service & high privacy, high service & low privacy, low service & high privacy) were chosen for further study through site visits that included more detailed data collection. The site visits included interviews with facility administrators, staff, residents, and family members, as well as a "walk-through" evaluation of the facility environment. The 300 facilities involved in the site visits represented a population of 4,383 ALFs across the nation -- or all those that met the definition of a facility that offered either high services or high privacy.
The Results
ALF Residents. The residents in the high privacy or high service ALFs were largely white, widowed females, who were quite elderly. More than one-half of the residents were 85 years of age or older. ALF residents were relatively well-educated; 45 percent had completed at least some college. They were also relatively affluent. Most entered assisted living from their own home or apartment (70%) and made the decision with help from someone else (90%), almost always their adult children. However, one-quarter of residents indicated that they had little or no control over the decision to enter a facility.
- ½ were aged 85 or older
- Largely white, widowed females
- Educated, relatively affluent
- About ¼ had significant cognitive impairment
- One in five had ADL assistance
- Two in five reported themselves in fair or poor health
Over one-quarter (27%) of the residents suffered from moderate or severe cognitive impairment, one-half of residents (51%) received assistance with bathing, and one-fifth of residents received assistance in some other activity of daily living. The overwhelming majority (77%), however, received help with their medications, and many residents used assistive devices, especially to help with ambulation or locomotion. Almost one-third (32%) experienced urinary incontinence. Two-fifths of the residents considered themselves in only fair or poor health, and, in the year prior to their interview, they used inpatient services at rates much higher than the general population.
Residents were relatively satisfied with the attitudes of staff and how staff treated them (e.g., with respect and affection). Their greatest points of concern about staff were related to inadequate staffing levels and high staff turnover. Residents were split almost evenly in their perceptions of the availability of activities they enjoyed and on the availability of transportation to events they might enjoy. One of the more unsettling findings concerning activities was that almost three-fifths of the residents (59%) indicated that ALF staff never or only sometimes asked them about their activity preferences.
- Generally felt they were treated with respect, affection and dignity
- Were relatively concerned about staffing level and turnover
- Were somewhat rarely asked about their activity preferences by facility staff
- 12% of residents who received help with locomotion and dressing and 26% who needed help with using the toilet reported having unmet needs for assistance
- Nine of ten believed they would be able to stay in the ALF for as long as they wished
- Most were uninformed about facility policies on retention and discharge
Assisted living residents in ALFs classified as providing high services or high privacy were almost equally likely to be found in accommodations consisting of a full apartment or only a bedroom. The majority (81%) had a private living space or shared it with a related individual; however, nearly one-third of the residents did not have a private full bathroom. Most residents (i.e., more than three-quarters) also had other types of autonomy over their environment, such as ability to lock their doors, furnish their apartments and arrange the furniture as they wished, and control the temperature in their room or apartment. Only about half, however, had a refrigerator and only about one-third had space for cooking. Most had access to key supportive devices, such as call buttons and safety railings in the bathroom.
When they needed temporary nursing care, they were most likely to receive it from the facility staff; however, one-third of the residents who needed such care were either discharged to a hospital or nursing home or, with family members, arranged for home health themselves. Finally, fewer than one-third of the residents reported being informed by the facility about the discharge and retention policies. Despite this, the vast majority of residents expected to be able to stay in the facility for as long as they wished.
ALF Staff. The project investigated facility staff's knowledge of the appropriate response in a variety of situations involving relatively common health problems among frail older persons. In many instances, the vast majority of staff was aware of the proper response to specific situations, including most medication management issues. On the other hand, a significant number of staff members were poorly informed about antipsychotic drugs and some issues related to the care of individuals with dementia. More troubling, the majority of staff members were almost completely unaware of what constitutes normal aging. Given the goal of enabling residents to age in place and the advanced age of current residents, these results are particularly disquieting. Poor training and knowledge in these areas may in the future become more and more troublesome and risky, both for providers and residents, since many of the conditions staff identified as a "normal part of aging" were potentially treatable and reversible.
- Were knowledgeable about many care issues
- Were less knowledgeable about dementia care and very uninformed about normal aging
- Staff appeared satisfied with most aspects of work, except salary and advancement opportunities
- Median staffing level was 14 residents for each caregiver
- Two in five reported themselves in fair or poor health
Most staff in the high privacy or high service ALFs reported relatively high levels of satisfaction or positive affect toward their working conditions. Two areas, however, were a concern or area of low satisfaction for most staff. The first was their pay level, which usually ranged from between five and nine dollars per hour for personal care attendants. They also expressed dissatisfaction with what they viewed as limited possibilities for advancement.
Personal care staff did not report their workload as overly heavy, and the median number of residents for whom they cared was fourteen.2 In a nursing home this level of staffing would cause concern for some experts. However, as discussed above, the ALF residents were not as impaired as nursing home residents. At the same time, the survey demonstrated that most direct care staff in ALFs also had responsibility for a variety of tasks in addition to direct resident care, including housekeeping, laundry, and meal service. This complicates any attempt to evaluate the adequacy of staffing levels or compare them to those in other settings.
Walk-Through Observations. The observers' judgments about the physical plant in assisted living facilities indicated that these settings were largely well-maintained, clean, relatively homelike settings for the frail elderly with a wide range of social and recreational resources. Most were in suburban areas, and nearly half (46%) were single story buildings.
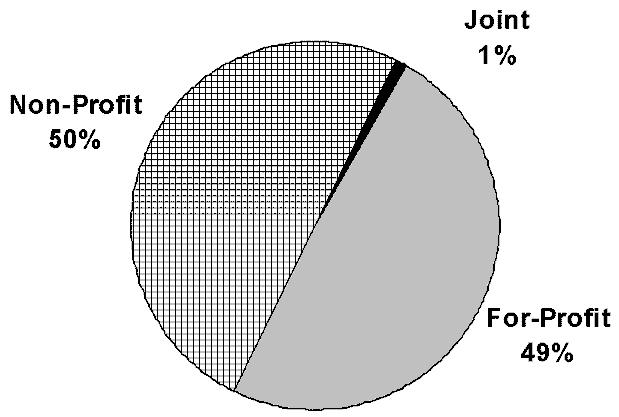
Facilties, Administrators, and Staffing. Assisted living facilities were almost equally likely to be operated by for-profit as by not-for-profit entities. However, the vast majority (79%) of organizations that owned or operated the high service or high privacy ALFs were involved in the operation of other types of supportive housing for the elderly, such as nursing homes and congregate apartments. Almost two-thirds (64%) of the not-for-profit ALFs, for example, were located on a multilevel campus that housed various types of supportive housing for the elderly, including a nursing home. Indeed, nearly half (49%) the owners of all of the high service or high privacy ALFs owned or operated nursing homes, and nearly half (46%) of these ALFs were part of a multi-facility system or "chain" of assisted living facilities.
| Ownership in High Privacy or High Service ALFs |
 |
Facilities showed some variation in the level of functional limitations and cognitive status among their residents. In most ALFs, relatively few residents had significant functional limitations and care needs. In most ALFs, assistance with medications was the only area in which they reported most residents needing and receiving help. However, approximately 15 percent of ALFs seemed to have a substantial proportion of residents with somewhat heavier physical care needs, such as need for help with transfers and other middle-range and late loss ADLs. Administrators also reported fairly high "turnover" rates among residents, with an average annual rate of 41 percent of the residents each year.
Staffing varied considerably across facilities. According to administrators, on first shift, one-quarter of the ALFs had direct care staff to resident ratios of 8-to-1 or lower, and another quarter had ratios of 16-to-1 or greater. (In evaluating these reports, it is important to remember that the personal care attendants (PCAs) reported very different staffing ratios, with a median of 1-to-14 and one-quarter of the PCAs reporting that they cared for 23 or more residents). While staffing ratios varied considerably, there was some consistency across ALFs in the types of staff used. For example, the sampled ALFs that were site visited almost universally utilized some licensed nursing services. Staff turnover was lowest among licensed nursing staff, but administrators estimated that roughly one-quarter of all direct care staff turned over during the course of a year.
- Half were for-profit businesses and half were not-for-profit entities
- Most ALF owners engaged in some additional type of long-term care service provision
- There was considerable variation in staffing
- Median price is $1,800 per month
- There was wide variation in which services were covered by the base rate
The most common basic monthly charge in the high privacy or high service ALFs was between $1,735 per month and $19,990 -- or an average of about $1,800. However, because of the diversity among ALFs in the number and types of services included in that base rate, one is not quite sure what that sum purchased. For example, relatively few facilities (36%) provided temporary nursing care as part of their base monthly rate, while a substantial majority (80%) provided planned recreational activities. For those residents who exhausted their funds paying at this level, many facilities were willing to accept payments from alternative sources if they were available (e.g., charity, SSI, Medicaid). However, policy in a substantial proportion of facilities (45%) required the discharge of those who exhausted their private financial resources.
Conclusions
There are a number of policy issues surrounding the emergence and growth of assisted living and its ability to help meet the long-term care needs of the elderly and disabled. This report begins to address some of these by focusing on only those facilities that seem to most closely embody the philosophical tenets of "assisted living." Thus, the report describes the facilities that offer either high privacy or high services -- or both -- and their policies and practices, particularly with respect to services, policies on autonomy and resident control, and staffing. Further, this report describes the characteristics of the residents and their perceptions about the care they receive and the environment of the facilities in which they live. In providing this descriptive data, we begin to address questions about the role and performance of assisted living facilities and their place in the constellation of long-term care services. We also attempt to relate the descriptive data to the central study questions about whether ALFs embody the principles of assisted living and whether the needs of residents are being met. These issues are discussed at length in Section VII on conclusions. Finally, it is important to note that even in this special subgroup of ALFs, there was tremendous variability in ownership, size, staffing, policies, and performance along key dimensions.
In conclusion, assisted living appears to offer an important type of residential long-term care setting for persons with mild or moderate disabilities who cannot safely or securely live alone but do not need the level of care provided in a nursing home. Further, the high privacy or high service ALFs provide this care in a setting that has many components valued by consumers, particularly in terms of privacy and environmental autonomy. In addition, most high service or high privacy ALFs offered a wide array of services. The issue of whether such services can meet residents' unscheduled needs is more complex. Moreover, the degree to which such facilities enable residents to age in place is clearly mixed unless one limits the concept to one of "aging in place without significant decline in physical or cognitive functioning." Finally, assisted living is still a largely private-pay sector and, among the high service or high privacy ALFs, one that is largely unaffordable for most moderate and low income older persons unless they spend down their assets or receive help from relatives.
I. STUDY BACKGROUND
The last decade has seen the emergence and growth of a new industry known as assisted living. Consumer demand, concerns about nursing home quality, pressure from providers, and the availability of capital for construction and conversion have combined with states interest in containing long-term care costs to produce dramatic growth in this industry. Initially, this development was largely an unregulated market response to both demographic trends and consumer preferences. More recently, however, state involvement in setting standards and developing Medicaid payment policies for assisted living has expanded exponentially (Mollica, 1998). Despite this, there is tremendous variability among facilities known as assisted living (ALFA, 1998; Gulyas, 1997; Hawes, Rose & Phillips, 1999; Hodlewsky, 1998). Further, relatively little is known about the assisted living industry and its residents. This dearth of information is problematic, given the rapid growth of the assisted living industry, its increasingly prominent role in providing long-term care for the frail elderly, and the largely uncritical enthusiasm for assisted living that has dominated the policy process.
Because of the promise of assisted living, its rapid growth, and the lack of broadly generalizable information about the industry and its performance, the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation (ASPE) has funded a number of studies to examine the role of residential care and its newer incarnation, assisted living. The current ASPE study is known as A National Study of Assisted Living for the Frail Elderly.
A. Emergence and Growth of the Assisted Living Industry
The graying of the American population represents a major public policy challenge, particularly given estimates that the number of elderly needing long-term care will double to 14 million over the next two decades (US-GAO, 1999). Some commentators liken the effects of this trend on public expenditures for social and health services to the development of a fiscal black hole (Callahan, 1987). As a result, there have been a number of private and public sector responses to meeting this growing need for long-term care (Harrington, Dunah and Carillo, 1994; Williams & Temkin- Greener, 1996). The most dramatic response in the long-term care sector has been the emergence and growth of facilities known as assisted living (American Seniors Housing Association [ASHA], 1998; Citro & Hermanson, 1999; Mollica, 1998). For the last several years, assisted living residences have dominated new construction of housing for seniors3 (ASHA, 1998). Indeed, one-third of facilities that call themselves assisted living have been in business for five or fewer years, and 60% have been in operation for ten or fewer years (Hawes, Rose & Phillips, 1999).
B. Defining Assisted Living
The key elements or philosophical tenets of assisted living are based on the premise that assisted livings goal is to meet customers scheduled and unscheduled needs, promote independence, autonomy and dignity among consumers, and enable residents to age in place in a home-like environment (Assisted Living Quality Coalition4, 1998; ALFA, 1998; Gulyas, 1997; Hodlewsky, 1998; Kane & Wilson, 1993). This philosophy is typically translated into an operational definition of an assisted living facility (ALF) as one that provides or arranges at least the following: 24-hour staff, housekeeping, at least two meals a day; and help with at least two activities of daily living (ADLs).5 There is less agreement among members of the industry on the environmental characteristics of assisted living; however, privacy is typically considered a key element of assisted living (Assisted Living Quality Coalition, 1998; Citro & Hermanson, 1999; Gulyas, 1997; Hodlewsky, 1998).
It has been difficult to arrive at a precise estimate of the number of ALFs in the U.S. for three reasons. First, there is no federal regulation and thus no national listing of facilities. Second, definitions vary across states and because of this, it is often difficult to distinguish assisted living from other types of housing with supportive services, such as board and care homes, personal care homes, and other types of residential care facilities. Third, some states do not license ALFs that consist of apartments. As a result, many estimates include a multitude of different types of facilities, some of which do not meet the common conception or definition of assisted living. For example, the Assisted Living Federation of America (ALFA) estimated that there were more than 40,000 ALFs nationwide in 1998 (ALFA, 1998; Citro & Hermanson, 1999). However, this estimate appears to have included small board and care homes, as well as other facilities.
As part of this study, A National Study of Assisted Living for the Frail Elderly, project staff developed a more explicit definition of assisted living and created a sampling frame from which a national probability sample of ALFs was selected. This operational definition limited ALFs to those facilities that served the elderly, had more than ten beds, had no rooms shared by three or more residents, and either advertised themselves as assisted living or provided key services, including assistance with two or more activities of daily living.6 By this definition, as of the start of 1998, there were an estimated 11,500 ALFs nationwide with more than 611,000 beds7 (Hawes, Rose & Phillips, 1999). As a point of comparison, there were an estimated 17,000 nursing homes with 1.6 million beds in 1996 (Krauss et al., 1997).
C. Expansion of State Policy Concerning Assisted Living
While assisted living initially developed in the U.S. largely in the absence of regulation or public financing, states have more recently moved fairly rapidly to develop and implement assisted living regulations.8 The first licensure regulation specifically directed at assisted living was passed in Oregon in 1989. By 1992, fewer than 10 states had such regulations in place (Mollica & Snow, 1996). By 1998, however, 30 states had passed legislation or issued regulations. Other states were considering draft regulations or revising their regulations, and 35 states reimbursed or planned to reimburse services in assisted living or board and care facilities as Medicaid-covered services (Mollica, 1998). This includes both Medicaid waiver programs and more aggressive use of payments for Medicaid personal care services (Harrington et al., 1994; Mollica, 1998).
In addition to creating new licensure categories and expanding Medicaid waiver programs, many states began allowing higher levels of care to be provided outside nursing homes. For example, by the mid-1990s, the majority of state licensing agencies allowed ALFs to house residents who were chair-fast because of health problems or who used wheelchairs to get around inside the facility. One-third of the licensing agencies allowed such facilities to retain residents who were bedfast (Hawes, Wildfire & Lux, 1993). Some states also embarked on more aggressive strategies for expanding the potential role of ALFs. These strategies included:
-
permitting the provision of daily or intermittent nursing care (including skilled care) and hospice care in these facilities,
-
allowing retention of residents with greater levels of impairment, and
-
modifying their nurse practice acts (Hawes, et al., 1993; Kane & Wilson, 1993; Manard, Altman, Kane & Zeuschner, 1992; Mollica, 1998; Mollica & Snow, 1996; Newcomer, Lee & Wilson, 1996).
Despite this growth in state policy activity, no consensus has emerged on the appropriate regulatory model for assisted living. Some state policies sought to create assisted living as a unique arrangement, with distinctive environmental features (e.g., requiring that ALFs provide apartments with kitchens). Other states differed on whether regulation should even address the housing component or should be limited to only the service component, in effect treating assisted living as a kind of home health service. Some states allowed ALFs to provide daily nursing care, while others explicitly prohibited such services -- requiring facilities to arrange for the provision of these services through home health agencies. Still other states subsumed assisted living under their traditional board and care home regulations (Mollica, 1998; Mollica & Snow, 1996).
Despite variations in regulations, it is clear that most states intend to encourage the growth of assisted living and other forms of residential care. Indeed, it appears that some states have substituted residential care beds for nursing home beds in their long- term care system (Hawes et al., 1995b). In part, public payors have grown interested because some research has found that housing with supportive services might be a cost-effective alternative to nursing homes (Lawton, 1976; Mor, Sherwood & Gutkin, 1986). For example, one recent study suggested that use of assisted living for patients with Alzheimers disease and other dementias could reduce nursing home utilization and reduce Medicaid costs by an estimated $2,000 per person per month (Leon, Cheng, & Neumann, 1998).
D. Lack of Information on the Assisted Living Industry
In the view of many observers, assisted living represents a promising new model of long-term care that blurs the sharp and invidious distinction between nursing homes and community-based long-term care and reduces the chasm between receiving long-term care in ones own home and in an institution. In addition, ALFs are thought to provide (or be capable of providing) a range of long-term care services that makes them a viable but less institutional alternative to nursing homes (Kane & Wilson, 1993; Mollica & Snow, 1996; Wilson, 1993).
Despite the promise of assisted living, its rapid growth, and expansion of state policy in the area, there is relatively little empirical information about this new sector of the health care system. First, there have been few studies of residential care and practically none of assisted living. Second, previous assisted living studies have been limited to facilities in a single state or a few states. These studies include work in California (Newcomer, Preston & Broderick, 1995; Newcomer, Lee & Wilson, 1997); Oregon (Rosalie Kane, personal communication, 9/1/99); Washington (Susan Hedrick, personal communication, 9/1/99 ) or in a few states, such as Maryland, North Carolina, Georgia, and New Jersey (Philip Sloane & Sheryl Itkin Zimmerman, personal communication, 9/1/99). This is a serious limitation of the previous research. As noted above, there is tremendous variation across states in the way assisted living is defined, in the services ALFs are allowed to provide, and in the residents ALFs may serve. Thus, there is variation across states and communities in the relationship between assisted living and other parts of the health and long-term care systems.
E. The Current Study
This report is the third in a series of planned reports based on data collected from a survey of a national probability sample of ALFs. These data were collected as part of a study, "A National Study of Assisted Living for the Frail Elderly." This study was initiated and funded by the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation (ASPE). Additional support for the project has been provided by AARP, the Administration on Aging (AoA), the National Institute on Aging (NIA), and the Alzheimers Association. Other reports produced during this study include surveys of state licensing agencies (Mollica, 1998; Mollica & Snow, 1996), interviews with developers (Manard & Cameron, 1997); a report on a telephone survey of a national probability sample of ALFs (Hawes, Rose & Phillips, 1999a and 1999b); and a report on a sample of discharged residents (Phillips, Hawes, Spry & Rose, 2000). One more report is forthcoming: a report on the effects of different privacy and service arrangements on such issues as resident satisfaction, aging in place, and affordability.
ASPE has a long-standing interest in the potential for housing with supportive services, including board and care homes and ALFs, to meet the needs of aged and disabled persons for residential long-term care services. As noted earlier, since the early 1980s, ASPE has commissioned a number of studies aimed at increasing both the depth and breadth of the knowledge base for policy-making in this area.
F. Organization of the Report
This report presents information gathered in site visits to a nationally representative sample of 300 ALFs. These are ALFs that provided either a high level of privacy in accommodations or a high level of services or both high services and high privacy. This sample of facilities is a sub-sample of the original sample of all ALFs developed for The National Study of Assisted Living for the Frail Elderly (Iannacchione, Byron, Lux, Wrage & Hawes, 1999). Analysis of information on the entire sample of facilities was presented in an earlier project report (Hawes, Rose & Phillips, 1999). The sample of facilities included in this report is a sub-sample of those ALFs in the original sample that provided a level of privacy or services that the research team considered consistent with the basic philosophy of assisted living.9 Thus, the report provides generalizations only to the 41% of the full sample of ALFs nationwide that met the study criteria for providing high privacy or high service (or both).10
The report provides information on this special group of ALFs in the following structure:
- Section II provides an overview of the study methods,
- Section III presents the information on ALF residents,
- Section IV presents the information on ALF staff,
- Section V presents the results of the walk-through observations in each of the study ALFs,
- Section VI presents information from interviews with the administrators about facility operations, policies, and staffing,
- Section VII provides a policy-focused set of conclusions based on the report findings.
II. STUDY METHODS
This section of the report presents the eligibility criteria used for ALFs included in the overall study, as well as the criteria used to select a subset of ALFs for site visits. This section also describes the criteria and process used to determine whether an ALF provided high services or high privacy or both. Finally, this section describes the process of data collection in interviews with administrators, other staff, residents and, for some, their family members, and through a structured observation of conditions in the facility by project staff. A more detailed description of the study methods in terms of sampling design and data collection may be found in other project reports (Ahlen & Major 1999; Iannacchione et al., 1999).
A. Defining Assisted Living Facilities: Overall Study Eligibility
The National Study of Assisted Living for the Frail Elderly considered residential care facilities eligible for inclusion in the study only if they met certain criteria. In order to be eligible, a facility had to be operating in the United States at the time of the initial sample frame construction in late 1997 and the telephone eligibility screening and data collection (late 1997 and early 1998). To be identified as eligible, an ALF also had to:
1. Serve the elderly
2. Have 11 or more beds; AND
3a. Be a self-proclaimed ALF, that is, a facility that referrred to itself as an ALF or advertised itself as providing assisted living;
OR
3b. Be a residential care facility that, at a minimum, offered (provided or arranged) certain key services, defined as: at least two meals, 24-hour staff, housekeeping, and assistance with at least two of the following: medications, bathing, or dressing.
B. Rationale for Exclusions from Eligibility
The study excluded facilities with fewer than 11 beds for three reasons. First, we expected the majority of these very small facilities to be board and care homes that did not serve the elderly or did not provide the level of care and services commonly associated with assisted living. Previous studies of the board and care industry (Hawes et al., 1995a; Hawes et al., 1995b) indicated that very small facilities were more likely than larger homes to serve a younger population with developmental disabilities or chronic mental illness. They were also much less likely to make a wide array of services available to residents and much less likely to have a nurse on staff. Thus, including small facilities in the sampling frame would have contributed to a large number of ineligible facilities being found during the screening calls. Second, in practice, there were not many places with fewer than 11 beds that referred to themselves as assisted living. For example, in Oregon, which had a specific licensure category called assisted living and which allowed licensure of places with fewer than 10 beds, there were no facilities constructed that were that small. Thus, it seemed unlikely that otherwise eligible facilities would be eliminated simply because of the studys size criterion. Third, including the small homes would have meant basically re-examining many issues that were addressed in an earlier study of the board and care industry (Hawes et al., 1995a) and would, in many ways, have duplicated that effort.
The study also excluded places that did not serve the elderly, places licensed for only special populations (e.g., persons with developmental disabilities), and places licensed only as nursing homes. (Long-term care campuses that housed eligible ALFs and a nursing home or other residential setting was eligible).
C. Data Collection in Eligible Facilities
In order to determine whether a place met our study eligibility criteria, project staff created a list of places believed to be assisted living or similar residential care facilities in 60 geographic areas known as First Stage Sampling Units (FSUs). As noted above, greater detail about this process can be found in the projects sampling report (Iannacchione et al., 1999). A sample of these facilities was selected, and project staff conducted telephone interviews with the administrators. The report on these interviews describes the general nature of the assisted living industry (Hawes, et al., 1999). Some of the information from these telephone interviews was used to identify facilities that were eligible for additional data collection.
D. Identifying Facilities for Site Visits
After interviewing facility administrators in the sample of eligible ALFs, project staff selected a sub-sample of facilities for additional data collection. One group of facilities that met general eligibility criteria did not appear at all consistent with the philosophy of assisted living or with the generally accepted concept of what ALFs offer. These were facilities that, despite what they called themselves, in fact offered minimal services or minimal privacy, as defined below. This group of facilities was excluded from additional data collection. A second group was identified that provided a combination of low services and low privacy, as defined below. A sub-sample of these facilities was targeted for a second telephone interview intended to collect additional information from the administrator about policies, services, and price. A third group of ALFs was targeted for additional data collection that involved on-site, in-person interviews with administrators, staff, and residents, and telephone interviews with family members of very impaired residents. This third group of facilities consisted of a sample of the ALFs that offered high services or high privacy or both high services and high privacy. The criteria that define these groupings are described below.
1. Classifying Facilities by Levels of Privacy and Services
ASPE and the project team decided early in the process of designing the study to conduct site visits to only those facilities that conformed closely to the philosophy of assisted living or, more correctly, to the general consensus about what were key elements of assisted living. To examine the characteristics of these facilities and to make comparisons between different types of facilities, the project team recognized the importance of identifying characteristics of ALFs that were expected to affect their performance. As noted earlier, two major dimensions intended to capture key features of the facilities were the availability of needed services (i.e., to meet scheduled and unscheduled needs and to enable residents to age in place) and resident control over his or her environment. The project team considered privacy of accommodations an important aspect of the environment, and indeed prior research found that residents had strong preferences for privacy (Jenkens, 1997; Kane, Baker, Veazie & Solomon, 1998). Thus, we used the service and privacy dimensions to sort all the facilities that had been surveyed during the first telephone data collection.
The facilities interviewed during the initial telephone survey were divided into the three sub-populations or tiers shown in Exhibit II.1. The level of services and privacy offered by a facility determined its tier membership. During the design phase of the study, we developed working definitions for each of the levels of service and privacy. (The criteria for inclusion in each Tier are described below.) The working definitions were then refined based on the results of the initial facility telephone screening survey and appear below (Hawes et al., 1999; Iannacchione et al., 1999). Only those facilities that met criteria for inclusion in Tier #3 were eligible for site visits that included interviews with residents, administrators and other staff. For any resident who was too impaired to respond to the interview, project staff interviewed a direct staff caregiver and, by telephone, a family member. Thus, only data from Tier #3 facilities were included in this report.
| EXHIBIT II.1: Tier Classification of Survey-Eligible Facilities by Level of Privacy and Level of Source | |||
| Level of Privacy | Level of Service | ||
| High | Low | Minimal | |
| High | Tier#3 | Tier #3 | Tier #1 |
| Low | Tier #3 | Tier #2 | Tier #1 |
| Minimal | Tier #1 | Tier #1 | Tier #1 |
This report concentrates on describing the facilities, staff and residents in this group of ALFs. Relatively little attention is devoted to differences across the three types of facilities in Tier #3 (e.g., high service with low privacy, low service with high privacy, or high service with high privacy). More detailed discussions of the effects of these different privacy and service levels on such factors as resident satisfaction, length of stay, and so on, will appear in subsequent project reports.
2. Defining Levels of Service and Privacy
In the initial telephone screening survey, project staff collected sufficient information about each responding facility to place it in one of three categories or Tiers. The Tier #1 facilities offered minimal privacy or minimal services or both. To be rated as providing minimal privacy, a facility had to have one or more rooms or apartment bedrooms shared by at least three residents. Such an arrangement, referred to as a ward-type bedroom, is considered incompatible with the concept of assisted living -- regardless of the characteristics of a facilitys other units. To be rated as providing minimal services, a facility did not provide what were considered basic services. Those basic services included the following:
- two meals a day;
- housekeeping;
- 24-hour staff oversight;
- assistance with medications and at least one ADL and medications or assistance with two or more ADLs.
Thus, if a facility did not offer all of these basic services it was classified as providing minimal services. As noted above, ALFs classified as offering either minimal privacy or minimal services (i.e., Tier #1 facilities) were deemed ineligible for any further data collection, since they did not meet the studys definition of assisted living. As shown in Exhibit II.2, 32% of the ALFs nationwide fell into this category, even among self-described ALFs.
For ALFs that offered both low services and low privacy, that is, the Tier #2 ALFs, the only additional data collection was a more extensive telephone survey of the administrator. Those data will be reported elsewhere. An ALF was defined as low privacy if it had no bedrooms shared by three or more persons but was a facility in which fewer than 80% of the bedrooms were private. An ALF was classified as low services if it did not have an RN on staff and did not provide nursing care with its own staff but did provide the following:
- 24-hour staff oversight;
- housekeeping;
- at least 2 meals a day;
- personal assistance, defined as help with at least two of the following: medications, bathing, or dressing.
As shown in Exhibit II.2, an estimated 27% of ALF sites nationwide offered both low privacy and services.
| EXHIBIT II.2: Distribution of ALFs by Mix of Services and Privacy | ||||
| High Service | Low Service | Minimal Service | Total for Privacy | |
| High Privacy | 11% | 18% | 2% | 31% |
| Low Privacy | 12% | 27% | 2% | 41% |
| Minimal Privacy | 8% | 20% | 1% | 28% |
| Total for Service | 31% | 65% | 5% | 100% |
| Percentages may not total 100% due to rounding. | ||||
ALFs that reported providing either high services or high privacy or both were included in the Tier #3 sampling strata. These ALFs constituted an estimated 41% of the total supply of ALFs nationwide. A subset of these ALFs was then selected for the on-site, in-person interviews. A high privacy facility was one in which 80-100% of the units were private. A high service ALF provided at least the following:
- 24-hour staff oversight;
- housekeeping;
- at least 2 meals a day;
- personal assistance, defined as help with at least two of the following: medications, bathing, or dressing;
- at least one full-time registered nurse (RN) on staff; and
- nursing care (monitoring or services) with its own staff.
There was some disagreement about whether the last two criteria were essential. For example, one could argue that a facility that will arrange nursing care might also be classified as high service. However, having an RN on staff should improve the ability of the facility to appropriately supervise assistance with medications, monitor the health status of residents, assess changes over time, and supervise and monitor the quality of the services provided or arranged. Certainly, it seems likely that such a facility would be more able to allow residents to age in place and to serve as a viable alternative to nursing home care.11
3. Data Collection in Tier #3 Facilities
Tier #3 facilities offered one of the following combinations of services and privacy: (1) High Service and Low Privacy; (2) Low Service and High Privacy; or (3) High Service and High Privacy. Tier #3 facility administrators were surveyed using the Administrator In-Person Interview and the Administrator Self-Administered Supplemental Questionnaire. Also, project staff conducted a structured observation of the Tier #3 facilities, using the Walk-Through Observation instrument.12 Thus, for these facilities, there is very detailed information about resident case mix, services, prices, admission and discharge policies, visiting hours, other policies related to resident autonomy, administrator background, staff training, facility ownership, and affiliations with multi-facility systems.
In addition, a probability sample of staff and residents of Tier #3 facilities were interviewed on-site, using the Staff Member Interview and the Resident Interview. For members of the resident sample who were moderately or severely cognitively impaired or who were physically unable to participate at the time of the interview, proxy respondents were identified. For each resident requiring a proxy, we used the Resident Proxy Respondent Interview to interview a staff member who provided direct care to the resident. Using the Family Member Telephone Interview, we also interviewed a family member of each resident who required a proxy respondent.13
E. Sampling
This section briefly describes the study sampling approach.
1. Sampling Units
The sampling design for the study was a stratified, three-stage, national probability sample with the following sampling units defined at each stage:
- First-Stage Sampling Units (FSUs): Counties or county equivalents;
- Second-Stage Sampling Units: Geographic addresses within selected FSUs that contain one or more candidate ALFs; and,
- Third-Stage Sampling Units: Residents, their family members, and staff members of selected Tier #3 ALFs.
2. Tier #3 Sub-sample
One of the study objectives was to determine the extent to which ALFs conformed to the philosophy of assisted living. Thus, criteria were used to identify those facilities that most closely approximated the philosophy -- that is, those offering high services or high privacy or both. In order to describe these facilities and to identify any differences in performance associated with variations in facility characteristics, subsequent data collection was conducted among the participating Tier #3 facilities. On-site interviews were conducted with Tier #3 facility administrators, staff members, and residents.14 A total of 705 Tier #3 facilities were identified in the 60 FSUs originally selected for the facility eligibility screening and initial telephone survey. However, limited project resources required that a sub-sample of 40 FSUs be selected from these 60 FSUs for subsequent on-site data collection. The sub-sample of 40 FSUs was selected with equal probabilities using systematic sampling (Kish, 1965). To preserve the geographic spread of the sub-sample, the 60 FSUs were ordered by state prior to selection. A total of 482 Tier #3 facilities were associated with the sub-sample of 40 FSUs and were the ALFs targeted for recruitment to participate in the on-site data collection.
3. Selection of Residents and Staff Members
The administrators of the Tier #3 facilities were recruited by telephone in order to secure permission for a Field Representative (FR) to visit the facility to conduct the various in- person interviews. During this telephone recruitment, the facility administrator was asked how many residents and staff members were currently at the facility. These staff member and resident counts were used to generate sample selection worksheets that the FR used to select which residents and staff members would be interviewed. For the resident samples, six random numbers were selected in each facility. If the number of residents at the facility was less than eight, all residents were selected. Similarly, for the staff members, two random numbers were selected for each facility, but if there were less than four staff members at the facility, all of the staff members were selected.
4. Response Rates
The staff and resident response rates within Tier #3 facilities were quite high. Ninety-three percent of the selected staff members responded. Information was gathered for 88% of the residents selected for interviews (from in-person interviews with residents or their proxy respondent). However, only 62% (i.e., 300) of the 482 eligible facilities participated in the full on-site data collection. This rate is lower than the 74% rate achieved in the earlier Board and Care study (Hawes et al., 1996). However, the assisted living industry is in a greater state of flux than the board and care industry, and a lower rate of participation might be expected because of that turmoil. In addition, to be counted, a facility had to participate in all aspects of the data collection (i.e., have completed interviews with administrators, staff and residents and the walk-through observation). Further, most surveys of ALFs have had difficulty obtaining good response rates, and most have had participation rates that were lower (e.g., ALFA, 1998; Gulyas, 1997; Hodlewsky, 1998). Finally, with statistical adjustments for non- response, we can develop meaningful national estimates with these data. The 300 ALFs included in this analysis represented the estimated 4,693 ALFs across the nation that offered high services or a high privacy environment or both high services and high privacy.
F. Analytic Strategy
This report focuses on providing descriptive information about residents in assisted living, ALF staff and administrators, and the policies and environments within these facilities. The reported statistics will, in the main, be comprised of means and proportions and their standard errors. All results reported were produced using SUDAAN, a statistical software package expressly designed to provide appropriate estimates of variance and standard errors for data derived from multi-stage samples (Shah, Barnwell & Bieler, 1997). A number of tables including a relatively large number of variables are presented in this report. In many instances, different numbers of individuals responded to the various items reflected in the tables. For these tables, the reported N is the largest number of respondents for a single item in the table. The numbers in parentheses beside the reported means or proportions within the tables and in the text are the standard errors associated with these population estimates.
Throughout the presentation of these data it is important to remember that the estimates apply to only about two-fifths (41%) of the places that identified themselves as an ALF or provided a comparable level of services in a residential long-term care setting. These were the ALFs that provided the higher levels of service or privacy that the research team deemed most consistent with the general philosophy underlying the assisted living movement.
III. RESIDENTS IN ASSISTED LIVING FACILITIES OFFERING HIGH SERVICE OR HIGH PRIVACY
This section of the report describes the characteristics of residents in the 41% of ALFs that offer high services or high privacy or both high privacy and high services. Thus, this group of residents does not represent all the residents in all ALFs nationwide but only those in this special group of ALFs. This sample of residents represents nearly 200,000 elderly residents in high service or high privacy ALFs.
A. Demographic Characteristics
As Exhibit III.1 indicates, individuals residing in high service or high privacy ALFs were, like most elderly persons in long-term care, overwhelmingly white, widowed females. Only 12% were still married. They were also quite elderly. The average resident in the high service/high privacy ALFs was 84.5 years old. More than 96% (0.90) were over 65 years of age, and 54% (1.79) were aged 85 or older. By comparison, 49% of U.S. nursing home residents were 85 and over (Krauss & Altman, 1998). About three-quarters (76%) of ALF residents in the high service/high privacy facilities had one or more living children, and most (86%) had a relative within a one-hour drive of the facility. The vast majority (91%) reported being visited by friends or relatives within the last month, and more than one-third (36%) reported receiving visitors either daily or more than once a week. They were, on the whole, a relatively well- educated group. More than 40% had at least some college education, and more than 20% were college graduates. Of those residents who provided information on their annual income (i.e., only 47% of the residents interviewed), 70% reported incomes between $9,000 and $50,000; more than half of the residents reported incomes greater than $14,000 per year.
| EXHIBIT III.1: ALF Resident CharacteristicsN=184,558 | |
| Characteristic | Prevalence % (std. error) |
| Female | 78.6 (1.11) |
| Marital Status | |
| Married | 12.1 (1.00) |
| Widowed | 70.8 (1.64) |
| Divorced/separated | 7.2 (0.70) |
| Never married | 9.9 (1.23) |
| White | 98.7 (0.55) |
| Living Children | 75.8 (1.51) |
| Relatives Within Hour Drive | 85.9 (1.90) |
| Age | |
| Under 75 | 10.9 (1.21) |
| 75-84 | 34.8 (1.12) |
| 85+ | 54.3 (1.79) |
| Friends/Relatives Visit--Last 30 Days | |
| None | 9.3 (1.28) |
| Once or twice | 26.7 (1.44) |
| Once a week | 27.6 (2.04) |
| More than once a week, not daily | 30.1 (2.29) |
| Daily | 6.3 (0.91) |
| Education | |
| Not a high school graduate | 26.8 (2.23) |
| High school graduate | 28.4 (1.69) |
| Some college | 24.6 (1.96) |
| College graduate | 20.3 (1.80) |
| Income (47.3% reporting) | |
| Less than $5,000 | 11.6 (1.84) |
| $5,000 to $8,999 | 12.7 (2.19) |
| $9,000 to $13,999 | 23.7 (2.04) |
| $14,000 to $24,999 | 23.0 (1.63) |
| $25,000 to $50,000 | 23.1 (2.66) |
| Over $50,000 | 5.9 (1.10) |
B. Entry Into Facilities and Length of Stay
Seventy percent of current ALF residents resided in their own home or apartment prior to moving to the ALF in which they were interviewed. As one might expect, most residents (73%) received help in making the decision to move from their previous residence into an ALF, as Exhibit III.2 indicates. In the vast majority of cases (91%), the other participants in the decision were family members. Only 18% of the time was a physician involved in the decision. What was more surprising, only about half (52%) of the residents who received help in making the decision indicated that they had complete or almost complete control over the decision. One-quarter (25%) indicated that they had little or no control over the decision or choice of ALF. As discussed in the section on conclusions, this fact has significant implications for facilities perceptions of who the consumer is and potentially for how their services are marketed.
| EXHIBIT III.2: Entry into an ALFN=192,046 | |
| Characteristic | Prevalence % (std. error) |
| Residence Prior to ALF | |
| Own home/apartment | 70.2 (1.95) |
| Relative's home | 8.8 (1.00) |
| Nursing home | 4.2 (0.73) |
| Subacute care | 2.2 (0.42) |
| Supportive housing | 12.5 (1.47) |
| Other | 2.1 (0.55) |
| Received Help with Decision | 72.9 (1.65) |
| Who Helped (multiple response) | |
| Family | 90.5 (1.31) |
| Physician | 17.7 (2.62) |
| Other | 16.1 (2.92) |
| Amount of Control Over Decision | |
| Complete/almost complete | 52.2 (4.67) |
| Some control | 23.0 (2.54) |
| Little or no control | 24.9 (3.33) |
| Length of Stay | |
| Less than one year | 37.5 (2.19) |
| One to three years | 43.1 (1.78) |
| Over three years | 19.4 (1.44) |
At the time of the survey, the average resident had lived in the study facility for just over two and one-half years. Thirty-eight percent of residents had been in the facility for less than one year; 43% had been in the facility for between one and three years; and 19% had been in the facility for more than three years. When reviewing these figures, it is important to remember that these data come from a cross-sectional survey, not a prospective study that followed people from entry to departure. This means that longer-stay residents were somewhat over-represented in the study, and the estimated average length of stay was somewhat higher than one would find in a prospective study of an admission cohort.
Prior Living Situation. For a significant proportion of assisted living residents, their current ALF residence was not their first experience with supportive housing. Within the five years prior to the survey, 6% of the residents had been in a nursing home (4%) or subacute care facility (2%), while 13% had been in some other type of residential facility or other housing setting with supportive services. These current ALF residents left their previous setting for a variety of reasons. Many needed more care than was available (40%); some preferred a location closer to family and friends (22%); others became acutely ill and required hospitalization and did not return to their previous setting after the hospitalization (11%). Slightly more than one in four of these residents (27%) reported dissatisfaction with quality of care or some other aspect of facility operations as part of the reason for their departure.
C. Health and Functional Status
1. Cognitive Status
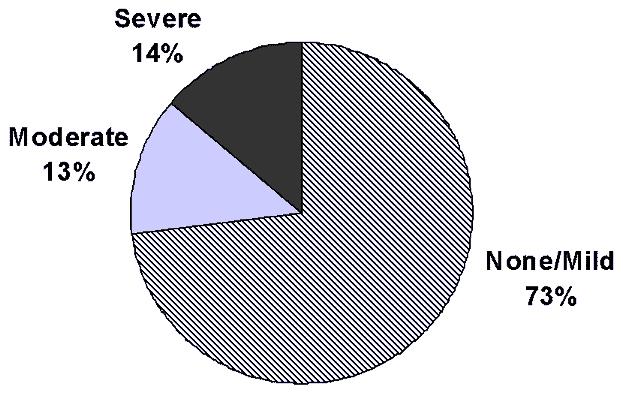
One of the major determinants of an individuals need for assistance or supervision is his or her cognitive status. In the ALFs classified as providing high service or high privacy, almost three-quarters (73%) of the residents were cognitively intact or had only mild symptoms of cognitive impairment, as displayed in Exhibit III.3. Thirteen percent of the residents exhibited moderate cognitive impairment, while 14% had severe cognitive impairment. Thus, more than one-quarter of assisted living residents (27%) exhibited symptoms of moderate to severe cognitive impairment.15
| EXHIBIT III.3: Cognitive Impairment of Residents in High Privacy or High Service ALFs |
 |
The analyses also revealed some differences in the distribution of resident characteristics and care needs across the three types of ALFs. The high privacy facilities, with both high and low services, served residents for whom the distribution of cognitive impairment was similar to the distribution of the population as a whole. However, the ALFs classified as low privacy and high service served a resident population with significantly higher levels of cognitive impairment than one would expect, given the distribution in the resident population as a whole. As Exhibit III.4 indicates, almost 36% of the residents in the high service/low privacy facilities had moderate or severe cognitive impairment, in comparison to 23-25% in other types of ALFs.
| EXHIBIT III.4: Cognitive Impairment and Type of ALF*N=179,721 | |||
| Cognitive Impairment | Type of ALF | ||
| Low Privacy, High Service | High Privacy, Low Service | High Privacy, High Service | |
| None, Mild | 64.1% | 76.9% | 75.1% |
| Moderate | 16.1% | 11.5% | 11.9% |
| Severe | 19.8% | 11.6% | 13.0% |
| * Significant differences among the facility types were determined using logistic regression and comparisons with the overall population values. The probability was less than .05 that the low privacy, high services facilities had the same proportion of individuals with moderate or severe cognitive impairment as the population. | |||
These results indicate that residents in assisted living, even in facilities with high levels of service or privacy, were much less likely to be cognitively impaired than were residents in nursing homes, where one sees moderate to severe impairment in 60-70% of residents (Krauss & Altman, 1998). The results also suggest that residents in assisted living were less likely to be cognitively impaired than residents in more traditional board and care facilities. Prior research on residents in board and care facilities in ten states found over 40% of residents had moderate to severe cognitive impairment (Hawes et al., 1995a, 1995b & 1995c).
2. Physical Function
Both cognitive impairment and physical ailments affect an individuals physical functioning. Exhibit III.5 provides information on the functional problems experienced by residents in ALFs offering high privacy or high services. The analysis focused on five activities of daily living (ADLs): dressing, locomotion, transfer, toilet use, and eating.16 As one would expect, it was in dressing, an early-loss ADL, that one found the highest levels of functional limitations, with nearly one-fifth of the residents (19%) receiving some type of assistance or supervision from another person. For mid-loss ADLs (locomotion, transfer, toilet use), between 8% and 9% of residents received supervision or physical assistance. For the ADL in which function is usually lost latest in the process of decline (eating), only 3% of residents received supervision or assistance. When one looks at ADL function in the aggregate, 79% of residents were independent. Thirteen percent received help with one or two ADLs, while just over 8% received help with three to five ADLs.
While residents in assisted living make relatively light use of staff assistance, they made considerable use of assistive devices to compensate for functional limitations. In the week prior to the interview, at least one-fifth of the residents used a cane (27%) or wheelchair (21%) to assist them with locomotion, while slightly more than two-fifths (44%) used a walker. One-third (32%) of residents had some urinary incontinence during that same seven-day period. Residents and proxy respondents reported even higher levels of assistance in instrumental activities of daily living (IADLs). For example, about three-quarters (77%) of residents received assistance in managing medications.17
| EXHIBIT III.5: Physical FunctionN=192,046 | |
| Type of Activity | Prevalence % (std. error) |
| Supervision or "Hands-on" Help Provided In | |
| Dressing | 19.3 (2.08) |
| Locomotion | 7.5 (1.22) |
| Transfer | 8.9 (1.57) |
| Toilet use | 9.0 (1.52) |
| Eating | 3.4 (0.92) |
| Supervision of Physical Assistance in ADLs | |
| None | 79.2 (2.17) |
| One or two | 12.7 (1.32) |
| Three to five | 8.1 (1.53) |
| Use of Assistive Devices | |
| Hearing aid | 21.8 (1.53) |
| Wheelchair | 20.6 (1.71) |
| Walker | 43.7 (2.03) |
| Cane | 27.0 (1.68) |
| Incontinent of Urine | 31.7 (1.65) |
| Received Help with Medications | 76.7 (2.12) |
| Needed More Help with | |
| Dressing | 12.0 (2.89) |
| Locomotion | 11.5 (3.29) |
| Toileting | 26.1 (2.07) |
| Eating | 0.0 (0.0) |
These levels of impairment in physical functioning are much lower than those found among nursing home residents, where nearly three-quarters of the residents received help with three or more ADLs (Krauss & Altman, 1998). They were roughly similar to the levels observed in board and care homes, where about 12% of the residents received hands-on assistance with three of more ADLs (Hawes et al., 1995b and 1995c). Further, the levels directly reported by residents and their proxy respondents were lower than the estimates provided by the administrators about their overall resident case mix. In those interviews, administrators estimated that nearly one-quarter (24%) of their residents had received hands-on assistance with three or more ADLs during the preceding seven days.18
| EXHIBIT III.6: Physical HealthN=192,046 | |
| Characteristic | Prevalence % (std. error) |
| Self-Reported Health | |
| Excellent | 7.1 (1.02) |
| Very good | 19.1 (2.28) |
| Good | 34.6 (1.41) |
| Fair | 29.3 (1.85) |
| Poor | 9.9 (.098) |
| Health Service Use (last 12 months) | |
| Hospital | 32.3 (2.30) |
| Emergency room | 24.2 (1.87) |
| Health Events | |
| Stroke | 5.6 (0.69) |
| Heart attack | 2.6 (0.53) |
| Hip fracture | 3.2 (0.53) |
| Fall | 37.0 (1.77) |
| Pain Interferes with Activities | |
| All of the time | 6.1 (0.67) |
| Some of the time | 18.5 (1.52) |
| Little of the time | 16.9 (1.35) |
| None of the time | 58.5 (2.27) |
Additional bivariate analyses indicated that there were no significant differences across the three facility types in the proportion of residents needing ADL assistance. The low privacy/high service facilities did serve a population with a somewhat higher proportion of individuals who needed help with two or more ADLs; however the difference was not statistically significant.
D. Unmet Needs
The residents were also asked about unmet care needs. The questions about assistance with ADLs asked about help provided, not help needed. Thus, the data on ADL assistance received could have under-represented residents actual needs. To address this, at least partially, residents who received some assistance were asked whether they needed more assistance than they received (e.g., needed or wanted more assistance, had to wait inordinately long for needed help). None had unmet needs for assistance in eating, but some residents reported needing more help with dressing (12%) and locomotion (walking or using a wheelchair) (12%). Further, slightly more than one-quarter (26%) of residents who were receiving some assistance with toilet use reported they had unmet needs for assistance in toileting. It is important to note that these unmet need questions were asked only of the residents who were able to respond for themselves.
For residents who were too physically or cognitively impaired to respond, a family member specified by the resident or one identified by the facility as the primary health care decision-maker was interviewed. When asked how much of the time their relative received the help he or she needed with bathing and dressing, the vast majority (75%) of family members interviewed responded that they received such help always. Fourteen percent reported the resident usually received the help needed, while nearly 12% of the family members reported that their relative received needed help only sometimes or never. The responses were similar for a question about whether family members received needed help with eating.
E. Health Conditions and Service Use
While the residents in ALFs with high services or high privacy received relatively little assistance in their ADLs, many did indicate some type of health problems or condition, as shown in Exhibit III.6. Most residents (60%) reported having good to excellent health; however slightly less than two-fifths of residents reported their health as only fair (29%) or poor (10%). These self-reported health rates were relatively similar to those of residents in board and care homes (Hawes et al., 1995c).
Residents also reported health conditions with the potential to limit physical functioning. For example, more than one-third of the residents (37%) also reported a fall in the last year, and one quarter (25%) of the residents reported that pain interfered with their normal activities some or all of the time during the preceding month.
Hospitalization was also relatively common. Residents reported a relatively high rate of use of hospital care. One-quarter (24%) of residents indicated that they had visited an emergency room in the 12 months prior to the interview, and almost one-third (32%) had an overnight stay in a hospital distinct from any emergency room visit. Again, these results are similar to the utilization rates observed among board and care home residents (Hawes et al., 1995b and 1995c). However, ALF residents had higher rates of hospital use than the general elderly population (i.e., only 18% had an inpatient hospital stay) and than nursing home residents (i.e., at 26%) (Krauss, Machlin & Kass, 1999; Krauss & Altman, 1998; Phillips, Hawes, Green & Norton, 1998).
Bivariate analyses indicated that the distribution of residents who had been hospitalized in the previous year in the three different types of high service or high privacy ALFs did not differ significantly from the distribution in the population as a whole. However, residents in ALFs offering the combination of high privacy and low service did have somewhat higher hospitalization rates than the whole population (i.e., 37% v. 32%), although the difference was not statistically significant.19
F. Resident Experiences and Ratings of Facility Performance
This section of the report addresses ALF residents attitudes and perceptions of the environment in which they lived. Literature in the area of patient and client satisfaction with health care suggests the importance of securing information from patients or residents about their experience (Cleary & McNeil, 1988). At the same time, studies have frequently noted an aquiescent response bias or a tendency of persons receiving services to provide positive responses when asked about their satisfaction with the services (Meister & Boyle, 1996; Pascoe, 1983). In an attempt to address this, both residents and family members were asked about their experiences as well as their ratings of various aspects of facility performance in key areas. Again, the data reported here are from interviews with residents and relatives of residents in ALFs that were classified as providing either high services or high privacy (or both high services and high privacy).
1. Ratings of ALF Staffing
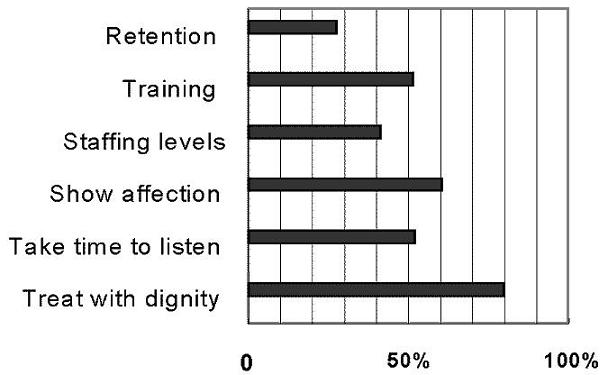
In focus group interviews, ALF residents and family members of ALF residents with dementia consistently identified staffing issues as a major component of quality (Hawes, Greene, Wood & Woodsong, 1996; Greene, Hawes, Wood & Woodsong, 1998; Hawes and Greene, 1998). Thus, residents in high privacy or high service ALFs were asked for their views on the level of staffing, staff retention, and the manner in which staff interacted with them. Exhibit III.7 displays the proportion of resident responses that were in the most positive category (e.g., staff always treat me with respect) for the various queries about staffing in the facility in which they lived. As shown, nearly all (79%) of the residents indicated that staff always treated them with dignity and respect. Almost two-thirds of residents (61%) indicated that staff was always affectionate and caring in their interactions with them.
In other areas, resident responses were more mixed. Just over half of the residents (52%) indicated that staff always took the time to stop and listen to them, and the same proportion (52%) reported feeling that staff training and supervision were very good. The most significant areas in which resident ratings were low were in the areas of staffing levels and staff turnover. Only 42% of the residents responded that adequate numbers of staff were always available, and just over one-quarter (28%) indicated that the facility was very successful in retaining good staff. Families had similar reactions. Only 48% of family members interviewed felt there were always enough staff on duty to adequately care for all the residents.
| EXHIBIT III.7: Positive Resident Ratings of Staffing |
 |
2. Activities
An important aspect of the assisted living environment is the type and quantity of activities offered to residents. As Exhibit III.8 shows, 45% of residents indicated that they were involved in activities all of the time or most of the time. However, 49% reported being involved in activities only some of the time. Most of this activity, however, was confined to the premises of the ALF in which the resident lived. Slightly more than one-third (35%) of the residents indicated that they had not been involved in an activity outside the facility in the two weeks preceding the interview. Slightly more than another third of the residents (36%) indicated that they had been involved in an activity outside the facility only once or twice during the preceding 14 days.
One reason residents may have reported relatively few activities outside the facility was that most residents reported that the ALFs in which they lived offered limited transportation to activities they enjoyed. More than half of the residents (55%) reported that transportation to activities that they enjoyed was either never available or only sometimes available. Forty-six percent of family members reported that the ALF never or only sometimes offered transportation to activities their relative enjoyed.
In addition, about half (49%) of the residents indicated that the facility never or only sometimes offered activities that they enjoyed. Family members were also skeptical about the activities program, with 36% reporting that the facility never or only sometimes offered activities the resident enjoyed and in which he/she could participate.
These results are not too surprising when one notes that only 41% of residents and 56% of family members indicated that staff usually or always asked about the residents activity preferences.
| EXHIBIT III.8: ActivitiesN=192,046 | |
| Resident Attitudes | Prevalence % (std. error) |
| Involvement in Activities | |
| None of the time | 6.1 (1.00) |
| Some of the time | 48.7 (2.15) |
| Most of the time | 35.1 (1.62) |
| All of the time | 10.0 (1.46) |
| Activity Outside Facility (14 days) | |
| Never | 35.4 (1.63) |
| Once or twice | 36.1 (1.79) |
| Three to five times | 20.6 (1.25) |
| Every day or every other day | 7.9 (0.77) |
| Offer Activities You Enjoy | |
| Never | 8.5 (1.14) |
| Sometimes | 40.5 (3.27) |
| Usually | 31.4 (2.17) |
| Always | 19.6 (2.35) |
| Transportation for Things You Enjoy | |
| Never | 19.3 (2.73) |
| Sometimes | 34.7 (3.34) |
| Usually | 26.1 (2.41) |
| Always | 19.9 (2.83) |
| Staff Ask About Activity Preferences | |
| Never | 22.9 (3.19) |
| Sometimes | 36.1 (3.71) |
| Usually | 26.1 (2.19) |
| Always | 14.9 (2.35) |
3. Living Arrangements and Meals
Living arrangements are also considered a key aspect of assisted living, with their emphasis on creating a non-institutional environment. In particular, prior studies found that residents have strong opinions about and preferences for private accommodations, both for their sleeping place and bathroom (Jenkens, 1997; Kane et al., 1998).
Accommodation Type. In the ALFs offering high privacy or high services (or both), the accommodations of the residents were almost evenly split between apartment and bedroom units, as shown in Exhibit III.9. For residents living in apartments, the most common arrangement (58%) was a one-bedroom apartment, with only 6% of the residents having a two-bedroom apartment. However, about one-third (34%) of the residents living in an apartment had a studio apartment.
Privacy. Private accommodations were common in the ALFs that offered either high privacy or high service or both. Eighty-one percent of the residents lived alone. Some residents shared their space with a relative, but among the one-fifth (19%) of residents who lived with someone, almost 70% shared their living space with a person unrelated to them by marriage or blood.
| EXHIBIT III.9: Living Arrangement and MealsN=188,064 | |
| Characteristic | Prevalence % (std. error) |
| Living Situation | |
| Apartment | 50.8 (4.67) |
| Bedroom only | 49.2 (4.67) |
| Type of Apartment | |
| Studio | 34.4 (4.78) |
| One bedroom | 57.6 (4.77) |
| Two bedroom | 6.1 (1.27) |
| Other | 1.9 (0.87) |
| Share Living Space with Another | 18.5 (2.40) |
| Full Bath Attached to Room/Apt. | 76.9 (2.93) |
| Attached bathroom is shared | 17.0 (2.63) |
| Other Shared Bathroom | 23.0 (2.67) |
| Able to Arrange Furniture as Wishes | 94.5 (2.11) |
| Individual Temperature Control | 83.9 (2.63) |
| Able to Lock Door for Room/Apt. | 83.2 (3.12) |
| Available in Room /Apartment | |
| Separate kitchen space | 35.6 (5.13) |
| Refrigerator | 53.7 (3.94) |
| Something to heat food | 36.4 (4.53) |
| Call button in bedroom | 81.5 (2.71) |
| Seat in shower or tub | 65.1 (3.46) |
| Railing in shower or tub | 77.5 (3.08) |
| Railing beside toilet | 80.5 (2.70) |
| Call button in bathroom | 77.7 (2.50) |
| Choice Among Entrees | |
| Never | 19.5 (4.29) |
| Sometimes | 12.8 (2.52) |
| Usually | 13.6 (2.29) |
| Always | 54.1 (5.49) |
| Food is Tasty & Well-Seasoned | |
| Never | 5.2 (1.01) |
| Sometimes | 28.8 (2.03) |
| Usually | 40.3 (2.62) |
| Always | 25.7 (1.83) |
As noted, private bathrooms were considered a key aspect of privacy, according to most residents. Three-quarters (77%) of the residents in these high privacy or high service ALFs had a full bath attached to their unit (apartment or bedroom). Fewer than one-fifth (17%) of these residents shared the bathroom attached to their unit, and nearly all those residents (95%) shared that attached bath with only one other person. For the 23% of residents who did not have a full bathroom attached to their apartment or bedroom, some did have a private half-bath attached to their unit; however, all of these residents shared at least bathing rooms for taking a shower or bath. Taken together with the residents who shared a full bathroom, this means that slightly more than one- third (35%) of all the residents in high privacy or high service ALFs shared all or part of a bathroom.
Amenities. The residents reported that their rooms or apartments were equipped with various amenities and safety devices. Safety devices, such as call buttons in bedrooms (82%) and bathrooms (77%) and railing in the shower/tub (78%) or beside the toilet (81%), were fairly common. However, even in the ALFs that offered high privacy or high services, kitchens were rare. Only about one-third (36%) of the residents reported having a kitchen or place to heat food. Moreover, only slightly more than half the residents (54%) had a refrigerator in their room or apartment.
Meals. Residents were also asked a number of questions about the meals and food service at the facility. Slightly more than half (54%) of the residents reported that they always had a choice among entrees, but 20% indicated that they never had such a choice. Only 26% of residents found the food was always tasty and well-seasoned, but another 40% indicated that the food was usually tasty. However, one-third (34%) of the residents provided poor ratings of the food, responding that the food was never or only sometimes tasty and well-seasoned. Families, perhaps having less direct information, gave somewhat more positive responses than residents. Only 21% of the families reported that the food was never or only sometimes things their relatives liked and could eat, and only 17% felt the food was never or only sometimes tasty and well-seasoned.
4. Nursing Care, Purchased Services, Charges, and Aging in Place
During the interviews, 12% of the assisted living residents (1.19) in ALFs that provided high privacy or high services reported that they had needed temporary nursing care or monitoring since moving into the ALF in which they currently lived.20 As displayed in Exhibit III.10, the most common way in which that nursing care was provided was with facility nursing staff (45%; 5.56). In an additional 14% (4.03) of the cases, the facility helped the resident or family make arrangements for nursing care through a home health agency. In just over one-fifth of the instances (22%; 4.59) the resident or the residents family arranged for a home health nurse. In roughly 10% of the cases, the facility requested that the residents go to a hospital or nursing home until they recovered to the degree that they did not need nursing services or monitoring, even if the anticipated need was only temporary (i.e., 14 days in duration). As might be expected, nursing services were not typically included in the basic monthly rate charged by the high privacy and high service ALFs.
Nursing services were not the only type of needed services that were either excluded from the package of services provided by the ALF or not part of the basic charge. In some cases, the services were offered for an additional fee. According to the reports of the residents, the service most residents purchased at a cost over and above the basic monthly rate was personal grooming services, such as shampooing and styling hair. Sixty-one percent (2.78) of residents purchased these services. Almost 20% purchased incontinence supplies (3.16); 11% (1.95) purchased additional transportation services; 16% (1.97) purchased personal laundry services; and 26% (2.58) purchased foot care (e.g., cutting toenails).
| EXHIBIT III.10: Resident Report on Arrangements When Temporary Nursing Care was Needed |
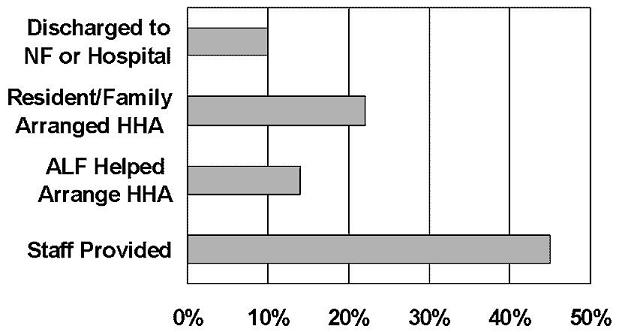 |
Queries concerning residents perceptions of the cost of care indicated that only two-thirds (67%; 2.56) of the residents who responded (excluding those with proxy respondents) were aware of the size of monthly bills or charges from the facility. Of those, just over two-thirds (68%; 3.21) indicated that the bills were about what they expected them to be; however, nearly one-third (29%; 2.91) of the remaining residents who were aware of the bills indicated that the charges were higher than they had expected. A similar proportion of family members (24%) reported that the monthly charges were higher than they had expected, while two-thirds (68%) responded that the charges were about what they expected.
One of the central philosophical tenets of assisted living is that ALFs will enable residents to age in place. However, resident and family knowledge about the conditions under which the resident could no longer be cared for in the facility was mixed. Less than one-third of the residents in the study (30%; 6.44) reported being informed of their facilitys discharge policies. Thus, almost 70% were uninformed about the conditions under which they might be discharged from the facility. Families reported feeling they were better informed, although 32% of the families reported that they either did not know whether the facility had policies about discharge (17%) or that the facility had no such policies (15%). Further, among those two-thirds (69%) of family members 15% felt that the policies were either very unclear or somewhat unclear, while 28% felt that the policies were only clear enough to provide a general idea of when the facility would discharge a resident.
Despite this, residents and families had substantial confidence that the resident would be able to stay in the ALF, aging in place. Residents were almost unanimous (98.2%; 0.48) in their expectation that they would be able to reside in their present ALF for as long at they wished. Essentially the same was true for family members, 89% of whom expected that their relative would be able to stay at the AFL as long as they wanted the relative to stay.
G. SUMMARY
The residents in the ALFs with high levels of privacy or service were largely white, widowed females, who were quite elderly. They were both relatively well-educated and relatively affluent. Most of them entered assisted living from their own home or apartment, making the decision to enter assisted living with the assistance of their families. However, almost one-quarter of residents indicated that they had little or no control over the decision to enter a facility.
Over one-quarter of the residents suffered from moderate or severe cognitive impairment, and roughly one-fifth of the residents received assistance in some ADL activity. The overwhelming majority, however, received help with their medications, and many used assistive devices, especially to assist with locomotion. Roughly two-fifths of residents considered themselves in only fair or poor health, and, in the year prior to the survey, they used inpatient services at rates much higher than the general population.
Residents were relatively satisfied with the respect that facility staff showed them in interactions. They were somewhat less sanguine about the affection staff showed and their willingness to listen, although the majority still felt that staff were always affectionate and had the time and willingness to listen to them. Their greatest points of concern about staff concerned the adequacy of staffing levels and staff retention by the facility, with fewer than half the residents reporting that the ALF in which they lived always had sufficient staff and were able to retain staff. Similarly, residents were not overwhelmingly positive about activities in ALFs. Residents split almost evenly on their perceptions of the ready availability of activities they enjoyed and on the availability of transportation to events and activities they would enjoy. One of the more unexpected findings was that almost three-fifths of residents indicated that staff never or only sometimes asked them about their activity preferences.
Assisted living residents in these types of ALFs were almost equally likely to be found with a full apartment as with only a bedroom. The majority did not share their living space, but those who did usually shared with an unrelated individual. When they needed temporary nursing care, they were most likely to receive it from the facility staff, although about one-third of the residents who needed such care had to make the arrangements themselves or were temporarily discharged to a hospital or nursing home to receive nursing care. Finally, although few residents had clear knowledge of facility discharge policies, almost all expected to stay in the facility for as long as they wished.
IV. STAFF WORKING IN HIGH PRIVACY AND HIGH SERVICE ASSISTED LIVING FACILITIES
The sample of staff in ALFs with high levels of service or privacy was drawn from only those staff who supervised or engaged in direct care of residents. A total of 569 staff members were interviewed. They included personal care assistants, nurses, resident care directors, administrators and others involved in providing or supervising resident care. The weighted staff sample provides estimates for the characteristics, knowledge, behavior, and attitudes of over 30,000 individuals involved in personal care in those ALFs that offered either high privacy or high services (or a combination of high services and high privacy).
A. Staff Characteristics and Training
Information on staff sociodemographic characteristics and work experience is presented in Exhibit IV.1. As those results indicate, the vast majority of staff members who provided or supervised personal care in ALFs were overwhelmingly female (97%), and two-thirds (68%) were white. One-fifth (20%) were licensed health care professionals of some type (i.e., RN, LPN, licensed social worker, some type of therapist). The majority of the staff members interviewed (51%) were nursing or resident care assistants, and 15% were medication technicians. One-quarter (25%) of the staff interviewed had some other designation, such as resident care coordinator, administrator, clerical staff or housekeeping staff. Eighty-five percent of the respondents had completed high school and just over one-third (35%) had at least some college. Three-quarters of the staff had previous experience in some type of setting that provided personal care. It is also interesting to note that significant numbers of the staff (39%) worked part time; only 61% worked full-time. Finally, half the staff had been employed in the facility for two or more years.
The types of training and orientation required for these staff varied across facilities, but for the most part, relatively little training was required. Of the unlicensed personnel, three-quarters (75%; 4.00) were required to attend some kind of pre-service training or orientation. For those who were required to take training, the most common amount of required training was between one and 16 hours of training. Further, only 11% (1.69) of the staff who took required training completed it prior to the start of work. Instead, they received on-the-job training or a combination of pre-service and on-the-job training. By comparison, aides in nursing homes are required to have a minimum of 75 hours of training (10 days) and to pass an exam before they can work on a unit providing direct resident care.
| EXHIBIT IV.1: Staff CharacteristicsN=30,384 | |
| Characteristic | Prevalence % (std. error) |
| Female | 96.5 (0.90) |
| Race/Ethnicity | |
| White | 68.1 (4.30) |
| African American | 23.6 (3.78) |
| Asian/Pacific Islander | 4.1 (1.19) |
| Other | 4.2 (1.00) |
| Education | |
| Did not complete high school | 15.4 (2.35) |
| High school graduate or GED | 32.5 (2.60) |
| Trade or vocational school | 17.4 (2.92) |
| Some college | 34.7 (3.19) |
| Previous Personal/Nursing Care Experience | 75.0 (2.63) |
| Worked in Facility for 2 or More Years | 52.2 (2.98) |
| Full-Time Staff | 60.9 (2.40) |
| Types of Staff | |
| Licensed professionals | 19.5 (2.65) |
| Resident/nursing assistant | 51.4 (2.86) |
| Medication technician | 14.9 (3.56) |
| Other | 25.2 (3.30) |
The content of the training usually covered the gamut of topics one would expect in such curriculum. The topics included:
- first aid (79%, 2.81);
- how to provide personal care (92%, 1.71);
- information about Alzheimers Disease (80%, 2.83);
- information about dealing with challenging behaviors (83%, 2.49);
- residents rights (96%, 1.62); and
- medication management (67%, 3.90)
The staff also reported that they received training on or orientation to the philosophy of assisted living and how that philosophy differs from traditional care in nursing homes or other residential settings. In addition, three-quarters of the staff (75%, 3.24) had participated in continuing education activities, including those at the facility, during the 12 months prior to their interview.
B. Staff Activities and Tasks
One of the personnel practices that nursing homes have begun to use to enhance their efficiency is cross-training staff. Staff members are trained so that they can perform multiple roles in the organization (Rudder & Phillips, 1998). While some nursing homes use this strategy, it appeared to be the rule, rather than the exception, in ALFs that offered high privacy or high services. More than that, staff responses suggested that in ALFs staff had regular responsibilities for carrying out more than one task.
| EXHIBIT IV.2: Staff DutiesN=30,080 | |
| Duties | Prevalence % (std. error) |
| Provide Personal Care | 91.3 (1.77) |
| Assist with Activities | 76.9 (2.77) |
| Medication Assistance or Supervision | 76.1 (2.45) |
| Serving Meals | 69.6 (3.13) |
| Laundry | 60.0 (4.10) |
| Housekeeping | 53.0 (3.53) |
| Travel Outside Facility | 42.6 (3.97) |
| Clerical Work | 32.8 (4.33) |
| Administrative/Supervisory Duties | 30.0 (3.11) |
| Cooking | 16.7 (3.26) |
| Maintenance, Repairs, Yard Work | 8.0 (1.81) |
As Exhibit IV.2 illustrates, the norm among the sampled ALFs was for staff to have more than one duty or responsibility. Given the nature of the staff sample, which was limited to only those individuals providing or supervising the provision of personal care, it is no surprise that the duty with the highest prevalence rate was providing personal care (e.g., help with bathing or dressing). The next two most common duties, which three-quarters of the staff reported as part of their job description, were assisting with activities (77%) and providing assistance or supervision with the administration of medications (76%). The majority of the staff interviewed also assisted with the serving of meals (70%), while 60% helped with the laundry and more than half (53%) did some housekeeping. Clerical and administrative or supervisory tasks were regular duties for one-third (33%) of care staff. It seems that only cooking, maintenance work, and landscaping were tasks that were relatively specialized. It is important to note that this multiplicity of task responsibilities makes calculating staffing levels for direct care staff much more complex.
C. Staff Knowledge of Aging and Care
1. Understanding Normal Aging
Most staff who provided or supervised direct resident care reported receiving some type of orientation and training or were licensed healthcare professionals. Despite this, most staff members were not knowledgeable about what constituted normal aging. When asked about a variety of conditions that occur with some frequency among the elderly as a result of some illness but which are not a normal part of aging, a significant majority of the staff mistakenly attributed these symptoms to the process of aging. As Exhibit IV.3 demonstrates, almost 88% (1.42) of staff believed that memory loss and confusion were a normal part of aging. Almost four in five staff (80%; 2.53) believed that urinary incontinence was a normal part of aging. A similar proportion (78%) of the staff felt that depression was normal for the elderly. Three out of five staff (63%; 3.04) even felt that being quarrelsome or frequently angry was simply normal aging. Only 8% (1.34) of direct care and supervisory staff appropriately indicated that none of these symptoms was a part of normal aging. This lack of knowledge bodes poorly for early recognition and treatment of relatively common conditions among the elderly that can often be resolved with treatment (e.g., depression). The result could well be unnecessary decline and loss of functional independence among ALF residents. The only encouraging finding in this regard is that most staff did recommend contacting a physician when a resident had new onset of incontinence, as discussed below.
| EXHIBIT IV.3: Staff Views of What is a Normal Part of Aging |
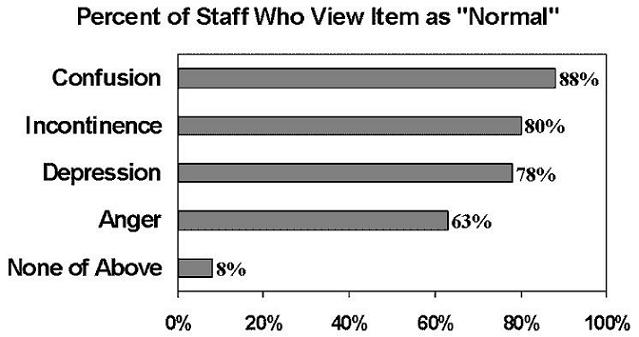 |
2. Understanding Medication Administration and Side-Effects
The provision of assistance with medications is one of the main tasks of ALF staff. As noted earlier, roughly three-quarters (77%) of ALF residents who lived in high service or high privacy ALFs received assistance with their medications, and slightly more than three-quarters of the staff who were interviewed (77%; 2.87) passed medications or otherwise helped residents with the self-administration of medication. The research team was unable to include a comprehensive set of questions on medication administration and drug side-effects because of the focus of the study and resource constraints; however, three items related to medication issues were included in the study.
Close to half of the staff members who were involved in medication administration answered all three questions about medications correctly. More than two-thirds (71%; 4.54) of the staff knew that the pulse of someone taking digoxin or lanoxin should be monitored, while about one-third (29%) did not answer correctly. Similarly, 74% (5.35) of staff administering medications indicated that they would use a metric or apothecary measure to prepare a medication calling for a 20ml dose. The responses were less informed about the potential side effects of powerful antipysychotics. Fewer than half of the staff members (48%; 6.04) were able to identify the correct set of negative side effects from a list of symptoms that should be noted and reported to the residents physician or supervisory staff at the facility.21 One-fifth (21%; 4.85) of the staff involved in medication administration reported having no idea what symptoms should be reported when these psychotropic medications were used.
These results were troubling, since the vast majority of ALF residents received assistance with medications and an equally large proportion of staff helped with medication administration. Moreover, other studies have found that, on average, persons in residential care facilities are taking more daily medications than residents of nursing homes (McGuire, 2000).22 Finally, a recent report by the U.S. General Accounting Office (1999) found that medication errors were among the most common quality problems in ALFs. Monitoring the effects of these medications, as well as providing residents with the proper medication at the proper dose and time, is a major responsibility of the assisted living industry. These results, though limited in scope, suggested that some ALF staff members were inadequately prepared for this serious task.
3. Responding Appropriately to Care Situations
Staff members were also asked about how they would handle situations described in several care vignettes. Each vignette provided information about a relatively common problem in caregiving and offered a series of potential responses. In some instances, staff members were asked to identify the single best answer. In other instances, the questions allowed for multiple responses (e.g., choose all that apply). Across these vignettes, staff exhibited considerable variability in the degree to which they were aware of the best response to the presenting problem.
The greatest consistency in responses occurred in the vignette that described a resident presenting with hives who had just started taking a new antibiotic a day earlier. Almost all of the staff (95%; 1.12) indicated that the first thing to be done was to contact, or have a supervisor contact, the residents physician. Staff also did quite well with a scenario involving the recent onset of urinary incontinence. Just over 90% (1.44) indicated that a physicians appointment was needed. However, 15% (1.93) also thought it a good idea to have the resident cut back on the amount of liquids taken between meals, a strategy that is inappropriate and could lead to worse problems, such as dehydration.
Another vignette asked staff how they would respond to a resident with memory loss who was repetitively asking for his wife, who died last year. The options offered in the question were to take the resident:
- to a quiet area, explain the wifes death, and comfort him; or
- to an on-going activity he enjoys and try distracting him.
Unfortunately, as displayed in Exhibit IV.4, more than three-fifths (63%; 3.35) of the staff indicated that they believed that the appropriate response was to reorient the resident to the reality of his wifes death. This response is particularly striking in the context of staff reports on training. Most staff reported that they received training or were licensed health professionals, and 80% who reported receipt of training said they received information about Alzheimers Disease and behavior management. Despite this, many staff did not know the approach that was considered the most appropriate way to address residents with cognitive impairment who had forgotten life events or were not oriented to the staffs perception of time and place.
| EXHIBIT IV.4: Staff Opinion of How to Manage Resident with Memory Loss |
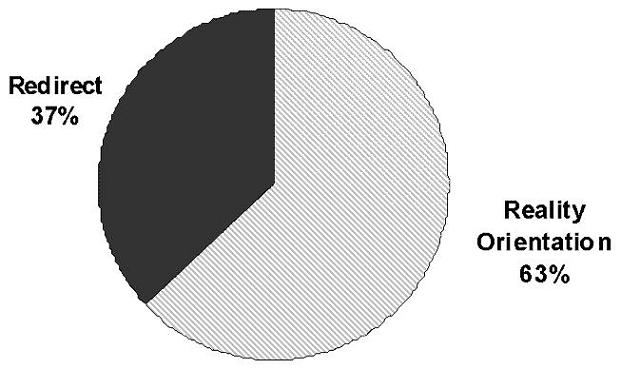 |
When staff were asked how they dealt with individuals who presented with difficult or disturbing behaviors, the vast majority of staff indicated appropriately that they discussed the problem with their supervisor, other staff, or the residents family. However, other less common practices were more troublesome. More than one-quarter of the staff (29%; 3.14) indicated that they would medicate the resident, and 11% (2.17) indicated that they would isolate the resident. One percent of the staff (0.47) responded that they would physically restrain or discipline the resident.
Staff responded more appropriately when asked how they would respond to a specific behavioral manifestation. Staff members were asked about how they would address a resident who resisted bathing and were given a variety of appropriate options from which to choose. One woefully inappropriate option was offered.
Gently but firmly make it clear that it is time for her bath. If she continues to resist, get another staff member to help you get the resident to the bathing room since allowing her to get her way will only make the problem worse next time.
Only 14% (2.08) of the staff selected this response as an option.
The importance of the staffs knowledge, or lack of knowledge, of normal aging was reinforced by their responses to a vignette involving a relatively sudden onset of confusion in a resident who was cognitively intact just a week earlier. More than three- quarters of the staff (76%; 2.23) indicated that a call to his physician was the best action to take. However, other staff selected inappropriate responses. Nearly one in ten staff (9%; 1.59) indicated that nothing should be done because that is "just what happens when one gets old. A slightly larger number of staff (14%; 2.01) thought it best to talk to the resident about staying active and trying harder to remember names.
Unfortunately, onset of confusion and memory loss can be associated with a wide variety of serious illnesses and conditions, including delirium, infection, stroke, dehydration, malnutrition, and adverse drug reactions. These conditions are often treatable. However, if treatable causes are not addressed in an appropriate manner, their potential sequelae are not only functional decline but also death. Thus, failure of one-quarter of the staff to recognize the sudden onset of confusion as a serious symptom that warrants investigation by a physician could place residents at risk of poor health outcomes and avoidable functional decline.
Staff responses to another vignette addressing issues of resident independence were also quite revealing. Over 85% (1.69) of the staff indicated that they had received training or orientation on the philosophy of assisted living and how it differed from traditional care. Of course, one of the major tenets of assisted living is assisting residents in maintaining their physical independence and control over their environment (Assisted Living Quality Coalition, 1998). The following, quite detailed scenario was offered to staff.
Mrs. Greene has arthritis and some short-term memory and judgment problems. She likes to dress herself, but she is slow and has difficulty with some activities. She also sometimes selects clothes that dont match. Thus, it might take her 20 minutes to get dressed by herself, and she might end up wearing a red plaid blouse with a pink and purple print skirt.
The options offered to the staff were to:
-
Choose her clothes and do all dressing activities for her that she finds difficult.
-
Let her choose her own clothing, as long as it was appropriate for the weather and activity, and do all the dressing activities for her that she finds difficult.
-
Let her choose her own clothing, as long as it was appropriate for the weather and activity, and let her dress herself, even if she is slow.
The last of these options is the one that conforms most closely to the ideal of helping residents maintain their independence in physical functioning, and two-thirds (67%; 2.94) of the staff chose that response. However, one-third of the staff members selected one of the other options that reflected practices less likely to help maintain independent function. In part, this approach may be attributable to the customer focus found in many facilities in which doing tasks "for" the resident was considered the appropriate approach.
D. Staff Satisfaction
All sampled staff members in the high service or high privacy ALFs were asked a number of questions about their job responsibilities and their attitudes or views about their job and their supervisors. Each item was scored on a five-level response scale ranging from strongly disagree to strongly agree. However, the variability in responses across the items may be more helpful in understanding staff attitudes than the absolute response levels for each item.23
For example, 75% of staff either agreed or strongly agreed with the statement that I am not asked to do excessive amounts of work. However, only 45% indicated that they agreed with the statement that my pay is good. In general, staff in the study facilities were considerably more satisfied with their workloads than with their salaries, as can be seen in Exhibit IV.5.24
As shown, a fairly high level of agreement (i.e., between 70% and 79%) was observed for items dealing with job security, workload, staffing levels (i.e., enough help), training, and the ability to provide input into management decisions. The items that received the highest levels of agreement (i.e., >70%) encompassed issues related to whether staff felt positively about their management and supervision. Those issues included whether staff felt they had sufficient time to get their work done, whether they had the needed equipment and training to get their job done, and whether staff felt they had flexibility in how they did their job. Staff members also felt they had job security.
| EXHIBIT IV.5: Staff SatisfactionN=30,384 | |
| Issues | Percent Agree or Strongly Agree % (std. error) |
| My Supervisor is Competent | 87.6 (1.78) |
| Have Opportunities to Learn Job Better | 84.9 (2.07) |
| Responsibilities are Clearly Defined | 85.5 (1.78) |
| Job Security is Good | 78.8 (2.72) |
| Enough Help and Equipment to do Job | 78.7 (3.08) |
| Enough Time to Get Work Done | 76.6 (2.05) |
| Reasonable Workload | 74.3 (2.40) |
| A Lot of Freedom in How I Do My Job | 72.9 (2.31) |
| Staff Receive Enough Training | 72.3 (2.11) |
| People Listen to My Suggestions | 72.1 (2.04) |
| Enough Time to Talk to Residents | 66.2 (2.80) |
| No Conflicting Demands Made | 65.5 (1.97) |
| Fringe Benefits are Good | 59.2 (2.72) |
| Few Hassles to Deal With at Work | 53.8 (2.70) |
| My Pay is Good | 44.7 (3.17) |
| Good Advancement Opportunities | 30.1 (2.33) |
| Personal Care Schedule is Paramount | 71.1 (1.63) |
Staff expressed somewhat lower levels of agreement with positive statements about having sufficient time to talk with residents, facing no conflicting demands, the adequacy of fringe benefits, and having few hassles at work, but a majority of staff (i.e., between 54% and 66%) agreed or strongly agreed with such statements.
The areas in which staff expressed the most significant dissatisfaction were with their salaries and their opportunities for advancement. Fifty-five percent of staff disagreed or strongly disagreed with the statement that their wages were adequate, and 70% did not agree with the statement that they had good opportunities for advancement.
Staff members were also asked whether getting personal care tasks done on schedule was the most important priority for direct care staff. Nearly three-quarters (71%) of staff agreed or strongly agreed with this statement. Thus, it seems that the body work or a task orientation and its scheduling may dominate direct care staffs conception of their role. While the philosophy of assisted living may emphasize a social model in contrast to this task-oriented approach, many direct care staff members seem to have received the message that keeping up with the schedule of personal care is the real heart of their duties.
E. Salaries and Workload of Aides/Assistants
Personal care assistants (PCAs) are the most numerous staff in all long-term care settings, providing the vast majority of personal care and assistance to residents. Thus, they play a key role in determining the quality of care in residential care settings, like ALFs. As reported earlier, half (51%) the staff respondents were PCAs in the direct care staff sample in high privacy or high service ALFs. Because of the key role they play, this section of the report examines only their responses to items on the interview about their workload and salaries.
Two basic elements affecting a PCAs workload are the number of residents to whom he or she is assigned and whether the PCA has a permanent or floating assignment.25 Many observers, including staff in nursing homes and ALFs, argue that a reasonable staff-to-resident ratio and permanent assignment of aides to a specific group of residents are essential elements of a social model of care, one of the key tenets of the philosophy of assisted living (Hawes, 2000). In keeping with this philosophy, in the high service or high privacy ALFs, almost two-thirds (64%; 3.53) of the PCAs indicated that they were usually assigned to the same group of residents, while the remaining one-third had different resident assignments on a daily or weekly basis.
| EXHIBIT IV.6: Wages of Personal Care Assistants in High Privacy or High Service ALFs |
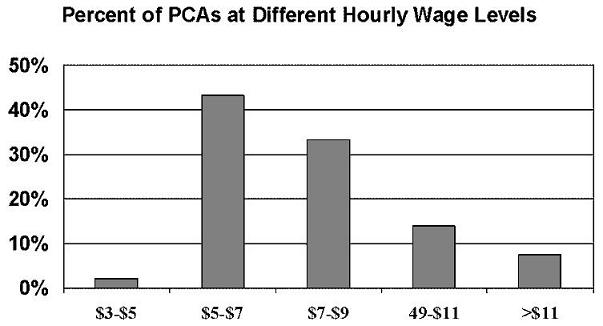 |
The number of residents to whom PCAs were assigned varied considerably. The modal, or most common response, was ten residents per PCA; however, the median number of residents per PCA was 14. This difference reflects the fact that one-quarter of the PCAs had more than 23 residents for whom they were responsible. These staffing levels must be considered together with the fact that most staff reported having multiple responsibilities (e.g., personal care, activities, laundry, and meal service).
The salary distribution for PCAs in high privacy or high service ALFs appears in Exhibit IV.6. The most common response, which was reported by more than two-fifths of the respondents (43%; 3.85), was that they earned between $5.01 and $7.00 per hour at the time of the interview in the fall of 1998. One-third (33%; 2.70) earned between $7.01 and $9.00. Thus, more than three-quarters of PCAs made between $5.00 and $9.00 per hour. Fourteen percent of the PCAs (2.59) made between $9.01 and $11.00.
F. Summary and Conclusions
This section of the report presented data from the survey of staff who provided or supervised personal care in ALFs with high levels of privacy or service. The findings from the staff responses are clearly mixed, particularly with respect to staff knowledge. First, the majority of unlicensed staff received some type of training or orientation. However, the requirement was usually for only a few days of training, and the training typically did not have to be completed prior to the start of work with residents. Second, in terms of knowledge, in many instances, the vast majority of staff members were aware of the proper response to specific situations, such as onset of incontinence, and to care needs, such as the appropriate response to signs of an adverse reaction to an antibiotic. Despite this, a significant number of staff members were ill-informed about dealing with the onset of new problems (e.g., confusion), some medication issues (e.g., signs of adverse reactions to neuroleptic medications), and issues related to the care of individuals with dementia. Third, the staff was almost completely unaware of what constituted normal aging and what signs and symptoms warranted referral for evaluation and treatment. Since several factors are expected to contribute to rising acuity levels in assisted living, poor training and knowledge in these areas may become more troublesome and risky over time, both for providers and residents. Finally, the perception of a significant majority of staff (71%) was that completing tasks on schedule was the most important priority for direct care staff, despite the incompatibility of this view with the philosophy of assisted living and a social model of care.
The staff in our sampled ALFs reported relatively low levels of dissatisfaction with their working conditions; however, they did have some concerns. Both their pay levels, which most commonly ranged from between five and seven dollars per hour for personal care staff, and their perception of the small possibility of advancement were the areas in which they reported the greatest dissatisfaction.
Most direct care staff did not perceive their workload as overly heavy, and the median number of residents for whom personal care assistants cared was fourteen. On the other hand, PCAs in ALFs also often did a variety of tasks, such as housekeeping, laundry, meal service, in addition to providing personal assistance to residents. Further, a significant proportion of all direct care staff (i.e., 44%) reported that they did not have sufficient time to talk with and listen to residents. Thus, the staffing ratios in those facilities that provided either high privacy or high services (or both) raise serious questions about the ability of many ALFs to care for residents with more significant care needs. For example, many experts believe the ratio of personal care staff to residents in nursing homes should be between 1:5 and 1:8 in a setting in which aides are not generally responsible for other tasks (Harrington, et al., 2000). Thus, it is unclear whether ALFs with ratios of 1:14 would be able to facilitate aging in place and adequately care for residents with the heavier care needs that aging-in-place would entail.
V. RESULTS OF THE WALK-THROUGH OBSERVATIONS IN HIGH PRIVACY OR HIGH SERVICE ALFs
As part of the site visit to the sampled high service or high privacy ALFs, the project staff assigned to conduct the interviews with administrators, staff and residents also performed a structured walk-through observation of the environment in the facilities.26 During the course of the structured observation, they evaluated the ALFs exterior, community areas, dining facilities, and other aspects of its physical plant and environment.
A. Safety and Supportive Features in High Privacy or High Service ALFs
Four items explicitly related to safety were a part of the walk-through instrument. Two of these items concerned fire safety and two items were related to supportive devices intended to help residents maintain independent function and reduce the risk of falls. Smoke detectors were universally used in ALFs (99.8%; 0.18), and fire sprinkler systems were almost equally ubiquitous (i.e., present in 92% of the ALFs; 1.67). There was a somewhat lower level of availability of supportive devices. Seventy-eight percent (3.34) of the facilities had handrails in the halls, but only 48% (5.88) of the facilities had ample lighting in the hallways. Ample lighting required that the entire area be brightly illuminated with no glare. Another 45% of the ALFs (5.07) had good lighting in their hallways, which indicated some glare or some areas with too little lighting. The same pattern held true for lighting in common or community areas such as dining rooms, community living rooms, and activity rooms. Half of the facilities (51%; 5.91) had ample lighting in community areas, while 45% (5.14) had only good lighting.
B. Community Rooms and Dining Areas
One important aspect of the environment and communal spaces in ALFs was whether they facilitated residents ability to make choices among various activities. Thus, part of the structured observation addressed the resources available in those spaces and the sorts of activities that could be carried out there. The most common social and recreational aid or resource available in these areas was a television set (98%; 0.73). Card or game tables were also almost universally available (92%; 2.29). Almost three-quarters of the community areas (74%; 4.51) had a radio, phonograph, cassette player, or some similar device for playing music. Slightly fewer of the community areas (69%; 5.43) had writing tables available. The majority of these spaces (61%; 4.71) had large window areas that contributed to an open feeling. Further, the observers nearly always (93%; 2.42) rated the furniture in these common areas as being either in good condition or like new, and most observers (70%; 4.08) rated the cleanliness of the community rooms as outstanding.
The field observers also reported that the common indoor spaces seemed to be used relatively heavily by the ALF residents. Exhibit V.1 displays the levels of use for these areas during a late morning period, based on project staff observations and counts. In only 8% of the facilities were these areas unused at the time of the walk-through. In just over two-fifths (41%) of the high privacy or high service ALFs, the community rooms were being used by fewer than one-third of the residents. In just over half (51%) of the facilities, these areas were being used by more than one-third of the residents during the observations.
| EXHIBIT V.1: Resident Use of Communal Spaces in ALFs |
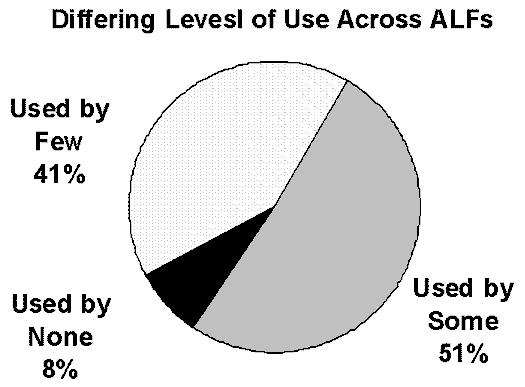 |
Almost all the high privacy or high service ALFs (96%; 1.70) had communal dining areas in which the furniture was either like new or good. The majority (56%; 5.13) of these community dining rooms had good window space that contributed to an open feeling, and the observers rated the cleanliness of almost three-quarters of the dining areas (73%; 3.66) as outstanding. However, in two-fifths of the high privacy or high service facilities (40%; 3.72), there was no community room in which residents could prepare and serve a meal to friends or relatives.
C. Outdoor Areas in High Privacy or High Service ALFs
As Exhibit V.2 demonstrates, there was considerable consistency in the general features of the outdoor areas of ALFs. Nearly all of these ALFs (>97%) could be entered without using steps or stairs. In essentially all the high privacy or high service ALFs, there was an outdoor area for residents use, and chairs were available for sitting outside. Nearly all the ALFs (94%) also had an area for walking, and the walkways were wide enough to accommodate ambulatory aids like wheelchairs and walkers. Three-quarters (75%) of the ALFs had benches or chairs along the walkway. Although observations were made during later summer and early fall, observers found that availability of a barbecue grill was less common, available in less than half (46%) of the high privacy or high service ALFs. When queried about the overall attractiveness of the outdoor communal areas, almost one-half of the project observers (48%) classified the outside area as very attractive, while another two-fifths (42%) indicated that the outdoor area was only average in its attractiveness.
| EXHIBIT V.2: Facility Outdoor AreaN=4,390 | |
| Characteristic | Prevalence % (std. error) |
| Can Enter Without Use of Steps | 97.0 (0.99) |
| Outside Area Available | 97.1 (1.63) |
| Chairs Available in Outside Area | 97.6 (1.12) |
| Tables Available in Outside Area | 75.1 (4.40) |
| Barbecue Grill Available | 46.3 (3.94) |
| Area for Walking | 93.7 (1.61) |
| Benches or Chairs Along Walkways | 74.9 (4.09) |
| Walkways Wide Enough | 95.7 (1.54) |
| How Attractive is the Area | |
| Very unattractive | 4.5 (1.88) |
| Below average | 5.8 (3.11) |
| Average | 42.2 (4.55) |
| Very attractive | 47.5 (4.82) |
The general impressions the project staff observers reached about the environment in the study ALFs were very positive. One of the hallmarks of the assisted living philosophy is that the facilities offer a long-term care setting that is homelike and lacks the bland uniformity and institutional style that so often characterizes other residential long-term care settings. As Exhibit V.3 indicates, most ALFs seem to have been relatively successful in addressing this issue. Over one-third (37%) of the high privacy or high service ALFs were classified as very homelike, while an additional two-fifths (41%) were seen as moderately homelike. Further, the vast majority of observers (92%) rated most of the ALFs as pleasant or very pleasant. At the same time, there was less variation in resident rooms and communal areas than one would expect. Observers reported that there was distinct variation among resident rooms in only two- fifths (40%) of the facilities and that the communal spaces were very distinctive in about the same proportion (38%) of the high privacy or high service ALFs. Finally, slightly more than one in five of the high privacy or high service ALFs (23%) were viewed as being only somewhat homelike or not at all homelike.
| EXHIBIT V.3: General ImpressionsN=4,338 | |
| Characteristic | Prevalence % (std. error) |
| How Homelike is the Facility? | |
| Not at all homelike | 5.3 (1.64) |
| Somewhat homelike | 17.2 (2.86) |
| Moderately homelike | 40.8 (3.47) |
| Very homelike | 36.7 (4.37) |
| Degree of Variation in Resident Rooms | |
| No variation | 0.7 (0.38) |
| Little variation | 19.1 (2.99) |
| Moderate variation | 39.9 (3.83) |
| Distinct variation | 40.3 (5.13) |
| Distinctiveness of Communal Spaces | |
| Little distinctiveness | 4.6 (1.68) |
| Some distinctiveness | 14.1 (2.52) |
| Moderate distinctiveness | 43.9 (3.89) |
| Very distinctive | 37.5 (4.08) |
| How Pleasant is Facility Overall | |
| Distinctly unpleasant | 2.7 (1.18) |
| Somewhat unpleasant | 5.2 (1.48) |
| Pleasant | 35.3 (4.55) |
| Very pleasant | 56.8 (4.82) |
D. The Neighborhood and Exterior Appearance of the ALFs
Most ALFs (49%) were located in suburban areas. Only 15% were found in urban areas. Twenty-two percent were situated in small towns, while 11% of the high privacy or high service ALFs were located in relatively rural areas. In terms of neighborhood, more than two-thirds (70%) of these ALFs were located in an area of either single family homes (35%) or an area that combined residential and business settings (35%). Another 14% were located in an area that mixed single family homes and low-rise apartments. The remaining 16% of ALFs were located in a mix of neighborhood types, such as busy commercial areas or areas without any nearby neighbors.
The most common type of high privacy or high service ALF was a single-story building (46%). Another two-fifths of the ALFs were low-rise buildings of two or three stories in height. Only 13% of the ALFs could be described as similar to a high-rise apartment building with four or more stories. The structured observations about the appearance of the ALFs, however, were more mixed. The most common description, representing nearly two-fifths (38%) of the facilities was that they resembled architecturally attractive square or rectangular apartment buildings, while an additional 18% resembled a cross between a large private home and an attractive apartment building. Only 8% of the ALFs were described as resembling a family home. Fourteen percent were described as looking institutional, like a traditional old-style nursing home. The remaining facilities resembled either an architecturally plain apartment building (9%) or a converted motel or hotel (6%).
Regardless of the style of the building, most (65%) of the ALFs were described as having a very attractive exterior and very nicely landscaped yard. Another 31% were rated as average, which meant that they had a well-maintained exterior and generally attractive yard. Only 5% were rated as below average or very unattractive.
E. Summary of Walk-Through Observations
All of the observers judgements about the physical plant in ALFs indicated that these settings were, by-and-large, well-maintained and clean, with key safety and supportive devices, attractive indoor and outdoor communal spaces, and key recreational or social amenities. There was a mixed review of the high privacy or high service ALFs in terms of the degree of variation in both individual resident spaces and also in communal spaces. However, the structured observations revealed a fairly uniform view of the facilities as pleasant or very pleasant places, that is a facility in which the field interviewer would be comfortable having a relative live.
VI. FACILITIES, ADMINISTRATORS, AND POLICIES
As part of the site visit to each of the sampled high privacy or high service ALFs, interviews were conducted with ALF administrators about their background and experience and about the ALF, including questions about ownership, staffing, policies, and services. The administrator was also asked to complete a questionnaire containing some supplemental questions about the facility and its staffing. The focus of this section of the report is on the information that the administrators provided on these topics.
This chapter reports the responses from the national probability sample of 296 administrators that represents the national population of 4,383 administrators and ALFs that offered high levels of privacy or service. Thus, the sample of ALFs discussed in this section excludes facilities that offered low services and low privacy or minimal services or privacy.27
A. Ownership and Operations in High Service and High Privacy ALFs
As shown in Exhibit VI.1, about half (49%) of the sampled high privacy or high service ALFs operated as for-profit enterprises, and one-half (50%) were not-for-profit operations. Less than 1% of the facilities were operated as joint ventures between for- profit and not-for-profit entities. By comparison, nearly three-quarters of all nursing homes were operated as for-profit enterprises (Krauss et al., 1997).
As shown in Exhibit VI.2, several other features of the operation of these ALFs are interesting. First, almost one-fifth (17%) of the ALFs were operated under a management contract rather than being administered by the owner or his/her direct employee. Many of these management companies operated in several states and provided these services to multiple facilities. Second, the vast majority (79%) of the owners of the high service or high privacy ALFs were involved in other types of supportive housing and residential long-term care settings. For example, half of the ALF owners (49%) also owned one or more nursing homes.
| EXHIBIT VI.1: ALF Ownership |
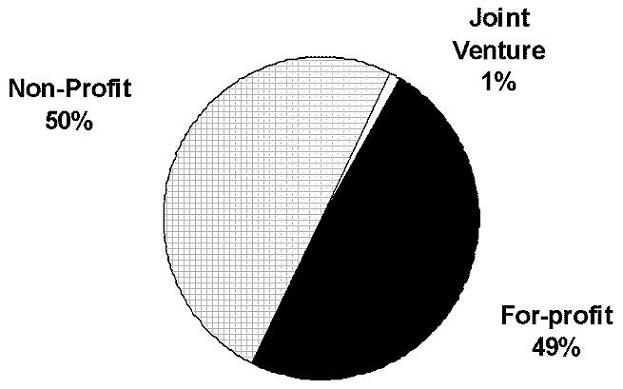 |
| EXHIBIT VI.2: Facility Ownership and AffiliationN=3,654 | |
| Characteristic | Percent of Facilities % (std. error) |
| Ownership | |
| For-profit | 49.2 (4.90) |
| Not-for-profit | 50.2 (2.93) |
| Joint venture | 0.5 (0.35) |
| Operated Under Management Contract | 17.4 (3.97) |
| Involved in Other Supportive Housing | 78.8 (9.67) |
| Own or Operate Nursing Homes | 49.2 (3.21) |
| Facility Part of ALF Chain | 46.4 (3.74) |
Almost one-half of the high service or high privacy ALFs (46%) were part of a multi-facility system or chain of ALFs. This is comparable to the best estimates about nursing home ownership which indicate that slightly over one-half of all nursing homes were part of multi-facility systems (Krauss et al., 1997). For-profit ALFs were significantly more likely to be part of a multi-facility system, with more than half (57%;5.83) being part of a chain or multi-facility system, compared to only 37% (5.07) of the not-for-profit ALFs. Not-for-profit ALFs, however, were more likely to be part of a multi-level campus or system that also operated nursing homes.28 Nearly two-thirds of the not-for-profit ALFs (64%;4.64) were on a multi-level campus with a nursing home, compared to only about one-third (35%;6.00) of the for-profit ALFs. Not-for-profits were also somewhat more likely to be operated under management contracts than were for- profit ALFs (22%; 4.82 vs. 12%; 3.82).
B. Facility Policies and Resident Autonomy
The prevalence of a variety of ALF policies on issues thought to be related to the choices and autonomy available to residents appears in Exhibit VI.3. Almost all high privacy or high service ALFs (99%) allowed residents to bring their personal furniture. Further, of those ALFs that allowed residents to bring personal furniture, the vast majority (90%) allowed residents to furnish their entire apartment with personal furniture. All ALFs (100%) also allowed visitors every day, and most (94%) did not set any restrictions on the visiting hours.
On other issues related to policies on resident autonomy and choice, ALF policies were somewhat more restrictive. For example, only two in five facilities (43%) allowed residents to bring pets and just over one-third (35%) kept facility pets. In those facilities that allowed pets, fish and birds were the most universally accepted pets. ALFs that allowed residents to bring either a cat or dog were somewhat less common. Only two of five (41%) ALFs permitted residents to keep a dog. Since only 43% allowed any pets, this meant that a total of only one in five (18%) of the high privacy or high service ALFs permitted residents to have a dog. Similarly, only slightly more than one- quarter (27%) permitted a cat. In addition, as one might expect in facilities that averaged 50 or more beds, the vast majority of high privacy or high service ALFs had a set meal schedule. The most common times for breakfast were from 8:00 to 9:00, with lunch from 12:00 to 1:00 and dinner from 5:00 to 6:00.
| EXHIBIT VI.3: Facility Policies and Resident AutonomyN=3,654 | |
| Policy | Percent of Facilities % (std. error) |
| Residents Can Bring Personal Furniture | 99.4 (0.38) |
| Residnets Can Furnis Entire Room/Apt. | 90.0 (2.58) |
| Residents Can Bring a Pet | 43.4 (3.13) |
| Of Facilities Allowing Pets, Those Allowing | |
| Dogs | 40.5 (7.40) |
| Cats | 61.9 (6.81) |
| Fish | 79.5 (5.62) |
| Birds | 71.0 (7.03) |
| Facility Keeps Pets or Animals | 34.9 (3.34) |
| Visitors are Allowed Every Day | 99.7 (0.27) |
| Visitors Can Visit at Any Time | 94.1 (1.95) |
| Set Meal Schedule | 97.4 (1.17) |
C. Resident Case Mix in High Privacy or High Service ALFs
An earlier section provided a description of the ALF population, based on a national probability sample of residents, and one of the previous project reports presented data on the entire universe of eligible ALFs (Hawes, Rose & Phillips, 1999). These earlier discussions, however, did not report on the distribution of various types of residents across different types of ALFs except in terms of administrators estimates of their residents overall ADL functioning and cognitive status. Moreover, the data collected directly from residents can be generalized to the ALF resident population nationwide, but the samples are not sufficient to estimate the resident case mix in any individual facility. This section of the report provides more extensive data from the administrators on their overall resident case mix and compares it to that found in nursing homes.
ALFs were relatively homogeneous in their mix of residents when one focused on the administrators reports of the proportion of their residents who received assistance with medications and basic ADLs during the seven days preceding the interview. Assistance with medications was the only area in which most ALF administrators (84%) reported that staff assisted more than half of the residents with their medications. (Indeed, as noted earlier, an estimated three-quarters (77%) of the residents reported receiving help with medications.)
Aside from help with medications, however, most ALF administrators reported a resident case mix that was relatively unimpaired. The vast majority of ALF administrators reported that fewer than half of their residents received help with eating or toileting. Less than 1% of administrators estimated that half or more of their residents needed help with eating, and only 16% of the administrators estimated that at least half the residents received help with using the toilet or with continence care. Similarly, only 12% of administrators reported having a majority of residents who needed assistance in locomotion. These results imply that there was some reasonable measure of homogeneity among resident populations in ALFs, and that most facilities did not have a population with heavy ADL care needs. This is a fairly striking comparison with nursing homes in which the majority of long-stay residents in all facilities have serious functional limitations and receive assistance with locomotion (67%), using the toilet (80%), and eating (60%) (Krauss and Altman, 1998).
While the administrators estimated that most of their residents were independent in these later loss and heavier care ADLs, some administrators did report that the majority of their residents (i.e., more than half of their residents) had relatively heavy care needs. Administrators estimates suggested that between 12% and 16% of ALFs had a significantly higher concentration of residents with heavier care needs.
D. Resident Turnover, Length of Stay, and Admission and Discharge Policies
The administrators of the high privacy or high service facilities included in the site visits reported a median turnover of nine residents in the six months prior to the site visit. Since the median facility population size was approximately 44 residents, there was a minimum turnover rate of nearly 21% in a six-month period. This would equal an estimated annual turnover rate of 41%. Thus, one would expect a facilitys resident population to turn over completely in approximately two and one-half years. This means that in a 44-bed facility one would expect to see an average of 44 new admissions over a two and one-half year period.29
| EXHIBIT VI.4: Facility Admission Policy*N=4,154 | |
| Will Admit If Applicant... | Percent of Facilities % (std. error) |
| Is Incontinent but Manages Own Supplies | 93.0 (1.44) |
| Uses a Wheelchair | 80.1 (2.99) |
| Is Incontinent and Can't Manage Supplies | 57.9 (4.25) |
| Needs Transfer Assistance | 52.3 (4.37) |
| Has Severe Memory or Judgment Problem | 50.0 (4.18) |
| Had Recent Psychiatric Hospitalization | 47.4 (3.66) |
| Wanders | 31.8 (3.52) |
| Resists Nursing or ADL Assistance | 27.3 (3.21) |
| Has Periodic Screaming Episodes | 15.8 (3.30) |
| Is Chairfast | 13.2 (2.17) |
| Is Verbally Abusive | 12.6 (3.19) |
| Engages in Socially Inappropriate Behavior | 12.6 (2.47) |
| Is Physically Aggressive | 3.2 (1.51) |
| Is Bedfast | 2.8 (1.06) |
| * The proportion of administrators who responded "yes" to the question about whether they would admit a resident was nearly the same as the responses for whether they would retain a resident with the given condition. | |
The retention and admission policies of our sample facilities are presented in Exhibit VI.4. Administrators were asked if they would admit or retain someone with various care needs. They could respond in one of three ways, yes, no, or it depends. Exhibit VI.4 displays the rates at which administrators indicated yes to the questions concerning admission. The yes rates for the question about retention policies did not vary much from the rates for admission for any of the hypothetical conditions. However, the it depends response rates for the retention question were generally somewhat higher than for the admission questions, indicating that administrators were somewhat more flexible on retention issues than in their admission policies. The difficulty for consumers, however, is that it depends is affixed to some hypothetical situation in the future and is not a response on which they can rely to describe how they will be treated should they develop a specific condition.
As Exhibit VI.4 indicates, the administrators were willing to admit (and retain) individuals who had physical problems that the resident could handle themselves, such as urinary incontinence they could manage on their own (93%) or wheelchair use (80%). By contrast, only slightly more than half (57%) of the administrators of high service or high privacy ALFs were willing to admit a resident who needed some assistance with urinary incontinence. Similarly, only about half of the ALFs (52%) would definitely admit (or retain) individuals who needed assistance with transfers (e.g., from bed to a wheelchair or to standing).
The picture for persons with psychiatric conditions was similar, as long as they did not exhibit any behavioral manifestations. Half (50%) of the administrators in high service or high privacy ALFs were willing to admit individuals who had a severe deficit in memory or judgment (e.g., cognitive skills for daily decision-making), and fewer than half (47%) indicated willingness to admit individuals with a recent psychiatric hospitalization. However, when asked about admission or retention of individuals who exhibited any behavioral symptoms, such as wandering, resisting ADL assistance, or socially inappropriate behaviors, the administrators responded negatively. Only between 12% and 32% of the administrators indicated willingness to admit or retain such individuals, with greater tolerance for wandering and resisting ADL assistance. In general, facilities were also unwilling to admit or retain residents who were restricted to a chair (13%) or bed (3%) because of a health problem.
E. Staffing
In assisted living, as in all residential care settings, staffing and staffing levels are of primary importance. Residents and families have cited issues related to staff as a key element of quality in assisted living, including staff type, staffing levels, staff training and knowledge, and staff attitudes (Hawes et al., 1996; Greene et al., 1998). Thus, many of the questions directed to the administrators had to do with staffing issues, particularly staffing levels.
In examining the resident-staff ratios in ALFs, it is important to remember that in ALFs, unlike other settings such as nursing homes, direct care staff did much more than provide personal care. As noted in Section IV, ALF direct care staff members were often expected to assist with housekeeping, meal service, organized social activities, and medication administration, as well as personal care activities.
1. Staffing By Shift in High Privacy or High Service ALFs
Since ALFs provided 24-hour supervision and service, most had three shifts of workers. On the first shift, which usually ran from early morning to mid-afternoon, the median staffing level for direct care staff was one staff person for every ten residents in the high service or high privacy ALFs. As always with the median, one-half of the facilities had higher staffing, while one-half had lower staffing. Twenty-five percent of the facilities had one direct care staff member for every 16 residents on the first shift, while another 25% of the facilities had a ratio of eight or fewer residents for each direct care staff member on the first shift.
Between mid-afternoon and late evening, on the second shift, the median resident- to-staff ratio was 13 residents for each direct care staff person. The staffing in the 25% of the ALFs with the highest staffing ratio was nine or fewer residents per staff person. The staffing in the 25% of the facilities with the lowest staffing ratio was 20 or more residents per staff member on second shift. On the third shift, the median was 22 residents per direct care staff person, with a ratio of 14 to one or better for facilities in the highest quartile and 34 or more residents per staff person in the lowest quartile of staffing.
2. Licensed Nurse Staffing
Nurse staffing in high service or high privacy ALFs was comprised of combinations of part-time and full-time licensed nurses, that is, Registered Nurses (RNs) and Licensed Practical or Vocational Nurses (LPNs). It included both salaried and contract staff. As Exhibit VI.5 indicates, four patterns occurred with considerable frequency. One third (33%) of all high privacy or high service ALFs had a full or part-time RN and LPN on staff. One-fifth (20%) of these ALFs had a full or part-time RN but no LPN on staff, and another one-fifth (20%) had a full or part-time LPN but no RN on staff. Almost 12% had neither an RN nor an LPN. Thus, one-third (32%) of the ALFs -- the high privacy and low service facilities -- had no RN on staff. The remaining 15% had some other combination of RN and LPN services (e.g., contract RN with staff LPN).
| EXHIBIT VI.5: Full and Part-Time Licensed Nurses in High Privacy or High Service ALFs |
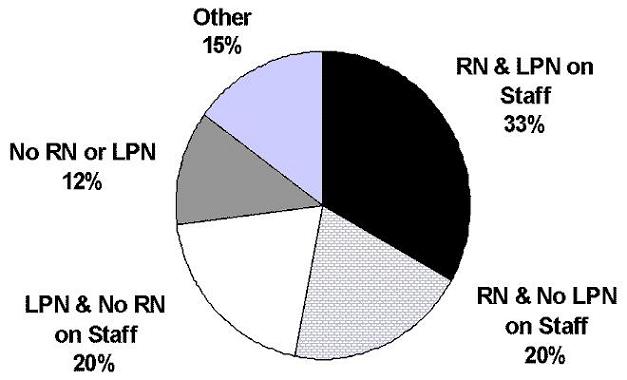 |
3. Other Healthcare Professionals Paid By ALFs and Contracts with Home Health
In the month prior to the site visit, the high privacy or high service facilities paid a wide variety of healthcare professionals as staff or consultants. Three-quarters of the ALFs (76%; 3.52) paid an Activities Director, and just over half (52%; 4.83) of the ALFs paid a registered dietician. Almost one-half (47%; 5.07) had a consulting pharmacist, and just over one-third (36%; 5.36) paid a physician for services as a Medical Director. One-third (33%; 4.18) of the facilities also had a formal arrangement or contract with a home health agency to provide services to residents.
4. Characteristics of Administrators in High Service or High Privacy ALFs
The ALF administrators indicated that the median length of service in their current position in the facility was 2.5 years. More than four out of five of the administrators (84%; 2.31) had worked in some position in the healthcare sector prior to becoming the administrator at the current ALF. However, almost one-quarter (24%; 4.35) of the administrators had received no training in operating a facility for the frail elderly prior to assuming their responsibilities. The highest education level for almost one-third of the administrators (30%; 3.27) was a bachelors degree, while an additional quarter (28%; 3.45) had some post-baccalaureate education. Like the residents, the majority of administrators were white (97%; 1.62) and female (75%; 3.00).
5. Staff Turnover in High Service or High Privacy ALFs
As in most residential care settings, staff turnover in assisted living is a major concern. In focus group interviews, both resident and family members cited low staff turnover as a key indicator of quality (Hawes et al., 1996; Greene et al., 1998). Stability among staff offers the opportunity for more consistent care and a staff that is more familiar with and attuned to individual resident needs and preferences. In assisted living, as in other such settings, personal care assistants or aides have the highest turnover rates among all direct care staff members. According to the administrators in this group of ALFs, one in five aides (20%; 1.80) had been on the job less than six months. Just over 11% (2.68) of RNs had been on staff less than six months. Administrators estimated the annual turnover rate for all direct care staff at 25% (1.63). However, the estimates of annual turnover varied widely, ranging from 0% to 200%.
F. Price and Services in High Privacy or High Service ALFs
1. Charges
As Exhibit VI.6 indicates, charges varied dramatically among the ALFs. In the majority of ALFs (52%; 4.56), the basic monthly price was based on some combination of charges for services provided and the type of resident accommodation provided. In another quarter (25%; 4.23) of the ALFs, the price was based solely on the type of accommodation provided (e.g., studio or one-bedroom apartment; single versus shared room). For the remaining high privacy or high service ALFs (23%), the rate was based on some different set of criteria (e.g., size of the apartment).
| EXHIBIT VI.6: Distribution of Monthly Basic ALF PriceN=4,108 | |||
| Type of Charge | 25th Percentile | Median | 75th Percentile |
| Single Rate | $1,300 | $1,990 | $2,586 |
| Multiple Rate | |||
| Lowest multiple rate | $1,150 | $1,500 | $1,900 |
| Most common rate | $1,400 | $1,735 | $2,200 |
| Highest rate | $1,900 | $2,370 | $2,900 |
Most of the basic monthly charges in the high privacy or high service ALFs ranged between $1,100 and $2,900. Roughly 80% of the ALFs classified as high privacy or high service indicated that they had multiple rates. Because the ALFs had multiple rates, the administrators were asked to report three price categories: their lowest monthly price; the most common price charged, and the highest monthly price charged. The median for the most common rate in those ALFs with multiple rates was $1,735 per month, for an annual cost of $20,820 and a median daily basic price of just over $57. As shown in Exhibit VI.6, the median rate for ALFs with single rates was higher at $1900 per month or $22,800 per year. Thus, ALFs that were able to vary their charge -- by services provided -- for example, had a lower basic price. However, with all ALFs, it is important to remember that this is the basic monthly rate and in most ALFs does not include the price of such ancillary services as daily housekeeping, transportation to appointments, and most ADL assistance, as displayed below in Exhibit VI.7.
2. Services Available
There was considerable variation in the types of services that these high service or high privacy ALFs would provide or arrange and the degree to which these services were included in the basic monthly charge. As Exhibit VI.7 illustrates, the basic rate in many ALFs included little more than the accommodations and meals. (In the exhibit, the services are arrayed from the most frequently provided to the least frequently provided.)
| EXHIBIT VI.7: Services Provided and Arranged by ALFs and, If Offered, Whether Included in the Basic Monthly RateN=3,549 | |||
| Services | Percent of Facilities | ||
| Provided | Arranged | Included* | |
| Three Meals a Day | 99.4 (0.58) | 0.6 (0.58) | 86.5 (2.56) |
| Planned Recreational Activities | 98.7 (0.66) | 1.1 (0.65) | 80.3 (3.11) |
| Assistance with Bathing | 97.8 (1.12) | 1.6 (1.07) | 66.7 (4.95) |
| Laundering Sheets and Towels | 97.5 (1.17) | 0.8 (0.47) | 84.5 (3.06) |
| Assistance with Dressing | 97.2 (1.20) | 1.6 (1.07) | 63.8 (4.77) |
| Medication Storage and Assistance | 97.1 (1.27) | 1.1 (0.49) | 66.4 (4.43) |
| Basic Health Status Monitoring | 96.1 (1.37) | 2.8 (1.02) | 74.7 (3.44) |
| Weekly Housekeeping | 92.0 (2.05) | 0.7 (0.42) | 8.6 (2.97) |
| Exercise or Health Promotion | 91.1 (1.91) | 1.3 (0.98) | 73.0 (3.48) |
| Scheduled Contact with Resident | 89.6 (2.49) | 1.3 (1.06) | 69.6 (3.93) |
| Special Diets | 89.5 (2.32) | 1.1 (0.86) | 68.1 (4.01) |
| Laundering Resident's Clothes | 89.5 (2.42) | 8.1 (2.05) | 59.7 (3.96) |
| Medication Reminders | 86.4 (2.59) | 1.2 (0.53) | 61.1 (3.96) |
| Transportation for Outings | 84.9 (3.00) | 11.0 (2.28) | 65.3 (3.05) |
| Nursing Supervision or Monitoring | 84.2 (2.58) | 8.4 (2.08) | 62.6 (4.01) |
| Meal Delivered to Room | 82.5 (2.60) | 4.3 (1.04) | 46.8 (4.40) |
| Assistance with Locomotion | 82.4 (2.75) | 2.1 (1.13) | 51.4 (4.19) |
| Assistance with Toilet Use | 80.3 (3.02) | 1.5 (0.60) | 48.5 (4.03) |
| Basic Incontinence Care | 78.5 (3.24) | 1.9 (0.62) | 42.5 (3.59) |
| Scheduled Toileting | 73.4 (3.16) | 1.1 (0.53) | 43.8 (3.86) |
| Transportation to Appointments | 67.6 (3.07) | 22.9 (3.10) | 48.3 (3.26) |
| Assistance with Transferring | 65.3 (4.20) | 1.3 (0.56) | 37.6 (4.11) |
| Daily Housekeeping | 60.6 (3.88) | 4.6 (1.19) | 41.7 (4.06) |
| Specialized Dementia Care | 60.1 (4.02) | 1.4 (0.56) | 34.8 (3.68) |
| Temporary Nursing Care | 53.5 (4.59) | 23.4 (3.37) | 35.5 (3.79) |
| Assistance with Eating | 50.6 (3.73) | 3.4 (1.24) | 30.2 (3.60) |
| Minor Foot Care | 50.2 (5.73) | 35.3 (5.09) | 35.6 (5.35) |
| Barber or Hairdresser | 40.4 (4.05) | 57.4 (4.07) | 7.9 (2.92) |
| Incontinence Supplies | 25.0 (3.53) | 27.5 (3.45) | 5.1 (1.74) |
| Hospice Care | 9.6 (2.63) | 57.4 (3.49) | 5.7 (2.23) |
| Overnight Sitter or Companion | 6.9 (1.76) | 42.5 (4.60) | 2.9 (1.33) |
| * Included indicates the cost of the service is included in the basic monthly charge. | |||
Almost all (i.e., >90%) high privacy or high service facilities offered a set of basic services that included three meals a day, planned recreational activities, medication assistance, weekly housekeeping, laundry, basic health status monitoring (e.g., blood pressure), and assistance with such early-loss ADLs as bathing and dressing. Moreover, in nearly all these ALFs, the facility provided these services with their own staff rather than arranging them with an external provider.
The variation among facilities concerning these basic services came in the number of elements of this package of available services that were included in the ALFs basic monthly rate. For example, in almost 15% of the high service or high privacy ALFs, three meals per day were not included in the base rate. Similarly, in roughly one-third of these ALFs, medication assistance and help with bathing and dressing were available, but they were not included in the facilitys basic monthly rate.
The next class of available services was a step beyond the basic service package, and these were provided by between 60% and 85% of the facilities. These other services included nursing care and monitoring (84%), assistance for those with more severe ADL limitations, such as assistance with toileting (80%), transfers (65%), eating (51%), basic incontinence care (79%) (e.g., changing pads, etc.), and transportation to appointments (68%). As shown in Exhibit VI.7, some of the ALFs that did not directly provide services with their own staff were willing to arrange for the provision of these services through an external provider. Such arranged services were largely restricted to services such as transportation, foot care, temporary nursing care, hospice, and similar services. For the most part, ALFs that did not provide ADL assistance with their own staff also did not arrange for such services with other providers. It is also worth noting that, by and large, ALFs did not include these additional services in their basic monthly fee. Thus, the majority of residents using such services as a higher level of ADL assistance, nursing care, or transportation would have had to pay additional fees either to the ALF or to the external provider.
3. Payment Sources and Discharge Policies in ALFs Classified as High Privacy or High Service
The general perception has been that payment for assisted living is solely by private monies; however, that was not completely true. The administrators in nearly one out in five high service or high privacy ALFs (18%; 3.76) reported that the facility had at least one current resident for whom the facility received Medicaid funds, either for personal care services or through a Medicaid waiver program. Nearly one-third (30%; 4.05) of the administrators also reported that at least one resident in the facility had care paid for by Supplemental Security Income (SSI) or a State-provided supplemental payment. However, fewer than 10% of the administrators (9%; 2.06) reported having units set aside for low-income elderly.
| EXHIBIT VI.8: Facility Policies When Private Funds are ExhaustedN=3,017 | |
| Facility Response | Percent of Facilities % (std. error) |
| Discharge Resident | 44.5 (5.35) |
| Use "Charity" Funds | 26.6 (3.53) |
| Accept SSI and State Funds, If Available | 17.6 (4.18) |
| Accept Medicaid, If Available | 11.3 (3.44) |
Despite this, it is important to note that acceptance of Medicaid and SSI was quite small overall, as shown in Exhibit VI.8. The administrators were asked how the facility handled the cases of residents who exhausted their private funds. A majority of facilities would attempt to find some type of public (e.g., Medicaid or SSI) or charity funds to support a residents continued stay in the facility. However, 45% of the facilities would simply discharge the resident who exhausted his or her private funds. In addition, fewer than one in five (18%) administrators reported that they would accept SSI and only about one in ten (11%) would accept Medicaid. Further, since only limited Medicaid funds were available in most states and since most administrators reported that SSI and state supplements were inadequate, discharge was the only recourse in most facilities.30
4. Dementia Care In Assisted Living
Only 5% of the ALFs that provided high services or high privacy indicated that their entire facility was dedicated to providing care for individuals with Alzheimer Disease or some other dementia. However, another 16% of those facilities indicated that a distinct part of their facility had been designated as an Alzheimers Special Care Unit (SCU). This means that just over one-fifth of all ALFs among the high privacy or high service group (21%) identified themselves as providing some type of care they represented as specialized dementia care.
Those facilities reported a number of special features associated with SCUs. Almost all of those ALFs that had a distinct-part unit or that identified themselves as specialized dementia facilities (91%; 3.73) reported that they provided additional training for staff on caring for persons with dementia. Locked exits, alarms, or other features limiting egress were also very common in these settings (87%; 4.58). Enclosed courtyards to limit egress (74%; 7.86) and a higher staff-resident ratio (76%; 7.46) were also frequently reported.31
G. Administrators Concepts of Assisted Living
To clarify their beliefs about what was characteristic of or special about assisted living, administrators were asked which of a variety of concepts they considered central to the concept of assisted living and their facilities approach to care. As the results in Exhibit VI.9 indicate, the administrators almost universally viewed resident autonomy, meeting residents unscheduled needs, and offering privacy and control of the environment as key tenets of the philosophy of assisted living. Four out of every five administrators (79%) also argued that assisted living was a social model of care rather than a medical model. Most (74%) also felt that, in general, assisted living offered a lower level of care than nursing homes, and almost half (49%) felt that residents and their families were responsible for dealing with a residents health care needs. Further, one-third (33%) of the administrators asserted that residents were expected to take care of themselves. These findings raise questions about how the administrators defined the concept of meeting residents unscheduled needs. Further, despite the emphasis on resident autonomy and service flexibility and responsiveness, fewer than one-third (29%) of the ALFs offered negotiated risk contracts as a means of implementing these concepts.
| EXHIBIT VI.9: Administrators' Concepts of Assisted LivingN=4,383 | |
| Issues Central to Assisted Living | Percent of Administrators % (std. error) |
| Meet Residents' Unscheduled Needs | 91.1 (2.14) |
| Resident Autonomy and Choice | 90.5 (2.31) |
| Privacy and Control Over Environment | 89.8 (2.30) |
| Social Rather than Medical Model | 78.8 (3.09) |
| Assisted Living is a Lower Level of Skilled Care Than a Nursing Home | 73.6 (2.60) |
| Resident/Family Responsible for Dealing with Residents' Healthcare Needs | 49.4 (4.28) |
| Residents Expected to Take Care of Themselves | 33.1 (3.43) |
| Ability to Offer Residents Managed or Negotiated Risk Contracts | 29.2 (4.52) |
H. Summary
ALFs that were classified as offering high services or providing a high privacy environment were almost equally likely to be operated by for-profit or by not-for-profit entities. However, firms that provided multiple types of residential care options and services (i.e., located on a multi-level campus) operated the majority of the high privacy or high service ALFs. Facilities showed some variation in the care needs of their residents. Based on administrator estimates, the resident populations were reasonably homogeneous across many ALFs. For the most part, administrators reported a resident case mix with relatively light limitations in ADLs and cognitive status; however, about 15% of the administrators in high service or high privacy ALFs reported having a substantial proportion of residents with heavier care needs.
Staffing varied considerably across the high service or high privacy ALFs. On first shift, one-quarter of these ALFs had direct care staff-to-resident ratios of 8-to-1 or lower, and another quarter had ratios of 16-to-1 or greater. However, the fact that ALF staff tended to be responsible for multiple tasks beyond personal care made it more difficult to interpret the staffing ratios.
While there was considerable variation in staffing ratios, ALFs almost universally utilized some type of full- or part-time licensed nursing staff -- RNs or LPNs. However, one-third of the ALFs classified as high privacy or high service did not have an RN on staff or under contract. Turnover was lowest among licensed nursing staff, but administrators estimated turnover of roughly one-quarter of all direct care staff during the course of a year.
The most common basic monthly charge among the ALFs offering high privacy or high services varied between $1,990 per month for ALFs with single rates and $1,735 for ALFs with multiple rates. This meant an average annual rate for basic services and accommodations of between $21,000 and nearly $24,000. This basic rate, however, did not cover help with medications, bathing or dressing in about one-third of the high privacy or high service ALFs. Moreover, in more than half the ALFs, the basic monthly rate did not cover such services as personal laundry, transportation to medical appointments, or help with getting ardound inside the facility (e.g., walking or using a wheelchair). For those residents who exhausted their private resources paying for care, many ALFs reported being willing to accept alternative sources of payment (i.e., public funding or charity), if they were available. However, policy in nearly half the high service or high privacy ALFs called for the discharge of those who exhausted their private financial resources.
VII. CONCLUSIONS
The development of meaningful national-level information on the assisted living industry is the overall goal of ASPEs National Study of Assisted Living for the Frail Elderly. The data generated by this study should address important questions about assisted living and its potential to meet the needs of older persons and those with disabilities. Further, it should inform consumers, advocates, and policy-makers, facilitating both individual choices and the development of regulatory and financing decisions directed at this burgeoning industry.
Over the last few years, the study has published reports that summarized developments in state policies on the regulation and financing of assisted living, interviews with developers, and an up-dated review of the literature on assisted living. In addition, we have reported results from our various primary data collection activities involving a nationally representative sample of ALFs and residents. The first of these reports was A National Study of Assisted Living for the Frail Elderly: Results of a National Survey of Facilities (Hawes et al., 1999). This report provided extensive descriptive data from a telephone survey of a sample of over 1,500 ALFs that was representative of an estimated national population of 11,459 ALFs serving 521,500 residents. The current report, Assisted Living Residents, Staff, and Facilities, takes a more detailed look at those facilities in the national sample that offered either substantial privacy or extensive services, or both, as well as the residents and staff in those facilities. A third report presents data from a follow-up survey of the residents discussed in this report, focusing in particular on discharged residents and their reasons for exiting the ALF (Phillips et al., 2000). A final report (Hawes, Phillips & Rose, 2000 forthcoming) focuses on the original ASPE study questions, such as the degree to which the industry matches the philosophy of assisted living and examines the effect of different ALF characteristics on such issues as affordability, aging-in-place, and resident satisfaction.
This section of the report on the ALFs classified as providing high services or a high privacy environment attempts to present the findings discussed in the preceding chapters in the context of key issues for consumers and policy-makers.
A. How Impaired Were Assisted Living Residents?
Many advocates for assisted living argue that ALFs can substitute or are substituting for nursing home care, while other observers argue that assisted living houses mainly frail elderly with few significant functional limitations. This study found that most residents were old (i.e., half were aged 85 or older), reported having one or more chronic diseases, and received help administering their daily medications. However, the residents in our sample of high privacy or high service ALFs were significantly less impaired than nursing home residents. Only about one-quarter (27%) of the residents had moderate to severe cognitive impairment, compared to nearly two-thirds of nursing home residents with such impairment (Krauss & Altman, 1998). Similarly, fewer than 10% of ALF residents received assistance with three or more ADLs, while more than 80% of nursing home residents received that level of ADL assistance (Krauss & Altman, 1998; Rhoades & Krauss, 1999).
The study also found that some administrators estimated having a more impaired population than the average ALF. Thus, there may be some overlap of residents at the higher acuity or heavier care end of assisted living and the lower acuity end of nursing homes. However, for the majority of facilities and residents, nursing homes and ALFs had somewhat distinct positions and functions.
It is important to note that a variety of forces militate against ALFs serving as an alternative to nursing homes. These include preferences of many ALF residents to live in settings that do not look too much like a nursing home, the concerns of state regulators about whether residential care is appropriate for very impaired elderly persons, the interest and political clout of the nursing home industry, and the conception that many ALF owners and administrators had of their niche among the range of long-term care services.
B. What Types of Services Were Available To ALF Residents?
Most residents in high privacy or high service ALFs received or had access to a wide range of services, from assistance with simple domestic tasks, such as housekeeping, laundry, and meal preparation, to assistance with bathing and dressing, which are known as early loss ADLs. Similarly, such services as transportation, assistance with medications, exercise and wellness programs, basic health status monitoring, help with locomotion, assistance with toilet use, and nursing supervision or monitoring were available in the vast majority (i.e., >80%) of the high privacy or high service ALFs. The most common way that these services were delivered was by ALF staff.
Other services, such as temporary nursing care and minor foot care, were widely available but less commonly provided by ALF staff (e.g., about half the ALFs would provide these services and another quarter to one-third of the ALFs would arrange for their provision by an external provider). The least commonly available services, such as hospice and overnight sitter or companion services, were typically offered only through an external provider and were available in fewer than six of ten ALFs.
C. Was Staffing Adequate in ALFs?
This question is difficult to address for several reasons. First, there is no consensus about what staffing should be, particularly in terms of nurse staffing. Some providers and advocates argue that assisted living is a social model in which an on-staff nurse is not only unneeded but undesirable. On the other hand, residents and family members of residents with dementia tend to prefer having a Registered Nurse (RN) on staff (Hawes et al., 1996; Greene et al., 1998), and a prior project report found that residents in ALFs with an RN on staff were significantly less likely to be discharged to a nursing home (Phillips et al, 2000). Second, there is no clear evidence about appropriate staffing levels, given the level of cognitive and physical functioning among ALF residents. Moreover, the study was not designed to answer this question, since the staffing data cannot be linked to accurate estimates of resident case mix in each facility. Despite these limitations, there are some relevant data on staffing adequacy, but they do not present a clear picture on staffing adequacy.
First, most but not all of the high privacy or high service ALFs had an RN on staff.32 One-third of the ALFs had no RN on staff, while the other ALFs had a full- or part-time RN on staff. In addition, most of the ALFs without an RN on staff had a full- or part-time LPN. Thus, there were licensed nurses on staff in the vast majority of high privacy and high service ALFs.
Second, there was considerable variability in direct care staffing levels, particularly for staff members identified as personal care assistants (PCAs). The modal, or most common, staffing ratio for PCAs was ten residents per PCA; however, the median number of residents per PCA was 14. This difference reflects the fact that one-quarter of the PCAs had more than 23 residents for whom they were responsible. These staffing levels must be taken together with the fact that most staff reported having multiple responsibilities (e.g., personal care, activities, laundry, and meal service). These levels raise questions about the adequacy of staffing levels, particularly since some residents reported unmet needs for assistance. Twelve percent reported needing more help with dressing and locomotion (walking or using a wheelchair). Further, slightly more than one-quarter (26%) of residents who were receiving some assistance with toilet use reported they had unmet needs for assistance in toileting. Finally, residents reported fairly high ratings of staff performance in most areas (e.g., being treated with dignity, respect and affection). However, only half (52%) reported staff always took the time to listen to them, and fewer than half (42%) reported that adequate numbers of staff were always available.
Third, the picture with respect to staff knowledge of care for the elderly was mixed. Most direct care staff had relatively good knowledge about how to deal with a set of care scenarios presented to them that concerned residents physical health problems and medication management, with the exception of antipsychotic drugs. Similarly, for the most part, they responded correctly to scenarios addressing management of residents with dementia, with the exception of using reality orientation as an appropriate strategy. The most troubling finding was that most staff also had no clear picture of normal aging. The vast majority (i.e., more than three-quarters) thought, for example, that incontinence, confusion, and depression were a normal part of aging, rather than potentially reversible conditions that could be the result of some treatable disease process or physiological problem.
In summary, there is no clear answer about staffing adequacy. On the one hand, most ALFs have both licensed nurses available to monitor residents and supervise care and average direct care staffing ratios of one PCA per 10 residents or better. On the other hand, one-third of the ALFs had no RN on staff and one-quarter had a ratio of one PCA for each 23 or more residents. These staffing patterns are troubling when coupled with the information that: (1) these PCAs were generally responsible for carrying out other tasks, such as meal service, laundry and some housekeeping; (2) most residents (58%) reported adequate numbers of staff were not always available; and (3) significant numbers of residents with functional impairments reported unmet needs. Such information raises questions about whether such ALFs could allow significant aging-in- place and meet the needs of residents with even moderate ADL impairment.
D. Were Policies in High Privacy or High Service ALFs Generally Consistent with ALF Philosophy?
Administrators in the high privacy or high service ALFs generally identified the same basic tenets of assisted living as the trade associations and the Assisted Living Quality Coalition (1998). Nine out of ten administrators identified meeting residents scheduled and unscheduled needs, resident autonomy and choice, and privacy and control over the environment as key elements of assisted living.
Privacy and Environmental Autonomy. The survey results indicated that there was a high degree of consistency between the philosophy of privacy and environmental autonomy and the practices in most of the high privacy or high service ALFs. First, most residents (81%) had a private living space (i.e., bedroom or apartment), and two- thirds (65%) had a private full bathroom. Second, most of these ALFs had practices that were thought to be consistent with resident autonomy over his or her private space. Thus, most residents (i.e., >80%) reported being able to furnish their accommodations with their personal furniture, to arrange their furniture as they like, control the temperature in their room or apartment, and lock their door. Only in terms of ability to store and heat food did a significant proportion of the ALFs perform more poorly than one might expect. Only about one-third (36%) of the residents reported having a kitchen or place to heat food. Moreover, only slightly more than half the residents (54%) had a refrigerator in their room or apartment.
Ability to Meet Scheduled and Unscheduled Needs. There is less clarity about whether the supply of high privacy or high service ALFs matched the philosophy of ability to meet residents scheduled and unscheduled needs. Certainly, these ALFs were willing to make a wide variety of services available to residents. In particular, the vast majority of administrators (i.e., >90%) reported providing assistance with those instrumental and physical ADLs that were predictable and could be scheduled, including bathing, dressing, basic health status monitoring, and medication assistance. There was a less uniform picture with respect to needs that were difficult to schedule. Some services were provided by between approximately two-thirds and four-fifths of the high service or high privacy ALFs, such as assistance with toilet use (80%), locomotion (82%), basic incontinence care (79%) and assistance with transferring (65%). Other services, such as temporary nursing care (54%) and assistance with eating (51%), were provided in only about half the ALFs. However, with temporary nursing care, another quarter of the facilities (23%) reported being willing to arrange for such care with an outside provider, such as a home health agency. The actual experience of residents was slightly different. When asked how they handled need for temporary nursing care, residents reported that the ALF staff provided such care in less than half (45%) the cases and helped arrange for the services with a home health agency or other similar provider in only about 14%of the cases. In one-third of the cases, either the resident was discharged to a nursing facility or hospital (10%) or the resident or family arranged for care from an external provider (22%).33
Resident Autonomy and Choices in Other Areas. Residents and administrators were also asked about other aspects of autonomy and choices. One key area was visiting hours, in which residents had considerable autonomy. The vast majority of residents lived in ALFs that had no restrictions on hours during which visitors were permitted. In other areas, choices were more limited. For example, only half of the residents reported that the ALF usually or always offered activities they enjoyed, and fewer than half (46%) reported that transportation was always or usually available to things they enjoyed. In addition, only 41% of the residents reported that staff always or usually asked about their activity preferences. A similar lack of choices was seen with respect to meals, with only 54% of the residents reporting that they always had a choice among entrees. Finally, advocates for ALFs often argue that they maximize resident autonomy and independence by allowing residents to make choices even when those choices might involve some risk for the resident. However, the formal mechanism for achieving this, managed or negotiated risk contracts, were relatively rare, with only about one-third (29%) of the ALFs having such contracts.
E. Could ALF Residents Age in Place?
According to the data gathered from these high privacy or high service ALFs, residents could be assured of aging in place if they remained relatively healthy and affluent. When residents reached a point where they needed assistance in transferring from a bed to a chair, developed judgment problems or severe memory loss, or began to exhibit troublesome behavioral symptoms, ALF retention policies tended to specify discharge of the resident. Also, when residents exhausted their private resources, their likelihood of remaining in an ALF was dramatically reduced. Only about one-quarter (27%) of the ALF administrators reported they would use charity funds to assist a resident in paying for care, and slightly fewer than one-third of the ALFs (29%) would accept Medicaid or SSI and state supplemental payments, if they were available.
F. Could ALFs Substitute for Nursing Home Care?
The idea that residence in an ALF could substitute for a nursing home is appealing from a variety of perspectives. For many individuals at risk of a nursing home placement, staying in an ALF is probably a preferred outcome, particularly given the greater privacy and environmental control generally available in high privacy or high service ALFs. Whether this represents a realistic option is not yet an answerable question. Research clearly indicates that most residents admitted to and living in nursing homes have very different care needs than most ALF residents (Krauss & Altman, 1998). In addition, prior research and the results of this study demonstrate that the factors that predict nursing home placement (e.g., significant cognitive impairment, behavioral problems, incontinence, and need for assistance in toileting) are also conditions that tend to result in an individuals discharge from most ALFs. Finally, the vast majority of residents in ALFs are private pay, and discharge is the course most commonly available if a resident exhausts his or her private funds. Each of these realities incrementally reduces the proportion of frail elderly for whom an ALF stay might substitute for some portion of a nursing home stay. The fundamental, and as yet unanswered, question is whether ALFs, as they are currently staffed, have the capacity to provide appropriate care to those at risk of a nursing home placement.
G. What Did Residence in an ALF Cost?
The simplest answer to that question is that the basic cost of a high privacy or high service ALF was more than the average elderly individual could afford on his or her income. The median charge in these ALFs was $1,990 per month for those with a single monthly rate. For ALFs with multiple rates, the median "most common" rate was $1735 per month. Thus, the range was between nearly $21,000 and $24,000 per year. These basic rates, however, varied from ALF to ALF in exactly which services were covered. Half or more of the high privacy or high service ALFs charged extra for such services as assistance with locomotion, transfers, eating, toilet use and basic incontinence care; meals delivered to residents rooms; transportation to medical or dental appointments; daily housekeeping; temporary nursing care; and minor foot care. About one-third of the ALFs had ancillary charges for assistance with bathing, dressing, medications, special diets, transportation for social outings, and nurse monitoring or supervision.
These policies were reflected in resident reports on whether they had purchased additional services over and above the basic rate during the preceding month. Sixty- one percent of the residents had purchased additional personal grooming services, such as shampooing and styling hair. Almost 20% had purchased incontinence supplies; 11% additional transportation services; 16% personal laundry services; and 26% foot care (e.g., cutting toenails). Further, one-third of the residents who were aware of the monthly charges indicated that the charges were higher than they had expected.
* * *
In conclusion, assisted living appears to offer an important type of residential long- term care setting for persons with mild or moderate disabilities who cannot safely or securely live alone but do not need the level of care provided in a nursing home. Further, the high privacy or high service ALFs provide this care in a setting that has many components valued by consumers, particularly in terms of privacy and environmental autonomy. In addition, most high service or high privacy ALFs offered a wide array of services. The issue of whether such services can meet residents unscheduled needs is more complex. Moreover, the degree to which such facilities enable residents to age in place is clearly mixed unless one limits the concept to one of "aging in place without significant decline in physical or cognitive functioning." Finally, assisted living is still a largely private-pay sector and, among the high service or high privacy ALFs, one that is largely unaffordable for most moderate and low income older persons unless they spend down their assets or receive help from relatives.
REFERENCES
Ahlen, K., & Major, M. (1999). National study of assisted living for the frail elderly: Field data collection report. Research Triangle Park, NC: Research Triangle Institute.
American Seniors Housing Association. (1998). Seniors housing construction report -- 1998. Washington, DC: American Seniors Housing Association.
Assisted Living Federation of America. (1998). The assisted living industry: An overview --1998. Fairfax, VA: Price Waterhouse for ALFA.
Assisted Living Quality Coalition. (1998). Assisted living quality initiative: Building a structure that promotes quality. Washington, DC: Assisted Living Quality Coalition.
Blessed, G.,Tomlinson, B., & Roth, M. (1968). The association between quantitative measures of dementia and of senile change in the cerebral grey matter of elderly subjects. British Journal of Psychiatry, 114: 797-811.
Callahan, D. (1987). Setting limits: Medical goals in an aging society. New York: Simon and Schuster.
Citro, J., & Hermanson, S. (1999). Assisted living in the United States. AARP Working Paper, unpublished. Washington, DC: American Association of Retired Persons, Public Policy Institute.
Clark, R., Turek-Brezina, J., Hawes, C., & Chu, C. (presenters). (November 1994). The supply of board and care homes: Results from the 1990 national health provider inventory. [Presentation], Atlanta, GA: Gerontological Society of America.
Cleary, P., & McNeil, B. (1988). Patient satisfaction as an indicator of quality care. Inquiry, 25: 25-36.
Greene, A., Hawes, C., Wood, M., & Woodsong, C. (1998). How do families define quality in assisted living facilities? Generations 21(4): 34-36.
Gulyas, R. (1997). The not-for-profit assisted living industry: 1997 profile. Washington, DC: American Association of Homes and Services for the Aging.
Harrington, C., Dunah, R., Bedney, B., & Carillo, H. (1994). Variations and trends in licensed nursing home capacity in the states, 1978-1993. San Francisco, CA: Institute for Health and Aging, University of California at San Francisco.
Harrington, C., Kovner, C., Mezey, M., Kayser-Jones, J., Burger, S., Mohler, M., Burke, R., & Zimmerman, D. (2000). Experts recommend minimum nurse staffing standards for nursing facilities in the United States. Gerontologist, 40 (1): 4-17.
Hawes, C. (2000). Unpublished data - results of focus group interviews with staff in nursing homes and assisted living facilities for HCFA (2000) and for the Alzheimers Association (1997).
Hawes, C., Greene, A., Wood, M. and C. Woodsong (1996). Family Members Views: What Is Quality in Assisted Living for People With Dementia? (Washington, DC: Alzheimers Association). [http://aspe.hhs.gov/daltcp/reports/fmviews.htm]
Hawes, C., Lux, L., Wildfire, J., Green, R., Packer, L., Iannacchione, V., & Phillips, C. (1995a). Study of North Carolina domiciliary care home residents. Research Triangle Park, NC: Program on Aging and Long-Term Care, Research Triangle Institute.
Hawes, C., Mor, V., Wildfire, J., Lux, L., Green, R., Iannacchione, V., & Phillips, C. (1995b). Executive summary: Analysis of the effects of regulation on the quality of care in board and care homes. Research Triangle Park, NC: Program on Aging and Long- Term Care, Research Triangle Institute. [http://aspe.hhs.gov/daltcp/reports/care.htm]
Hawes, C., Rose, M., & Phillips, C. (1999a). A national study of assisted living for the frail elderly, executive summary: Results of a national survey of facilities. Beachwood, OH: Myers Research Institute. [http://aspe.hhs.gov/daltcp/reports/facreses.htm]
Hawes, C., Rose, M., & Phillips, C. (1999b). A national study of assisted living for the frail elderly: Results of a national telephone survey of facilities. Beachwood, OH: Myers Research Institute. [http://aspe.hhs.gov/daltcp/reports/facres.htm]
Hawes, C., Wildfire, J., & Lux, L. (1993). The regulation of board and care homes, results of a 50-state survey: National summary. Washington, DC: American Association of Retired Persons.
Hawes, C., Wildfire, J., Iannachionne, V., Lux, L., Greene, A., Mor, V., & Laliberte, L. (1996). Report on study methods: Analysis of the effect of regulation on the quality of care in board and care homes. Research Triangle Park, NC: Program on Aging and Long-Term Care, Research Triangle Institute. [http://aspe.hhs.gov/daltcp/reports/stumthes.htm]
Hawes, C., Wildfire, J., Mor, V., Wilcox, V., Spore, D., Iannacchione, V., Lux, L., Green, R., Greene, A., & Phillips, C. (1995c). A description of board and care facilities, operators, and residents. Research Triangle Park, NC: Program on Aging and Long- Term Care, Research Triangle Institute. [http://aspe.hhs.gov/daltcp/reports/bcdesces.htm]
Hodlewsky, R. (1998). Facts and trends: 1998 the assisted living sourcebook. Washington, DC: National Center for Assisted Living, American Health Care Association.
Iannacchione, V., Byron, M., Lux, L., Wrage, L., & Hawes, C. (1999). A national study of assisted living for the frail elderly: Final sampling and weighting report. Beachwood, OH: Myers Research Institute. [http://aspe.hhs.gov/daltcp/reports/sampweig.htm]
Jenkens, R. (1997). Assisted living and private rooms: What people say they want. Washington, DC: American Association of Retired Persons, Public Policy Institute.
Kane, R., Baker, M., Veazie, W., & Solomon, J. (1998). Consumer perspectives on private versus shared accommodations in assisted living settings. Washington, DC: American Association of Retired Persons, Public Policy Institute.
Kane, R., & Wilson, K. (1993). Assisted living in the United States: A new paradigm for residential care for frail older persons? Washington, DC: American Association of Retired Persons.
Katzman, R., Brown, T., Fuld, P., Peck, A., Schechter, R., & Schimmel, H. (1983). Validation of a short-orientation-memory-concentration test of cognitive impairment. American Journal of Psychiatry, 140: 734-739.
Kish, L. (1965). Survey sampling. New York: John Wiley & Sons.
Krauss, N., & Altman, B. (1998). Characteristics of nursing home residents -- 1996. Rockville, MD: Agency for Health Care Policy and Research. 1988 MEPS Research Findings No. 5. AHCPR Pub. No. 99-0006.
Krauss, N., Freiman, M., Rhoades, J., Altman, B., Brown, E., & Potter, D. (1997). Nursing home update -- 1996: Characteristics of nursing facilities and residents. Rockville, MD: Agency for Health Care Policy and Research. MEPS Highlights, Number 2, AHCPR Pub. No. 97-0036.
Krauss, N., Machlin, S., & Kass, B. (1999). Use of health care services, 1996. Rockville, MD: Agency for Health Care Policy and Research. MEPS Research Findings No. 7. AHCPR Pub. No. 99-0018.
Lawton, M. (1976). The relative impact of congregate and traditional housing on elderly tenants. Gerontologist 16(3): 237-242.
Leon, J., Cheng, C-K., & Neumann, P. (1998). Alzheimers disease care: Costs and potential savings. Health Affairs, 17(6): 206-216.
Manard, B., Altman, N., Kane, L., & Zeuschner, A. (1992). Policy synthesis on assisted living for the frail elderly. Fairfax, VA: Lewin-VHI, Inc. [http://aspe.hhs.gov/daltcp/reports/polsynes.htm]
Manard, B. & Cameron, R. (1997). A national study of assisted living for the frail elderly: Report on in-depth interviews with developers. Washington, DC: The Lewin Group. [http://aspe.hhs.gov/daltcp/reports/indepth.htm]
McGuire, C. (2000). Presentation on Case Mix in Residential Care at the National Care Mix 2000 Conference, Madison, WI: May 22, 2000.
Meister, C., & Boyle, C. (1996). Perceptions of quality in long-term care: A satisfaction survey. Journal of Nursing Care Quality 10(4): 40-47.
Mollica, R. (1998). State assisted living policy -- 1998. Portland, ME: National Academy for State Health Policy. [http://aspe.hhs.gov/daltcp/reports/98state.htm]
Mollica, R., & Snow, K. (1996). State assisted living policy -- 1996. Portland, ME: National Academy for State Health Policy. [http://aspe.hhs.gov/daltcp/reports/96state.htm]
Moos, R. H., & Lemke, S. (1980). Assessing the physical and architectural features of sheltered care settings. Journal of Gerontology, 35(4), 571-583.
Mor, V., Sherwood, S., & Gutkin, C. (1986). A national study of residential care for the aged. The Gerontologist, 26 (4): 405-417.
Morris, J., Fries, B., Mehr, D., Hawes, C., Phillips, C., Mor, V., & Lewis, L. (1994). MDS cognitive performance scale. The Journals of Gerontology: Medical Sciences, 49: M174-M182.
Newcomer, R., Lee, P., & Wilson, K. (1997). Residential care for the frail elderly: State innovations in placement, financing, and governance. San Francisco, CA: University of California at San Francisco Institute for Health and Aging.
Newcomer, R., Preston, S., & Roderick, S. (1995). Assisted-living and nursing unit use among continuing care retirement community residents. Research on Aging, 17 (2): 149-167.
Pascoe, G. (1983). Patient satisfaction in primary health care: A literature review and analysis. Evaluation and Program Planning, 6: 185-210.
Phillips, C., Hawes, C., Green, R., and Norton, E. (1998). Medicare utilization among board and care residents. Beachwood, OH: Myers Research Institute, Menorah Park Center for Senior Living.
Phillips, C.D., Hawes, C. Spry, K. and Rose, M. (2000). A national study of assisted living for the frail elderly: Residents leaving assisted living -- descriptive and analytic results from a national sample. Beachwood, OH: Myers Research Institute, Menorah Park Center for Senior Living. [http://aspe.hhs.gov/daltcp/reports/alresid.htm]
Powell, M. (1976). The relative impact of congregate and traditional housing on elderly tenants. Gerontologist. 16(3): 237-242.
Rhoades, J. and Krauss, N. (1999). Nursing home trends, 1987 and 1996. Rockville, MD: Agency for Health Care Policy and Research; 1999. MEPS Chartbook No. 3 AHCPR Pub. No. 99-0032.
Rudder, C., & Phillips, C. (1998). 91 ideas for reducing costs, enhancing revenue, and maintaining quality in nursing homes. NY: Nursing Home Community Coalition of New York State.
Shah, B., Barnwell, B., & Bieler, G. (1997). SUDAAN: Users manual, Release 7.5, Volume 1. Research Triangle Park, NC: Research Triangle Institute.
D. Spore, V. Mor, J. Hiris, E. P. Larrat, C. Hawes. (1995). Psychotropic use among older residents of board and care facilities. Journal of the American Geriatrics Society, 43(12), 1403-1409.
United States Congress, General Accounting Office (1997). Consumer protection and quality of care issues in assisted living. Report to Senator Ron Wyden. Washington, DC: Government Printing Office.
United States Congress, General Accounting Office. (1999). Assisted living: Quality-of-care and consumer protection issues in four states. Report to Congressional Requesters.
Williams, T., & Temkin-Greener, H. (1996). Older people, dependency, and trends in supportive care. In R. H. Binstock, L.E. Cluff, & O. Von Mering (Eds.). The future of long-term care: Social and policy issues (pp. 51-74). Baltimore and London: The Johns Hopkins University Press.
Wilson, K. (1993). Developing a viable model of assisted living. In P. Katz, R. Kane, & M. Mazey (Eds.). Advances in long-term care. New York: Springer.
NOTES
-
Facilities that did not call themselves "assisted living" had to have at least 11 beds, primarily serve the frail elderly, house no more than two unrelated individuals in a room, provide at least two meals a day, 24-hour supervision, housekeeping services, and assistance with at least two activities of daily living (ADL) or one ADL and assistance with medications.
-
These data come from the staff interviews, and the staff interviewed almost exclusively worked the day shift. Information on staffing by shift appears in Section VI of the report.
-
Senior housing includes assisted living facilities, continuing care retirement communities, congregate apartments, senior/retirement apartments.
-
The Coalition is a group representing the Alzheimers Association, AARP, the American Association of Homes and Services for the Aging [AAHSA], the Assisted Living Federation of America [ALFA], the American Seniors Housing Association, and the American Health Care Association/National Center for Assisted Living (NCAL).
-
ALFs may provide services with their own staff or arrange for the provision of services through an external provider, such as a home health agency.
-
By this definition, a facility had to either define itself as an assisted living facility OR provide 24-hour staff oversight, housekeeping, at least 2 meals a day, and assistance with at least two of the following: medications, bathing, or dressing.
-
This growth has probably added more than 6,000 facilities and 300,000 beds to the residential care sector since the early 1990s, bringing the total to more than 50,000 residential care facilities with more than one million beds (Clark, Turek-Brezina, Hawes & Chu, 1994; Hawes et al., 1995a).
-
There is essentially no federal regulation of any type of residential care, including assisted living, other than the Keys Amendments that require states to certify that no person receiving Supplemental Security Income (SSI) is residing in a substandard facility.
-
The precise criteria for inclusion in the sub-sample of ALFs offering a high level of services or privacy (or both) appears in Section Two of this report.
-
The 300 ALFs that were included in the site visits that form the basis for this report are a representative sub-sample of the facilities that met the specified criteria for offering a high level of privacy or a high level of services or both.
-
The effect of these service arrangements on length-of-stay and other variables is being tested, and the analytic results will be presented in a subsequent report.
-
All project instrumentation will be included in the public use data files issued by ASPE.
-
Finally, members of the resident sample in the Tier #3 facilities who were discharged, died or otherwise exited the facility within the first six months following the site visit were interviewed. If they were deceased or could not respond, a family member was interviewed. The results are not discussed in any detail in this report but can be found in Phillips, Hawes Spry & Rose, 2000).
-
Interviews were conducted in a total of 305 ALFs; however, the full complement of interviews (i.e., with administrators, other staff, and residents) and the structured walk-through observation was completed in only 300 ALFs.
-
Most residents (80.7%) were classified based on their responses to items on the Short Blessed exam (Blessed, Tomlinson & Roth, 1968; Katzman et al., 1983). For residents unable to respond in the interview, proxy respondents provided information to items from the Cognitive Performance Scale (CPS) (Morris et al., 1994) that allowed the residents to be classified into the three categories of cognitive function compatible with categories of scores derived from the Short Blessed. This process is discussed in greater detail in Appendix A.
-
Bathing was excluded since facility policies, often based on liability insurance, tend to influence the rate of assistance with bathing.
-
This level of reported assistance could be a product of functional limitations among residents or of facility policy (i.e., that all medications are centrally stored and distributed by staff) -- or a combination.
-
Administrators were asked what proportion of their residents had received help with any of the following: locomotion, toilet use, transfers, or eating. A resident who received help with any of these later loss ADLs would almost always also be receiving help with bathing and dressing. Thus, we assumed that a an estimate of the proportion of residents receiving hands-on assistance with the later loss ADLs constituted help with three or more ADLs.
-
For all comparisons involving the three facility types, the statistical significance of the prevalence in each type of facility was compared with that in the population as a whole using a series of logistic regressions in which the independent variables were the facility types.
-
Temporary care or monitoring was defined as less than 14 days in duration.
-
The correct response was that all of the listed symptoms (e.g., tremors, muscle rigidity, gait disturbance, thrusting movement with tongue, and increased agitation) were ones that should be noted and reported.
-
A prior study of residential care facilities in ten states included assisted living facilities and also found that residents of these facilities were taking more daily medications than were residents of nursing homes (Hawes et al., 1995c; Spore et al., 1995).
-
We know that recipients of services, such as residents, exhibit what is known as a positivity bias when asked about their satisfaction with the service. There may be a similar tendency for staff to provide answers to satisfaction questions on an interview schedule that are somewhat more positive than one would obtain with a more intensive or more private method of data gathering.
-
In the table, items were reworded so that agreement reflected a positive statement. In the original interview, the wording of items was deliberately mixed, so that agreement could mean something positive or negative, depending on the item.
-
A permanent assignment means, in general, that an aide is assigned on a regular basis to the same group of residents. By contracts, a floating assignment means that the aide provides care and services to a different group of residents each day.
-
They used items from the Multiphasic Environmental Assessment Procedure (MEAP) (Moos and Lemke, 1980). These well-tested and validated items included a variety of environmental features, including safety devices, lighting, maintenance, cleanliness, availability of social and recreational aids, and so on.
-
A more detailed discussion of the criteria for inclusion in the site visits was provided in Section II.
-
A multi-level campus was one that housed an eligible ALF and some other type of housing for the elderly, such as congregate apartments, independent living, or a nursing home. A nursing home was the most common type of other supportive housing setting.
-
Figures such as these are somewhat deceptive. Some residents will have lengths of stay much longer than the average, while many residents will have relatively shorter stays. For example, in our survey of discharged residents (Phillips et al., 2000), the average length of stay of the discharged residents was 19.6 months.
-
Another project report provides information on a national probability sample of residents who had been discharged or otherwise exited the high privacy or high service ALFs ((Phillips et al., 2000). The vast majority of residents and their next-of-kin reported that the residents left because they needed more care and services than the ALF offered, rather than because they had exhausted their funds. Only between eight and nine percent of the residents left because they exhausted their funds.
-
It is important to note that the study did not evaluate the nature or quality of these features beyond the administrators report that the features in question were present (or absent).
-
All of the high service ALFs had at least a full-time RN on staff.
-
Percentages total 101 because of rounding.
OTHER REPORTS AVAILABLE
A National Study of Assisted Living for the Frail Elderly: Discharged Residents Telephone Survey Data Collection and Sampling ReportHTML http://aspe.hhs.gov/daltcp/reports/drtelesy.htm PDF http://aspe.hhs.gov/daltcp/reports/drtelesy.pdf
A National Study of Assisted Living for the Frail Elderly: Final Sampling and Weighting Report HTML http://aspe.hhs.gov/daltcp/reports/sampweig.htm PDF http://aspe.hhs.gov/daltcp/reports/sampweig.pdf
A National Study of Assisted Living for the Frail Elderly: Final Summary Report HTML http://aspe.hhs.gov/daltcp/reports/finales.htm PDF http://aspe.hhs.gov/daltcp/reports/finales.pdf
A National Study of Assisted Living for the Frail Elderly: Report on In-Depth Interviews with DevelopersExecutive Summary http://aspe.hhs.gov/daltcp/reports/indpthes.htm HTML http://aspe.hhs.gov/daltcp/reports/indepth.htm PDF http://aspe.hhs.gov/daltcp/reports/indepth.pdf
A National Study of Assisted Living for the Frail Elderly: Results of a National Study of FacilitiesExecutive Summary http://aspe.hhs.gov/daltcp/reports/facreses.htm HTML http://aspe.hhs.gov/daltcp/reports/facres.htm PDF http://aspe.hhs.gov/daltcp/reports/facres.pdf
Assisted Living Policy and Regulation: State Survey HTML http://aspe.hhs.gov/daltcp/reports/stasvyes.htm PDF http://aspe.hhs.gov/daltcp/reports/stasvyes.pdf
Differences Among Services and Policies in High Privacy or High Service Assisted Living Facilities HTML http://aspe.hhs.gov/daltcp/reports/alfdiff.htm PDF http://aspe.hhs.gov/daltcp/reports/alfdiff.pdf
Family Members' Views: What is Quality in Assisted Living Facilities Providing Care to People with Dementia? HTML http://aspe.hhs.gov/daltcp/reports/fmviews.htm PDF http://aspe.hhs.gov/daltcp/reports/fmviews.pdf
Guide to Assisted Living and State Policy HTML http://aspe.hhs.gov/daltcp/reports/alspguide.htm PDF http://aspe.hhs.gov/daltcp/reports/alspguide.pdf
High Service or High Privacy Assisted Living Facilities, Their Residents and Staff: Results from a National SurveyExecutive Summary http://aspe.hhs.gov/daltcp/reports/hshpes.htm HTML http://aspe.hhs.gov/daltcp/reports/hshp.htm PDF http://aspe.hhs.gov/daltcp/reports/hshp.pdf
National Study of Assisted Living for the Frail Elderly: Literature Review Update Abstract HTML http://aspe.hhs.gov/daltcp/reports/ablitrev.htm Abstract PDF http://aspe.hhs.gov/daltcp/reports/ablitrev.pdf HTML http://aspe.hhs.gov/daltcp/reports/litrev.htm PDF http://aspe.hhs.gov/daltcp/reports/litrev.pdf
Residents Leaving Assisted Living: Descriptive and Analytic Results from a National SurveyExecutive Summary http://aspe.hhs.gov/daltcp/reports/alresdes.htm HTML http://aspe.hhs.gov/daltcp/reports/alresid.htm PDF http://aspe.hhs.gov/daltcp/reports/alresid.pdf
State Assisted Living Policy: 1996Executive Summary http://aspe.hhs.gov/daltcp/reports/96states.htm HTML http://aspe.hhs.gov/daltcp/reports/96state.htm PDF http://aspe.hhs.gov/daltcp/reports/96state.pdf
State Assisted Living Policy: 1998Executive Summary http://aspe.hhs.gov/daltcp/reports/98states.htm HTML http://aspe.hhs.gov/daltcp/reports/98state.htm PDF http://aspe.hhs.gov/daltcp/reports/98state.pdf
INSTRUMENTS AVAILABLE
Facility Screening Questionnaire PDF http://aspe.hhs.gov/daltcp/instruments/FacScQ.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]