
U.S. Department of Health and Human Services
Executive Summary: Analysis of the Effect of Regulation on the Quality of Care in Board and Care Homes
Catherine Hawes, Vincent Mor, Judith Wildfire, Vince Iannacchione, Linda Lux, Rebecca Green, Angela Greene, Victoria Wilcox, Diana Spore and Charles D. Phillips
Research Triangle Institute and Brown University
July 10, 1995
This report was prepared under contract #HHS-100-89-0031 between HHS's Office of Family, Community and Long-Term Care Policy (now the Office of Disability, Aging and Long-Term Care Policy) and the Research Triangle Institute. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The Project Officer was Floyd Brown.
TABLE OF CONTENTS
- SUMMARY OF KEY FINDINGS
- 3.1 Characteristics of Board and Care Environments
- 3.2 Effect of Extensive Regulation
- 3.3 Effect of Licensure
- 3.4 Role of Board and Care Homes
- OVERVIEW OF STUDY METHODS
- 4.1 State Selection
- 4.2 Sampling of Licensed and Unlicensed Homes
- 4.3 Data Collection
- 4.4 Data Analysis
- 4.5 Limitations of Study Design
- THE BOARD AND CARE ENVIRONMENT: CHARACTERISTICS OF HOMES AND RESIDENTS
- 5.1 Characteristics of Homes
- 5.2 Characteristics of Residents
- 5.3 Niche Served by Board and Care Homes
- EFFECT OF REGULATION AND LICENSURE ON QUALITY OF CARE
- 6.1 Effect of Regulatory System on Quality
- 6.2 Effect of Licensure on Quality
- 6.3 Conclusion
- EFFECT OF REGULATION ON SUPPLY AND CHARACTERISTICS OF BOARD AND CARE HOMES
- 7.1 Licensed Homes
- 7.2 Unlicensed Homes
- 7.3 Conclusion
- CONCLUSIONS
- 8.1 Study Findings
- 8.2 Implications of Study Findings
- EXHIBITS
- EXHIBIT 1. Summary of Effects of Regulation on Quality
- EXHIBIT 2. Distribution of Board and Care Homes and Residents by Home Size
- EXHIBIT 3. Board and Care Home Resident Care Mix by Facility Type
- EXHIBIT 4. Services Provided by Homes
- EXHIBIT 5. SSI/SSP Payer Mix and Monthly Rate by Facility Type
- EXHIBIT 6. Distribution of Monthly SSI/SSP and Private Pay Rates
- EXHIBIT 7. Services Covered by Monthly Rate
- EXHIBIT 8. Comparison of Residents
- EXHIBIT 9. Board and Care Staff Who Administer Medication
- EXHIBIT 10. Level of ADL Impairment by Cognitive Impairment Level in Board and Care Home Residents
- EXHIBIT 11. Nursing Home and Licensed Board and Care Home Bed Supply, 1989-1990
- EXHIBIT 12. Comparison of Proportion of Licensed to Unlicensed Homes
SECTION 1: BACKGROUND
A variety of demographic factors and policy initiatives have increased demand for residential facilities that offer supportive services for the aged and disabled. These factors include
- A rapidly growing elderly population with significant levels of physical disability and mental impairment
- The almost universal rejection of nursing home care by younger persons with disabilities and their advocates
- A strong preference of the elderly for in-home and community-based services rather than nursing homes.
Although families continue to be the major source of long-term care, a variety of residential settings with supportive services have emerged to supplement their efforts. These arrangements support families whose members need more care than the family can provide and those elderly and disabled who have no family. Other than nursing homes, the most common form of residential setting with services for people with disabilities is board and care homes. This term is used in a variety of ways across the States. For this study, however, "board and care" refers to nonmedical community-based residential settings that house two or more unrelated adults and provide some services such as meals, medication supervision or reminders, organized activities, transportation, or help with bathing, dressing, and other activities of daily living (ADLs).
- personal care homes
- rest homes
- domiciliary care homes
- residential care homes
- homes for the aged
- assisted living facilities.
There are approximately 34,000 licensed board and care homes in the United States with more than 613,000 beds (Clark et al., 1994). These homes fall into one of three basic types of licensed facilities (Clark et al., 1994): (1) homes serving a clientele with mental retardation or developmental disabilities; (2) homes serving a clientele with mental illness; and (3) homes serving a mixed population of physically frail elderly, cognitively impaired elderly, and persons with mental health problems. The majority of homes fall into this last category. Not all board and care facilities, however, are licensed, and there is little uniform or comprehensive information about such homes. Unlicensed homes are as numerous as licensed facilities by some estimates (U.S. House, 1989). Thus, the total number of persons living and receiving long-term care in all types of board and care homes may be as high as 1 million (Clark et al., 1994; Hawes et al., 1993; Moon et al., 1989; U.S. House, 1989). As a point of comparison, there are an estimated 17,000 licensed nursing homes with approximately 1.68 million beds serving more than 1.5 million nursing home residents (DuNah et al., 1993).
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) in the U.S. Department of Health and Human Services (DHHS) has a long-standing interest in the potential of board and care homes to meet the needs of aged and disabled persons for residential services. ASPE commissioned a study in the early 1980s by Denver Research Institute (DRI) that described board and care homes and residents in five States and investigated the effect of regulation on quality of care (Dittmar and Smith, 1983). Other studies during the 1980s also attempted to describe homes and residents, the regulation of these homes by States, and the role these facilities play in providing long-term care (i.e., Reichstein and Bergofsky, 1980; Sherwood et al., 1981).
In the early 1990s, ASPE initiated a new examination of board and care homes and their role in the long-term care system. This time the policy interest was threefold:
- To document the characteristics of board and care homes, how much they had grown in the United States since the initial studies of the 1980s, and the role they play in meeting the need for long-term care
- To describe the characteristics of board and care residents, particularly the extent of frailty and disability among residents
- To assess the quality of care received by board and care residents and examine the effect of State regulation on the quality of that care.
To address these questions, ASPE launched two related initiatives. The first by Lewin-VHI, Inc., was a national survey of State licensure agencies to determine the number and types of homes and to generate a list of homes (Manard et al., 1990). The second initiative is the study reported here, and it addresses concerns related to board and care quality. ASPE placed a high priority on the need to evaluate board and care quality for several reasons.
First, the Federal expenditures directed at home and community-based services for persons with disabilities in all types of community-based residential settings was increasing rapidly in the early 1990s. Nevertheless, the Federal government played only a limited role in monitoring or regulating the quality of those services. The regulation of board and care was primarily a State responsibility, with the Federal role largely limited to the oversight specified in the Keys Amendments.1 The emphasis on strengthening Federal oversight of nursing home quality required by the Omnibus Budget Reconciliation Act of 1987 served to highlight the lack of systematic information on board and care residents and the effect of State regulations on their well-being. Second, there was a belief that the residents of board and care homes were far more disabled than they had been a decade before. Third, concerns were raised by the U.S. General Accounting Office, congressional hearings, and other studies that residents were not receiving adequate care or protection from health and safety risks (Avorn et al., 1989; Budden, 1985; GAO, 1989; 1992a; 1992b; Hartzema et al., 1986; U.S. House, 1989). These studies reported evidence of unsafe and unsanitary conditions, widespread use of psychotropic medications, lack of staff knowledge about medication administration, and other health and safety problems. Fourth, several reports raised questions about the effectiveness of State regulatory efforts (ABA, 1983; Dobkin, 1989; GAO, 1989; Hawes et al., 1993; Newcomer and Grant, 1988; Reichstein and Bergofsky, 1980; Stone and Newcomer, 1985; U.S. DHHS Inspector General, 1990). In addition, there were assertions that significant numbers of board and care homes were unlicensed and unregulated (U.S. House, 1989).
This report summarizes ASPE's analysis of the effect of regulation and licensure on the quality of care in board and care homes. Study purpose and methodology are described, major findings are presented, and implications of the study findings are discussed.
SECTION 2: STUDY PURPOSE AND APPROACH
Goals of This Study
- To describe the board and care environments
- To determine the effect of State regulation on quality of care
- To examine the differences between licensed and unlicensed homes
ASPE contracted with the Research Triangle Institute (RTI) to examine the quality of care in board and care homes in 10 States, five with extensive regulatory systems and five with more limited regulatory systems. The criteria used to define extensive and limited, including characteristics of the licensing regulations, inspection process, and approach to enforcement, are discussed in greater detail in Section 4. The principal purpose of the study was to analyze and compare State board and care regulations and their effects on the quality of care received by board and care residents. The study was to answer the following questions:
- What were the characteristics of the board and care environments in the study States, including the characteristics of the homes, operators, staff, and residents?
- What was the effect of State regulation on the quality of care and the experience of board and care residents?
- Were licensed and unlicensed homes markedly different? In particular, did facilities vary with respect to quality of care?
To accomplish this objective, data on State regulatory systems were analyzed, a sample frame of licensed and unlicensed homes was constructed, and a complex multistage sample design was implemented. Data on homes, staff, and residents in licensed and unlicensed homes in 10 States were then collected and analyzed. In addition, comparisons were made to the findings of earlier studies of board and care as well as to current data on the characteristics of other residential long-term care settings in order to clarify the role played by board and care homes.
The study methodology is described in detail in a forthcoming technical report, Project Study Methods. More extensive data on analytic methods and the characteristics of homes, operators, staff, and residents are presented in a forthcoming technical report, A Description of Board and Care Homes, Staff, and Residents. The analytic approach, multivariate models, and statistical results examining the impact of regulation and licensure on quality are presented in the forthcoming report, The Effect of Regulation on Quality of Care in Board and Care Homes.
SECTION 3: SUMMARY OF KEY FINDINGS
This section summarizes major findings of the ASPE study. See Sections 5 through 7 for more detailed discussions of the results.
3.1 Characteristics of Board and Care Environments
3.1.1 Homes
- Board and care homes fill an important niche in long-term care. They provide more extensive services and protective oversight than other residential settings, such as congregate apartments, but a lower level of care and services than is offered by nursing homes.
- The widespread perception that board and care homes are small and thus more "homelike" is somewhat misleading. Although most homes were small (2-10 beds), more than three-quarters of the residents lived in homes with 11 or more beds.
- Although the majority of homes provided access to a range of services, most were unable or unwilling to accommodate changing resident needs. For example, if a resident became ill and needed nursing care for more than 14 consecutive days, most homes would discharge the resident to a hospital or nursing home.
- The staffing ratios found in homes, the minimal training required of staff, and a lack of appropriate staff knowledge raise questions about whether board and care homes are capable of providing adequate care, particularly in managing medications and monitoring their effects.
- An estimated 12 percent of all board and care homes in the 10 study States were unlicensed.
- The study found a new type of large unlicensed home not identified in prior studies: apartments, retirement communities, and assisted living facilities that were unlicensed as board and care homes but provided meals, protective oversight, and the same types of services as licensed board and care homes.
3.1.2 Residents
- The average resident is older and more disabled than was true a decade ago.
- Only 22 percent of the residents were age 18 to 64. Thirty percent of the residents were age 75 to 84; 34 percent were 85 or older. Thus, 64 percent were age 75 or older. By comparison, the DRI study in the early 1980s found that only 38 percent were 75 or older.
- Forty percent of the residents were moderately to severely cognitively impaired, 23 percent had urinary incontinence, 15 percent used a wheelchair, and 7 percent were bedfast or chairfast. By comparison, the DRI study found 30 percent of the residents were "confused," 7 percent had urinary incontinence, 3 percent used a wheelchair, and only 2 percent were bedfast or chairfast.
- Forty-one percent of the residents received one or more psychotropic medications.
3.2 Effect of Extensive Regulation
- Extensive State regulation had an effect on the prevalence of unlicensed homes: in States with extensive regulatory systems, only 7 percent of all homes were unlicensed; in States with limited regulation, 25 percent were unlicensed.
- As shown in Exhibit 1, extensive regulation had a positive effect on several quality indicators. These include lower use of psychotropic drugs, lower use of medications contraindicated for the elderly, more operator training, and greater availability of social aids and supportive devices.
- Extensive regulation had no effect on such measures as the operator's requirements for staff training, availability of licensed nurses, or staff knowledge of basic care, monitoring, or medication supervision.
- Extensive regulation had no effect on measures of home cleanliness or the prevalence of physical amenities, such as outside sitting areas.
- Contrary to some expectations, extensive regulation was not associated with facilities having a very "institutional," less "homelike" environment.
3.3 Effect of Licensure
- Licensure had a positive effect on many of the measures that were also positively affected by extensive regulation. For example, licensed homes were more likely to have operators with training, to make more social aids and supportive devices available to residents, and to have greater staff knowledge of the ombudsman program.
- Licensure had a positive effect on measures that were not affected by extensive regulation, including the availability of key services and the prevalence of safety features.
- Licensure was effective in the area some observers argue is the main goal of regulation--raising homes above a minimum level of acceptable performance or "preventing" the worst performance. Thus, licensed homes were less likely to have the lowest scores on such measures as availability of social aids, physical amenities, safety features, and a low diversity/very institutional environment.
- Licensure had no effect on such measures as staff training and availability of licensed nurses.
3.4 Role of Board and Care Homes
- The niche for board and care homes appears to be different in States with extensive regulatory systems compared to States with limited systems.
- States with extensive regulatory systems have higher than average board and care bed supply and lower nursing home bed supply. States with limited regulatory systems have lower than average board and care home bed supply and higher nursing home bed supply.
- Homes in States with extensive regulation have residents with higher levels of disability than homes in States with limited regulatory systems.
- Thus, it appears that States with extensive regulatory systems were using board and care beds as substitutes for nursing home beds, particularly in comparison to States with limited regulatory systems.
| EXHIBIT 1. Summary of Effects of Regulation on Quality | ||
| Quality Indicator | Extensive Regulationa | Licensureb |
| Likelihood that most homes will be licensed | + | NA |
| Operator trained in care of elderly & disabled | + | + |
| Lower use of psychotropic drugs | +c | 0 |
| Lower rate of inappropriate drug prescriptions for elderly | +c | 0 |
| Staff knowledge of/referral to ombudsman program | +c | +d |
| Preventing low diversity/very "institutional" environment | +/-c | +d |
| Availability of social aids (e.g., working TV, radio) | + | +e |
| Availability of supportive devices (e.g., shower grab-bars) | +e | + |
| Preventing lowest scores on social aids (e.g., working TV, reading materials, card table, outside seating) | +/-e | + |
| Preventing lowest scores on supportive devices | +/-e | 0 |
| Preventing lowest scores on physical amenities | 0 | + |
| Preventing lowest scores on safety | 0 | + |
| Resident activity level | +e | - |
| Availability of key services (e.g., ADL assistance, special diets, activities) | 0 | + |
| Prevalence of safety features | 0 | + |
| Diverse "homelike" environment (e.g., smaller home size, personalization of rooms) | 0 | +d |
| Operator-required training for staff | 0 | 0 |
| Staff knowledge: basic care/monitoring/medication administration | 0 | 0 |
| Cleanliness and attractiveness of home | 0 | 0 |
| Home has amenities (e.g., comfortable chairs, plants, lamps) | 0/-e | 0 |
| Home has licensed nurses (RNs, LPNs) | 0 | 0 |
NA = Not applicable. + = The effect is positive, that is, in the direction of better quality. 0 = No association was detected. - = An effect is negative, that is, in the direction of worse quality.
|
||
SECTION 4: OVERVIEW OF STUDY METHODS
The study's principal objective was to evaluate the effect of regulation on the quality of care in board and care homes. The study used cross-sectional comparisons to examine the effects of extensive versus limited regulatory systems and licensure on the performance of homes.
State selection criteria included
- Content of regulations
- Nature of the inspection process
- Availability and use of a range of enforcement mechanisms or sanctions.
4.1 State Selection
If regulation does affect quality of care, the association would be most easily detected when comparing the extremes of the regulatory environment. Thus States were selected based on variations in their approach to regulating board and care homes. A group of experts that included providers, State licensing officials, long-term care ombudsmen who worked with board and care homes, and researchers identified key components of the regulatory system expected to have the greatest effect on the quality of care provided by homes. They cited key aspects of the licensing regulations (e.g., minimum staffing standards, provisions on residents' rights, requirements on training for operators), the inspection process (e.g., whether the surveys were unannounced, the makeup of the survey team, the frequency of inspections), and the availability and use of a range of enforcement mechanisms (e.g., bans on admission, fines, license revocation, and corrective action plans). Facilities then received points for the presence or absence of these features. States were rank-ordered along the regulatory continuum based on their total scores.
Study States
|
Twenty-one of the 50 States consistently fell into the "extensive" or "limited" extremes of the distribution on regulation, regardless of whether the scores for various elements were weighted for relative importance. From these 21 States, a purposive sample of 10 States was selected on the basis of factors such as the number of licensed homes, region, and the amount of State supplemental payments for beneficiaries of the Federal Supplemental Security Income (SSI) program who reside in board and care homes.2
4.2 Sampling of Licensed and Unlicensed Homes
Creation of the sampling frame for licensed homes involved identifying all the licensing agencies and programs in each State and the names of eligible homes. We excluded homes licensed for special populations (i.e., children, people in substance abuse treatment facilities) and homes licensed by departments of mental health or developmental disabilities, since their licensing standards and payment systems often differed from those of the agencies that licensed homes serving mixed populations or older persons.
To be eligible for the study, unlicensed homes had to provide:
- Room to 2 or more adults
- Meals
- Some type of 24-hour oversight or supervision
- One or more eligible services (e.g., transportation to medical appointments, medication reminders or storage, organized activities, or personal/ADL care).
The creation of a sample frame for unlicensed homes was complex. A probability-based sample of counties within the study States was selected. Within a subsample of these counties, a large number of local individuals knowledgeable about the existence of unlicensed homes were interviewed. They included ombudsmen, case managers, hospital discharge planners, mental health case managers, local licensure agencies, and building inspectors. Telephone book "yellow pages," newspaper advertisements, and national and local retirement directories were reviewed. In addition, data provided by the Social Security Administration were used to identify addresses at which two or more SSI recipients lived. "Nominees" were then screened by telephone to determine whether they met the basic criteria for inclusion as an unlicensed home.3
A probability sample of homes was selected from the list of homes that met the criteria for inclusion, stratified by whether they operated under an extensive or limited regulatory system, by licensure status (licensed/unlicensed), and by size (small, medium and large). From this home sample, random samples of residents and staff were selected.
4.3 Data Collection
During the late summer and fall of 1993, in-person interviews were conducted at the selected facilities. The site visits took approximately 1 day in small homes, 2 days in medium-sized homes, and 3 days in large homes. These site visits included:
- Interviews with operators in 512 homes--386 licensed and 126 unlicensed
- Interviews with 1,138 staff members
- Interviews with 3,257 residents
- A structured observation of the environment and care of residents.
4.4 Data Analysis
Our analytic approach focused on (1) determining whether regulation had an effect on the quality of care in board and care homes; and (2) describing the homes, operators, staff, and residents and the differences between them that were associated with the major factors of interest--licensure status and regulatory system type (extensive/limited). We analyzed the independent effects of extensive regulation and licensure and examined whether these effects were different for different types of homes. This strategy allowed the study to examine such issues as:
- Does extensive regulation affect both licensed and unlicensed homes similarly (e.g., does it have a halo effect on all facilities) or does it affect the performance of only those homes that are licensed?
- Does licensure affect small facilities differently than large facilities?
The quality measures included several facility measures (e.g., safety features, cleanliness), staff measures (e.g., training, knowledge of basic care procedures), and resident measures (e.g., satisfaction with food).
In examining the relationship between the regulatory system (extensive vs. limited), licensure, and quality of care, we used multivariate modeling techniques that control for multiple explanatory variables. A full description of the data analysis and detailed results are provided in the forthcoming report, Description of Board and Care Homes, Staff, and Residents.
4.5 Limitations of Study Design
The study design has several strengths, the most significant of which is that it enabled the categorization of States based on their regulatory system for board and care homes and the selection of States so as to maximize the likelihood of detecting any effect of regulation on quality. However, the design has some limitations as a result of its focus on assessing the effects of regulation and differences between licensed and unlicensed homes:
- First, the study does not attempt to determine what the quality of care is, that is,whether care in board and care homes across the country is excellent, adequate, or very poor. We know where it is "better" or "worse" but not what that means in terms of a normative or absolute standard.
- Second, the study was cross-sectional in design. With only one data collection point, we were limited in the quality measures we could assess. Such important measures as change in resident status (i.e., traditional outcome measures) were beyond the scope of this study. Thus, the study focused on a limited set of measures of structure and process quality. The study included measures of resident satisfaction or ratings of various aspects of the homes' performance; however, as with measures of residents' rights and autonomy and umet care needs, there was little variation across residents in their ratings. Thus, these measures were not useful in examining the effects of regulation.
- Third, measures of unmet care need relied on resident self-reports to identify need for more assistance or dissatisfaction with the quality of the assistance provided. Thus, we do not have comparable measures of unmet care needs for cognitively impaired residents for whom a proxy respondent was interviewed. Because cognitively impaired residents represent 40 percent of the study sample and because their impairment makes them most vulnerable to unmet care needs or poor care, this is a significant limitation.
- Fourth, the approach of selecting five States with limited regulatory systems and five with extensive regulatory systems meant that, although we could assess the relative effects on quality of extensive regulatory systems, we could not address the effects of the mid-range of regulatory environments.
SECTION 5: THE BOARD AND CARE ENVIRONMENT: CHARACTERISTICS OF HOMES AND RESIDENTS
This section discusses general characteristics of board and care homes and the residents who live there. Variations in these characteristics associated with differences in regulation and licensure status are discussed in Section 6 and Section 7.
5.1 Characteristics of Homes
The diversity among places known as board and care homes is striking. Homes ranged in size from 2 to more than 1,400 beds. Some homes had three or four residents sharing a room; others were private apartments. They ranged from family homes to parts of multilevel campuses that also had congregate apartments and a skilled nursing home. Rates ranged from less than $400 to more than $4,000 per month. Some offered little more than room, meals, oversight, and limited services; others provided or arranged for skilled nursing services and therapies. Homes also differed in the services that were included in their fees. In addition, resident mix differed among facilities. Some residents were cognitively intact but needed moderate assistance with meal preparation and transportation; others had dual diagnoses of mental retardation and developmental disabilities (MR/DD), and still others had indwelling catheters and needed daily nursing care.
5.1.1 Homelike vs. Institutional Settings
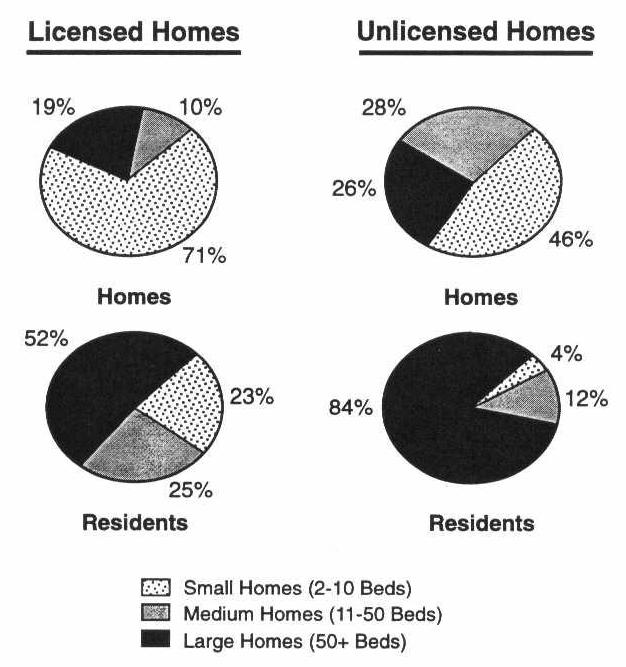
Board and care homes are thought of as less institutional than nursing homes. However, many homes lacked environmental features and practices that create a "homelike" or noninstitutional atmosphere. The widespread perception that board and care homes are small and thus more "homelike" is somewhat misleading, as depicted in Exhibit 2. Most residents lived in medium-sized (11 to 50 beds) or large homes (51+ beds). These larger unlicensed homes included apartment complexes, assisted living facilities, and retirement communities that provide meals, protective oversight, and some assistance with ADLs. (Unlicensed homes, including apartments, are discussed in detail in Section 7.)
Fifty-two percent of the residents in licensed homes and 84 percent of the residents in unlicensed homes lived in large homes (more than 51 beds).
In addition to size, many board and care homes had other features or policies not typically regarded as "homelike." Most homes had common areas, which included community rooms or living rooms and outside sitting areas; however, only 43 percent of the residents reported they had access to a kitchen to fix a snack, a cup of coffee, or a soft drink. Homes also differed as to whether residents were allowed to bring their own furniture or only a few possessions and whether the facility had a "homelike" or institutional appearance. Twenty-one percent of the homes were rated as having an institutional appearance and little variation or distinctiveness in furnishings, and 37 percent showed only "moderate distinctiveness," with furnishings varying from room to room but the overall design, wall coloring, and floor coverings showing little variation. Further, residents and the owner or operator (the onsite, day-to-day manager) ate all meals together in only 35 percent of the licensed homes and in 25 percent of the unlicensed homes. Only 22 percent of the residents reported being completely free to decide when to eat a meal, and 38 percent of the residents reported that they were not allowed to do chores around the home.
| EXHIBIT 2. Distribution of Board and Care Homes and Residents by Home Size |
 |
5.1.2 Facility Resident Mix
Board and care homes also differed in their mix of residents. As displayed in Exhibit 3, most homes housed a predominantly elderly population. Other homes housed primarily persons with mental, emotional or nervous conditions, including persons with MR/DD, and some homes had a mix of elderly disabled and persons with chronic mental illness and MR/DD.
For all board and care homes, the resident mix was quite complex in terms of disability levels and the need for protective oversight and services. Approximately three-quarters of the homes reported having one or more residents with cognitive impairment. Slightly more than half the homes (57 percent) had residents with a diagnosis of mental illness or a prior stay in a psychiatric hospital. One-third had residents with MR/DD.
| EXHIBIT 3. Board and Care Home Resident Case Mix by Facility Type | |||
| Resident Case Mix | Unlicensed Homes | Licensed Homes (%) | |
| Apartments (%) | Other (%) | ||
| Predominantly elderly residents (>90%) | 83 | 35 | 56 |
| Predominantly residents with mental conditions (>90%) | 3 | 45 | 21 |
| Mixed resident population | 14 | 20 | 23 |
Board and care homes also coped with other complex care problems. Forty-two percent of homes had one or more residents with alcohol abuse problems, and 15 percent said they had residents with drug abuse problems. Some homes also housed residents with significant health problems and functional impairments. About one-third of the homes reported having one or more residents who were bedfast or chairfast because of health problems, and 59 percent of the homes reported having residents with urinary incontinence.
5.1.3 Supportive Services
Board and care homes offered a wide range of services, as shown in Exhibit 4. More than three-quarters of the homes reported providing medication storage or supervision, organized activities, recreational trips, and transportation. Ninety-two percent of licensed homes and 62 percent of unlicensed homes provided personal care, such as assistance with bathing or other ADLs. Nearly 40 percent of licensed homes and 45 percent of unlicensed homes reported providing money management to one or more residents. However, approximately 66 percent of the residents who received any help reported that family members managed their money, indicating that relatively few residents availed themselves of this facility service.
| EXHIBIT 4. Services Provided by Homes | ||
| Services Provided | Licensed Homes (%) | Unlicensed Homes (%) |
| 3 meals a day | 97 | 90 |
| ADL assistance | 92 | 62 |
| Medication storage or supervision | 99 | 76 |
| Organized activities | 88 | 81 |
| Recreational trips | 80 | 75 |
| Transportation | 89 | 87 |
| Nursing care (RN/LPN) | 25 | 27 |
| Money management | 39 | 45 |
5.1.4 Payer Mix, Rates, and Services Included in Monthly Rate
Homes differed in terms of payer mix, average monthly rates, and the services that were included in the monthly rate. There are two primary payers for board and care: private payments by residents or their families and public payments through the Federal Supplemental Security Income (SSI) program and State Supplemental Payments (SSP).4 One of the key differences among facilities, then, is the proportion of residents whose care is paid for by SSI/SSP, as shown in Exhibit 5.
| EXHIBIT 5. SSI/SSP Payer Mix and Monthly Rate by Facility Type | |||
| Proportion of Residents with SSI/SSP as the Payer | Unlicensed Homes | Licensed Homes (%) | |
| Apartments (%) | Other (%) | ||
| <20% | 93 | 53 | 39 |
| 20%-80% | 6 | 25 | 38 |
| >80% | 2 | 23 | 23 |
| Average Monthly Rates | |||
| Mean Private Pay Rate | $1,070 | $992 | $1,208 |
| Mean SSI/SSP Rate | $436 | $481 | $689 |
These two primary payers have very different average payment levels for board and care, as shown in Exhibit 5. Exhibit 6 displays ranges of rates for both SSI/SSP and private pay rates and the percentage of homes whose average monthly rate falls in each category. As shown, an estimated 85 percent of all public payments (SSI and SSP) were less than $800 per month in 1993. By comparison, 74 percent of the private pay rates were higher than $800 per month.
Licensed homes tend to include a wider array of services in their monthly rate than do unlicensed homes. In licensed homes, these monthly rates generally covered room, board, personal laundry, special diets, and assistance with ADLs. However, in about one-fifth of the licensed homes, there was an additional charge if the resident needed a special diet or personal assistance with eating, dressing, and toileting (see Exhibit 7). Among unlicensed homes, only 57 percent included special diets in their rate, 65 percent covered personal laundry, and only 71 percent included ADL assistance in the monthly charge. Three-quarters of all homes charged extra for incontinence supplies.
| EXHIBIT 6. Distribution of Monthly SSI/SSP and Private Pay Rates | ||
| Monthly Rate | Homes Receiving SSI/SSP (%) | Homes Charging Private Rate (%) |
| < $500 | 25 | 6 |
| $501-$650 | 32 | 6 |
| $651-$800 | 28 | 14 |
| $801-$1,200 | 9 | 29 |
| $1,201-$1,700 | 3 | 32 |
| $1,701-$1,950 | 1 | 7 |
| > $1,951 | 2 | 6 |
5.1.5 Services from External Agencies
According to the operators, few homes (18 percent of licensed homes and 27 percent of unlicensed homes) have a formal arrangement or contract with a home health agency. Despite this, residents received services from outside agencies. About half the homes (53 percent) reported that outside agencies provided temporary or episodic nursing care to residents. In addition, 25 percent of the licensed and 33 percent of the unlicensed homes reported that agencies provided ADL assistance/personal care to residents. In 40 percent of homes, therapy services were provided to residents by outside providers.
Approximately one-third also reported that some residents attended senior centers, adult day care programs, sheltered workshops, or day activity programs.
| EXHIBIT 7. Services Covered by Monthly Rate | ||
| Services | Licensed Homes (%) | Unlicensed Homes (%) |
| Personal laundry | 93 | 65 |
| Incontinence supplies | 26 | 26 |
| Special diets | 81 | 57 |
| ADL assistance/personal care | 82 | 71 |
5.1.6 Nursing Care
Facilities differed in their willingness and ability to provide or arrange for daily nursing care for residents. Approximately 21 percent of all homes provided nursing services with registered nurses (RNs) or licensed practical nurses (LPNs) who worked full or part time in the home. If a resident needed only temporary nursing care (some daily care/monitoring by an RN or LPN for less than 14 days), only 42 percent of licensed homes and 21 percent of unlicensed homes reported that they provided services with facility staff or arranged for a home health agency to provide care. However, 58 percent reported they would choose some other option. For example, 21 percent of the licensed homes and 37 percent of the unlicensed homes reported that they sent the resident to a hospital/emergency room if the resident became ill and needed temporary nursing care. If a resident needed nursing care for more than 14 days, only 18 percent of the homes reported that they would provide care with facility staff or arrange for a home health agency to provide the care. Forty-four percent of the licensed homes and 56 percent of the unlicensed homes reported they would discharge such a resident to a hospital (acute care or VA) or a nursing home.
5.1.7 Quality of Care
Staffing patterns, staff training, staff knowledge, and some care practices raise some concerns about the quality of care. Nearly 20 percent of the operators in licensed homes and 33 percent in unlicensed homes reported that they did not require training for staff. Of those that required training, only 23 percent of licensed homes and 15 percent of unlicensed homes required staff to complete all training before they began providing resident care.
Forty-one percent of board and care residents received one or more psychotropic drugs.
One major area of concern relates to staff qualifications and their supervision or administration of medications in board and care homes. As noted in Exhibit 4, 99 percent of the licensed homes and 76 percent of unlicensed homes reported providing medication storage or supervision. In addition, as shown in Exhibit 8, 71 percent of the residents reported receiving assistance with medications and 41 percent were taking psychotropic drugs. However, only 21 percent of the homes had any licensed nurse on staff. This included full or part-time nursing staff and RNs as well as LPNs or licensed vocational nurses (LVNs).
| EXHIBIT 8. Comparison of Residents | |||
| Measure | Board and Care | Nursing Home | |
| 1983 DRI Studya (%) | 1993 ASPE Studyb (%) | HCFA 93c (%) | |
| Aged 75+ | 38 | 64 | 81 |
| Cognitively impaired | 30 confused | 40 | 66 |
| Mental/psych condition | 33 | 33 | 17 |
| MR/DD | 11 | 11 | 13 |
| Urinary incontinence | 7 | 23 | 64 |
| Bedfast or chairfast | 2 | 7 | 13 bedfast |
| Wheelchair | 3 | 15 | 53 |
| Help bathing | 27 | 45 | 97 |
| Help eating | NA | 5 | 72 |
| Help taking medications | 43 | 75 | 100 |
| Taking >1 psychotropic | 34 | 41 | 27 |
MR/DD = Mental retardation/developmental disabilities. NA = Not available.
|
|||
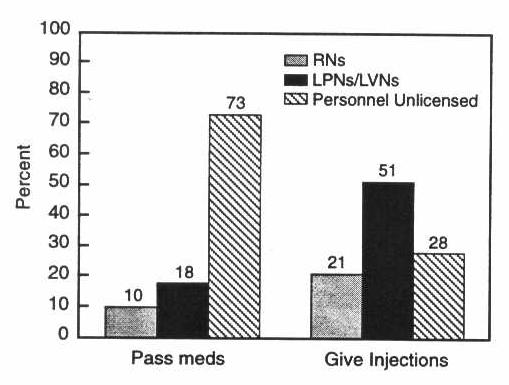
Seventy-three percent of staff who reported passing medications were not licensed nurses (RNs, LPNs); and 28 percent of staff giving injections were not licensed nurses.
As shown in Exhibit 9, 73 percent of the staff who reported passing medications were not licensed nurses, although only one study State (Oregon) had a program for training and certifying nursing assistants to pass medications. Only 18 percent of staff who passed medications reported being LPNs or LVNs. Only 10 percent were RNs. Further, 26 percent of the non-nursing staff passing medications reported they received no training on medication supervision or management. Of staff who reported giving injections to residents, only 21 percent were RNs, and 51 percent were LPNs/LVNs. More troubling, 28 percent of the staff giving injections were unlicensed staff.
| EXHIBIT 9. Board and Care Staff Who Administer Medication |
 |
The relatively limited staff knowledge of care practices and monitoring is also troubling. Staff were tested on their knowledge of what signs are part of "normal aging" and how to handle hypothetical cases (e.g., new onset of incontinence, chest pain). Those who passed or administered medications to residents were also tested on correct procedures and recognition of signs and symptoms of adverse reactions. Only 14 percent of the operators and staff scored 76 percent or higher (out of a possible score of 100 percent). And 39 percent of the staff provided correct answers for half the questions or fewer.5
5.2 Characteristics of Residents
The population of 3,257 residents in the study sample was overwhelmingly elderly (78 percent), female (66 percent), Caucasian (91 percent), and widowed, divorced, or never married (85 percent). Further, in terms of age, cognitive impairment, and functional status, they were more impaired than the residents described in studies conducted during the 1980s and significantly less impaired than nursing home residents, as shown in Exhibit 8.
5.2.1 Age
Only 22 percent of the residents in this study were non-elderly (age 18 to 64). Indeed, 64 percent of the residents were age 75 or older. This study's residents were older than those described in board and care studies from the early- to mid-1980s. The DRI study in the early 1980s found that only 38 percent of the residents were 75 or older in the "elderly/mixed" homes in five States (Dittmar and Smith, 1983). In another study of board and care homes in the early 1980s, Sherwood and her colleagues excluded non-elderly residents but found only 42 percent of the residents were 75 or older (Mor et al., 1986).
5.2.2 Mental Status and Cognitive Impairment
Excluding Alzheimer's and other dementias, the number of residents with psychiatric conditions was about the same as in the 1980s, with one-third of the residents in this study, like the DRI study, reporting a mental, emotional, or nervous condition. Similarly, the percentage of residents with a diagnosis of mental retardation or developmental disabilities (about 10 percent) is essentially the same. DRI reported "confusion" among residents rather than measuring cognitive impairment and found 30 percent of the residents were confused. Sherwood and colleagues (1981; Mor et al., 1986) found that 24 percent were cognitively impaired, compared to this study's finding that 40 percent of the residents had moderate to severe cognitive impairment.
5.2.3 Functional Impairments
The study also found significant levels of functional impairment among residents (Exhibit 8). Twenty-three percent had urinary incontinence, 7 percent were bedfast or chairfast (in their rooms 22+ hours per day) because of a health problem, and 15 percent used a wheelchair as a primary mode of locomotion. Forty-five percent of the residents received bathing assistance from another person; 20 percent received hands-on assistance with dressing; and 9 percent received assistance with locomotion. Nearly 12 percent of the residents received help from another person in performing three or more activities of daily living (ADLs included bathing, dressing, locomotion, toileting, transferring, and eating).
The impairment among residents in this study is much higher than the levels found by Dittmar and Smith (1983) in the DRI study and by Sherwood and her colleagues in their study (Mor et al., 1986; Sherwood et al., 1981). For example, these earlier studies found only 7 percent of the residents had urinary incontinence. Similarly, Dittmar and Smith (1983) found only 2 percent of the residents in the elderly/mixed homes were bedfast or chairfast, 3 percent used a wheelchair, 27 percent received help in bathing, and 43 percent received help with medications. The rates of psychotropic drug use were also higher in 1993.
5.3 Niche Served by Board and Care Homes
Board and care homes fit in the "niche" between other residential settings (e.g., congregate apartments) and nursing homes. Moreover, although there is overlap, board and care homes provided a distinct service compared to these other settings.
In terms of services, board and care homes provided more care and services than congregate apartments with supportive services and boarding houses (Griffith, 1995). However, even with the addition of services provided by home health agencies, visiting nurses, and others, the average board and care home provided fewer skilled and rehabilitative services; less routine monitoring, assessment, and care planning; and less nursing and restorative care than nursing homes. Only 21 percent of the board and care homes had a full-or part-time RN or LPN on staff. And 82 percent of the board and care homes, were unable or unwilling to provide nursing services to a resident for an illness that lasted longer than 14 days. Moreover, 21 percent of the licensed homes and 37 percent of the unlicensed homes reported being unable to handle a resident's illness that necessitated even a temporary need for nursing care.
In general, board and care home residents are more impaired than residents of other settings in which residents receive meals and services, such as congregate apartments. In a current study of the Congregate Housing with Services Program (CHSP) for the U.S. Department of Housing and Urban Development (HUD), for example, preliminary data suggest that fewer than 7 percent of the residents have impairments in one or more basic ADLs, compared to 45 percent of board and care home residents (Griffith, 1995).
Twelve percent of board and care residents were dependent in three or more ADLs and 40 percent had moderate to severe cognitive impairment. Thus, there is some overlap with the nursing home population.
Compared to nursing home residents, however, board and care home residents are much less impaired, on average. Using data collected during the same time period as the ASPE data collection (summer 1993) for approximately 2,100 nursing home residents in 10 States, we found that nursing home residents were older and more impaired than the board and care home residents in cognition, ADLs, and other areas of functioning, as shown in Exhibit 8 (Hawes et al., 1994; Phillips et al., 1994). For example, 65 percent of nursing home residents received assistance in locomotion, whereas only 9 percent of board and care residents received such assistance. As shown in Exhibit 8, 72 percent of nursing home residents received hands-on assistance or supervision in eating, while only 6 percent of the board and care residents received such assistance. Nearly two-thirds of the nursing home residents had urinary incontinence, while only 23 percent of the board and care residents were incontinent. Approximately two-thirds of the nursing home residents had moderate to severe cognitive impairment, while 40 percent of the board and care residents were similarly impaired.
There does appear to be some overlap between the nursing home population and the board and care home population in terms of ADLs and cognitive impairment. For example, as shown in Exhibit 10, 12 percent of the board and care residents received assistance in three or more ADLs, which is often the criterion for nursing home placement or eligibility. Further, 40 percent of the board and care residents are cognitively impaired (Exhibit 8). However, the vast majority of nursing home residents (more than 70 percent) received assistance with three or more ADLs. Thus, while the amount of overlap in resident characteristics between board and care homes and nursing homes is likely to vary from State to State, on average in the 10 study States, the amount of overlap was relatively small.
These data show that most board and care homes have a definite long-term care niche. The services they provide and the residents they serve align them more closely with nursing homes than with such residential settings as boarding homes or congregate apartments, even those with enriched support services. On the other hand, few board and care home residents are as impaired as the average nursing home resident, and, in most board and care homes, the services are far less skilled or intense than in the average nursing home.
| EXHIBIT 10. Level of ADL Impairment by Cognitive Impairment Level in Board and Care Home Residents | ||||
| ADL Assistance Receiveda | Cognitively Intact (%) | Moderate Cognitive Impairment (%) | Severe Cognitive Impairment (%) | Total by ADL Status (%) |
| In 0 ADLs | 40 | 8 | 4 | 52 |
| In 1-2 ADLs | 19 | 8 | 8 | 36 |
| In 3+ ADLs | 2 | 2 | 8 | 12 |
| Total for Cognitive Status | 61 | 19 | 20 | 100 |
|
||||
SECTION 6: EFFECT OF REGULATION AND LICENSURE ON QUALITY OF CARE
Prior studies (Dobkin, 1989; GAO, 1989; U.S. DHHS, Inspector-General, 1990) found four basic domains on which States' regulatory systems varied:
- Licensing standards--the type of residents a home could accept and must discharge, standards for staffing ratios, training, residents' rights, and the number of beds and services a home could provide without being licensed
- Inspection processes--how often homes were inspected, whether the inspections/ surveys were unannounced, and the makeup and training of the survey team or inspector
- Range of enforcement remedies that were available and used
- Resources available to supplement the payment of SSI for board and care residents who were poor and aged, blind, or disabled.
Prior research suggested that State regulation of board and care homes was inadequate and ineffectual (Dobkin, 1989; Hawes et al., 1993; Reichstein and Bergofsky, 1983; Sherwood and Seltzer, 1981; Stone and Newcomer, 1985). Empirical findings about the positive effects of regulation were largely limited to such features as fire protection and safety (Dittmar and Smith, 1983; Mor et al., 1986; Reschovsky and Ruchlin, 1993). Thus, Reschovsky and Ruchlin (1993) argued that "overall, governmental regulatory policies did not significantly affect board and care home quality."
Prior studies found that regulation had little or no effect on quality other than to improve the fire safety in board and care homes.
The current study has several advantages over prior examinations of the effect of regulation on quality in board and care homes. First, the study was designed to facilitate an effective evaluation of regulation. It drew on substantial work by the DHHS Inspector General and the American Association of Retired Persons (AARP) to identify variations among States on a number of key dimensions of regulation (Hawes et al., 1993; U.S. DHHS, 1990). This allowed us to rank the States on a presumed continuum of regulatory systems from "limited" to "extensive." Second, prior studies involved fewer States (e.g., five in the previous DRI study for ASPE) and did not have a comparable method for selecting States with the maximum possible variation in regulatory systems. Third, the study's probability sample allowed for generalization across States with extensive and limited regulatory systems. Fourth, this study examined a broader range of quality measures. Thus, although the one-time data collection precluded the possibility of examining resident outcomes, this study was able to identify and examine a variety of measures of structural and process quality.
This section describes the results of the multivariate models used to examine the effect of the nature of the regulatory system (extensive vs. limited) and of licensure on board and care home quality. A more detailed description of the analytic strategy and statistical results is presented in the forthcoming technical report, The Effect of Regulation on the Quality of Care in Board and Care Homes.
This study found positive effects of regulation on safety, quality of life, and quality of care.
6.1 Effect of Regulatory System on Quality
The study's primary goal was to determine whether more extensive regulatory systems were associated with better quality of care. Thus, the primary comparison was between the quality in homes operating in States with more extensive regulatory systems and in homes in States with more limited regulatory systems.
6.1.1 Prevalence of Unlicensed Homes
The study's first finding is that States with extensive regulatory systems are much more likely to have most of their homes licensed. In States with extensive regulation, only 7 percent of the total supply of board and care homes are unlicensed. In States with limited regulatory systems, an estimated 25 percent of all homes are unlicensed. Thus, the positive effects of licensure are indirectly associated with extensive regulation.
6.1.2 Operator Education, Training, and Experience
The operator is the day-to-day manager of the facilities and, as such, directs the staff and determines both the quality of the environment and the care provided to residents. Operators of homes in States with extensive regulation were more likely to have received training in the care of the elderly and disabled before they began operating a board and care home. They also tended to have more education and prior experience providing health care.
6.1.3 Lower Use of Psychotropic Drugs and Use of Fewer Contraindicated Medications
Residents of licensed homes in States with more extensive regulation had lower use of psychotropic medications. Although these medications have beneficial effects for many persons, their inappropriate use can be devastating. Moreover, because of the lack of licensed nurses to monitor residents' reactions to psychotropics in board and care homes, widespread use among residents has been a particular concern (Avorn et al., 1989; GAO, 1992a; 1992b; Harrington et al., 1994; Hartzema et al., 1986). Thus, the lower use of psychotropics among residents in extensively regulated States, even when controlling for differences in resident characteristics across the States, is a significant beneficial effect. Residents in licensed homes in States with extensive regulatory systems were also less likely to be receiving medications that are contraindicated for use with the elderly (Beers et al., 1991; Spore et al., 1995; Stuck et al., 1994).
6.1.4 Prevention of Very Poor Performance
It is widely argued that regulation may be limited in its ability to ensure homes provide the "best" quality, but that it can prevent the "worst" quality. This study examined the likelihood that extensive regulation would be associated with preventing homes from being in the bottom rank of scores (the bottom 20 percent) on a variety of quality measures. Extensive regulation was positively associated with several such effects:
- Extensive regulation was associated with preventing licensed homes from having a very institutional environment. These homes were less likely than licensed homes in States with limited regulation to have few or no personal possessions in residents' rooms and little diversity in the style and color of furniture throughout the facility, factors associated with a more institutional environment.
- Small and medium-sized homes that were extensively regulated were less likely to score at the bottom on the availability of social and recreational aids, such as a working television, radio tape/CD player, reading materials, and outside sitting area. The availability of such aids is considered important to residents' ability to choose among activities and have a decent quality of life (Moos and Lemke, 1978).
- Small, extensively regulated homes were less likely than small homes in States with limited regulation to have the lowest scores on the availability of supportive aids and devices, such as shower grab-bars, grab-bars by the toilet, and call buttons.
6.1.5 Availability of Social Aids and Supportive Devices
Extensive regulation was also associated with homes having higher scores on the availability of social aids and supportive devices. Thus, extensively regulated homes were more likely to have a wide range of such social aids as a working television, radio, reading materials, card tables, and outside sitting area. Extensively regulated small homes made a wider range of supportive devices available to residents.
Regulation was effective in promoting higher quality of care, not merely in preventing the worst performance.
6.1.6 Staff Knowledge of Ombudsman Program
Staff in licensed homes in States with extensive regulation were much more likely to know the name and phone number of the ombudsman. They were also more likely to call an ombudsman and more likely to refer families or residents to an ombudsman if a problem occurred.
6.1.7 Resident Activity Level
Residents in large, extensively regulated homes were more likely to have greater levels of involvement in activities, a wider range of activities, and greater satisfaction with activities outside the home than residents in large homes in States with limited regulatory systems. The effect was apparent only in large homes and had no effect on small and medium-sized homes.
6.1.8 No Effect
Extensive regulation had no effect on several measures: preservice training, staff knowledge, the availability of licensed nurses (RNs or LPNs) on the home's staff, cleanliness and attractiveness, and physical amenities. In addition, extensive regulation had no effect on availability of services, the prevalence of safety features, and prevention of low scores on safety and physical amenities, although licensure had a positive effect on these measures.
Staff Knowledge of Care and Monitoring. We evaluated the effects of regulation on staff knowledge of signs that are part of normal aging and how to handle hypothetical cases (e.g., new onset of incontinence). In addition, those who passed or administered medications to residents were tested on correct procedures and recognition of signs and symptoms of adverse reactions. None of the differences in staff knowledge were associated with either the licensure status of the home or whether it was extensively regulated, with one exception. Staff in large unlicensed homes (mainly the apartment-only facilities) had better scores on the "normal aging" items. They also had a resident population that, while mainly elderly, was relatively unimpaired.
Availability of Licensed Nurses on Staff. The only factor associated with having licensed nurses on staff was home size, with small homes being unlikely to have such staff.
Cleanliness, Attractiveness, and Physical Amenities. The factor associated with better quality on these measures was whether the home was an "apartment-only" facility. These facilities are very different from other board and care homes. They have a higher private-pay mix, few or no SSI recipients, and a more homogeneous set of residents (i.e., mostly elderly and less impaired than residents in licensed and extensively regulated homes). Moreover, most are unlicensed and operate in States with limited regulatory systems. Given their location, resident case mix, and payer mix, it is unlikely that regulation alone would change the fact that these places tend to be cleaner, more attractive, and have more physical amenities.
6.2 Effect of Licensure on Quality
The study also examined the effects of licensure on quality, comparing the performance of homes that were licensed to those that were unlicensed. As noted above, since a greater proportion of facilities in States with extensive regulation are licensed, the regulatory system can be seen as having an indirect effect on facilities by changing the likelihood that they will be licensed.
The measures on which licensure had a positive effect are summarized in Exhibit 1 and include a wide array of structural and process quality indicators. Two main types of effects were found: preventing poor performance and promoting better performance.
6.2.1 Prevention of Very Poor Performance
Licensure was effective in preventing homes from having the worst performance along important dimensions of quality. As noted earlier, one of the main roles of regulation is to raise the performance of facilities above certain minimum levels and, in this, licensure is largely effective. Compared to unlicensed homes, licensed homes were less likely to have the lowest scores on the availability of safety features, such as smoke detectors, a fire extinguisher in the kitchen, secure handrails at all stairways, and non-skid surfaces on stairs. Licensed homes were also less likely to have the lowest scores on physical amenities, such as the availability of comfortable furniture, table and floor lamps, and adequate sheets and towels. Licensed homes were less likely to have very low scores on diversity, such as personalization of residents' rooms and diversity in the furniture, wall colors, and floor coverings throughout the facility. Thus, they were less likely to have an "institutional" look. And, licensed homes in extensively regulated States were less likely to have the lowest scores on availability of social aids, such as a working television and radio/cassette player, card tables, reading materials, and outside sitting areas. This is particularly important, since many observers fear that regulation leads to a more "institutional," less homelike environment in board and care homes (Eckert et al., 1987; Reisacher, 1985). However, according to criteria developed by Moos and Lemke (1978), licensed homes do not have more "institutional," less homelike environments. This includes a combination of preventing an "institutional" look and low diversity with preventing low scores on physical amenities and the availability of social aids.
6.2.2 Promoting Better Performance
Licensure was also successful in helping facilities perform better in several key areas: operator training, safety, availability of services and availability of supportive devices. Licensed homes are more likely than unlicensed homes to have an operator who was trained in the care of the elderly and disabled prior to operating a board and care home. In addition, licensed homes had higher scores on safety features. They also had higher scores on the availability of supportive devices, such as grab-bars in the showers and by toilets. Licensed homes were also more likely to make key services available to residents, such as personal care and assistance with ADLs, nursing care, special diets, and transportation to medical and dental appointments and recreational activities.
Licensure had a positive effect in large homes for the prevalence of social/recreational aids. Similarly, licensure had a positive effect only in homes in States with extensive regulation for (1) staff knowledge of the ombudsman program; (2) preventing homes from having a very institutional environment; and (3) increasing the diversity and "homelike" qualities of the environment, such as personalization of room and smaller home size.
6.2.3 No Effect
On a number of measures, there was no statistically significant difference between licensed and unlicensed homes. These measures included staff preservice training, staff knowledge, amenities, availability of licensed nurses on staff, residents' need for assistive devices, and use of psychotropic drugs. For the last measure, extensive regulation had a positive effect (see Section 6.1.3).
6.3 Conclusion
Compared with prior studies of the effect of regulation (Dittmar and Smith, 1983; Reichstein and Bergofsky, 1983; Reschovsky and Ruchlin, 1993), this examination of regulation found more consistent and widespread positive effects on quality in board and care homes.
Safety. Like the other studies, this study found that regulation had a positive effect on the safety of the resident's environment. Licensure not only made it less likely that licensed homes would have the lowest scores on safety features, it also made it more likely that licensed homes would have a wider array of the safety features and supportive devices considered important by residents and others who study the ability of a facility to meet the needs of frail and disabled individuals (Moos and Lemke, 1978).
Quality of Life. This study found a consistent pattern with respect to many of the features that promote quality of life for residents. These include avoiding an institutional environment with little diversity and providing social and recreational aids and amenities. Homes in States with extensive regulatory systems and licensed homes performed better on these aspects of quality than their counterparts.
Quality of Care. Several factors suggest that homes in States with extensive regulation and homes that are licensed are better prepared to cope with the disability levels and potentially changing needs of residents who are clearly older and more impaired than residents were during the 1980s. These include: (1) greater availability of supportive services in licensed facilities; (2) greater operator training in care of the elderly and disabled; and (3) lower use of psychotropic drugs and medications contraindicated for use in the elderly in extensively regulated homes.
SECTION 7: EFFECT OF REGULATION ON SUPPLY AND CHARACTERISTICS OF BOARD AND CARE HOMES
One of the first effects we see of extensive regulatory systems is in the nature and number of board and care homes. This section presents data on the total number of licensed homes across the country, their distribution across the study States, and characteristics relevant to their role in providing long-term care. It also reports estimates on the number of unlicensed homes in the study States, describes characteristics of the homes, including the "apartment-only" facilities, and discusses the association between regulation and the prevalence of unlicensed homes.
There are an estimated 34,090 licensed board and care homes with more than 600,000 beds.
7.1 Licensed Homes
Study findings suggest that States with extensive regulation have a larger supply of licensed board and care home beds, fewer unlicensed homes, and a lower supply of nursing home beds. In addition, homes in States with extensive regulatory systems have residents who tend to be older and more disabled than residents in States with limited regulatory systems.
7.1.1 Supply of Licensed Board and Care Homes and Beds
Licensed homes are not evenly distributed across the States. In 1990, the number of licensed homes serving a primarily older population ranged from a low of 24 homes in Wyoming to more than 4,000 facilities in Michigan and California. Total beds ranged from a reported low of 195 beds in West Virginia to more than 60,000 in Florida and 90,000 in California (Hawes et al., 1993). These variations were associated with differences in the population age 65 and older among States. However, data from the current study suggest that variations in supply may also be associated with policy differences about the role or niche of licensed board and care in providing residentially based long-term care.
States have a variety of options for meeting the needs of the elderly and disabled for residential long-term care. One option is board and care homes. Another option is nursing homes. We used data from other studies on nursing home and board and care home supply and analyzed the differences between States we identified as having extensive or limited regulatory systems.
Although we selected only five States with extensive regulatory systems and five States with limited systems for the main study, we initially identified 12 States with extensive and 12 States with relatively limited regulatory systems. For these, we collected data on the supply of licensed board and care home beds and the supply of nursing home beds. First, we compared them to the national supply of beds.
In 1990, the average number of licensed board and care home beds in the United States serving an elderly/mixed population was 16 per 1,000 elderly (Hawes et al., 1993). As shown in Exhibit 11, among the 12 States initially identified as having limited regulatory systems, the average licensed board and care bed supply was 7 beds per 1,000 elderly, less than half the national average. Among the 12 States initially identified as having extensive regulatory systems, the rate was 20 beds per 1,000 elderly, or 25 percent higher than the national average. The ratio of nursing home beds to elderly persons was reversed; that is, States with extensive regulatory systems for board and care had lower supplies of nursing home beds.
| EXHIBIT 11. Nursing Home and Licensed Board and Care Home Bed Supply, 1989-1990 |
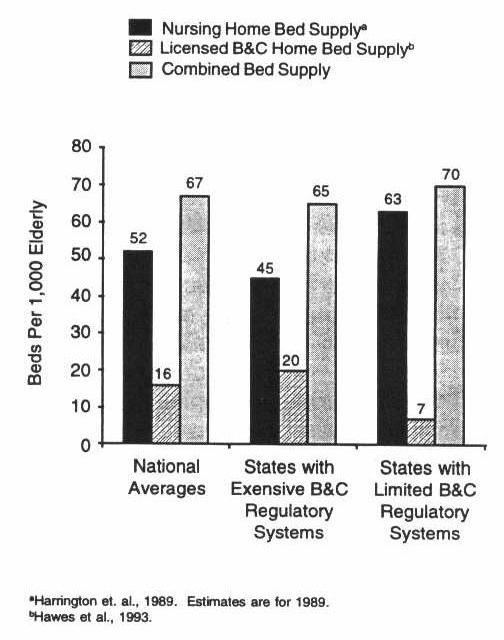 |
The total combined bed supply (nursing home plus licensed board and care home beds) of States with extensive and limited regulatory systems was similar to the national average of 67 beds per 1,000 elderly (i.e., 65 and 70, respectively). However, the States with more extensive regulatory systems had much greater reliance on board and care home beds to provide residential long-term care. States with extensive regulation had nearly three times the rate of board and care home beds per 1,000 elderly (20 beds vs. 7) compared to States with limited regulatory systems (Harrington et al., 1989, Hawes et al., 1993).
States with extensive regulatory systems had much greater reliance on board and care home beds to provide residential long-term care.
7.1.2 Characteristics of Licensed Board and Care Homes
Resident Case Mix. On average, board and care residents in licensed homes in extensively regulated States were almost 7 years older than their counterparts in States with limited regulation. In addition, residents were more likely to be physically impaired (bed and chairfast), cognitively impaired, incontinent, and impaired in multiple ADLs than residents of homes in States with limited regulatory systems. Residents in homes in States with limited regulation were more likely to have behavior problems, a psychiatric history, or MR/DD. These data suggest a different role for board and care homes between the two types of States. In States with extensive regulatory systems, the lower nursing home bed supply combined with a more impaired population of residents suggests the possibility of substitution of board and care for nursing home care for elderly persons with some cognitive or ADL impairment. States with limited regulatory systems, on the other hand, seem less inclined to substitute board and care for nursing home care, based on the relative ratio of board and care beds to nursing home beds, as shown in Exhibit 11.
- Are older
- Are bedfast or chairfast
- Are cognitively impaired
- Have urinary incontinence
- Have multiple ADL impairments.
Availability of Services. Despite having more impaired residents, homes in States with extensive regulatory systems were not more likely to have licensed nurses on staff. In addition, extensive regulation had no effect on the availability of supportive services, such as ADL assistance, therapies, or special diets.
7.2 Unlicensed Homes
This section discusses key findings about the distribution and characteristics of unlicensed homes. It finds that they are less likely in extensively regulated States, as shown in Exhibit 12, and that their basic character has changed since the 1980s with the emergence of a new type of home that contains apartments but provides meals, protective oversight, and supportive services to residents.
7.2.1 Supply of Unlicensed Homes
There are two types of unlicensed homes. The first type operates as a legally unlicensed board and care home. In some States, the size of certain homes (e.g., fewer than five or six beds) or the services provided (e.g., no ADL care) exempted them from mandatory licensure under State regulations. In addition, as of 1990, about half the States did not require board and care home licensure for facilities consisting only of apartments, regardless of their size or the services they offered (Hawes et al., 1993). Thus, there are many types of facilities, large and small, that provide meals, protective oversight, and services (like licensed board and care homes) but that are legally unlicensed. In addition, there are illegally unlicensed homes that meet the State's criteria for the type of facility that requires a license but has avoided licensure.
| EXHIBIT 12. Comparison of Proportion of Licensed to Unlicensed Homes |
 |
After surveying these homes to determine whether they met study criteria for an unlicensed home, we estimated a total of 1,555 unlicensed homes operating in the 10 study States in the fall of 1993, with an upper bound of 2,052 unlicensed homes. When combined with the estimates for the licensed homes, this produced a total board and care home population in the 10 States of 13,189 homes with more than 300,000 beds. Unlicensed homes accounted for less than 12 percent of total homes and about 27 percent of the total beds in the 10 study States.
7.2.2 Characteristics of Unlicensed Homes
A new type of unlicensed home has emerged during the past 10 years. Previous studies found only small unlicensed homes (Eckert et al., 1987; Mor et al., 1986; Reisacher, 1985). We found, however, that, on average, unlicensed homes were larger than licensed homes. The average size of unlicensed homes was 52 beds compared to 19 beds for licensed homes. The difference in size is directly attributable to the inclusion of facilities that provided relevant services and oversight but that housed residents in apartments. In many States, these were classified as "assisted living facilities" and were not required to be licensed as a board and care home. These facilities have become a significant segment of the industry. In the 10 study States, facilities that were apartments accounted for a third of all unlicensed homes and more than 80 percent of all unlicensed beds.
Apartment-only board and care homes were quite different from other facilities, both licensed and unlicensed. They were very large, with an average size of 138 beds. In addition, they were largely unlicensed. Of the 45 apartment-only facilities in the study, only 9 were licensed. When weighted to represent the estimated population in the 10 study States, 76 percent of the apartment-only facilities were not licensed as board and care homes. Further, apartment-only facilities were a much smaller proportion of all homes in States with extensive regulation, where they constituted 4 percent of the total homes, compared to 18 percent of the total homes in States with limited regulatory systems. Finally, as noted in Section 6 and in Exhibit 3 and Exhibit 5, the apartment-only facilities differed from other homes in resident case mix and payer mix. Eighty-two percent of the apartment-only facilities had a resident population that was more than 90 percent elderly. More than 80 percent of the residents were private pay.
When apartments that function as board and care homes are excluded, the remaining unlicensed home population is smaller, with an average size of 19 beds. Among these unlicensed homes, 65 percent are small (2-10 beds), 25 percent are medium-sized (11-50 beds), and only 10 percent are large (51+ beds).
7.3 Conclusion
In conclusion, there are significant differences among States in the supply of licensed and unlicensed homes. Extensive regulation is associated with a higher supply of licensed homes per 1,000 elderly and a higher ratio of board and care beds to nursing home beds. This fact, combined with the fact that residents in States with extensive regulatory systems tend to be more impaired, suggests that those States may be pursuing a deliberate strategy of substituting care in board and care homes for care in nursing homes. States with more limited regulatory systems rely almost completely on nursing homes for the provision of residentially based long-term care. Further, they rely more on unlicensed facilities to provide a significant proportion of board and care housing.
SECTION 8: CONCLUSIONS
This section summarizes the major findings of the study of the effect of regulation on board and care home quality and discusses their implications.
8.1 Study Findings
8.1.1 Key Descriptive Findings
Several descriptive findings emphasize how board and care homes have changed over the last decade. These findings also provide a context for the policy implications discussed in Section 8.2.
- The average resident is significantly older and more disabled than was true a decade ago.
- While the perception is that board and care consists of small, private family homes, most residents live in fairly large facilities; the majority live in places with more than 50 beds.
- In the 10 study States, an estimated 12 percent of the homes and 27 percent of the beds are in unlicensed board and care homes.
- During the last decade, a new type of unlicensed home has emerged: retirement apartments and places called assisted living facilities that provide the same services as licensed homes (meals, protective oversight, and personal care) but are not licensed. They tend to be large, house mainly elderly residents, and house only a few residents who are poor or near poor.
8.1.2 Positive Effects of Regulation on Quality
Regulation was associated with better quality in a number of areas. Four findings are particularly relevant.
-
Licensure alone was effective in ensuring that homes provided care above a threshold of minimum performance.
Many observers believe that this prevention of performance below some minimally acceptable level of quality is the main role of regulation. The minimum requirements of licensure, whether in States with extensive or limited regulatory systems, prevented homes from having the worst performance along key quality dimensions, including
-
Low prevalence of safety features, social aids, supportive devices, and physical amenities.
-
-
Extensive regulatory systems reduced the prevalence of unlicensed homes.
By having a broad definition of places that required an operating license and by enforcing licensure, States with extensive regulatory systems reduced the prevalence of unlicensed homes.
-
Extensive regulatory systems and licensure were effective in promoting better safety, quality of life, and quality of care.
For some aspects of quality, the basic elements of licensure requirements alone, whether in States with extensive or limited regulatory systems, were sufficient to promote higher quality. For other aspects of quality, the additional components of extensive regulatory systems were needed to achieve better quality.
- Licensure, regardless of the type of regulatory system, was associated with:
- A higher percentage of safety features in homes
- Greater availability of an array of supportive long-term care services, such as personal care, special diets, transportation to medical and dental appointments, and, when needed, nursing care.
- Extensive regulatory systems were associated with important aspects of better quality, including:
- Lower use of psychotropic drugs
- Lower use of medications that are contraindicated for use with the elderly
- Greater availability of social and recreational aids.
- Licensure and extensive regulation combined were associated with:
- Increased staff knowledge of, and willingness to refer problems to, the ombudsman program
- Greater likelihood that operators are trained in the care of the elderly and disabled
- Greater availability of supportive services.
- Licensure, regardless of the type of regulatory system, was associated with:
-
Regulation achieved positive effects on quality without producing an excessively institutional model of care.
Despite fears that regulation would lead to an institutional model of care, licensed homes and homes in States with extensive regulatory systems were not more likely to be "institutional." Instead, they tended to be smaller, to have greater environmental diversity, and to make more social and recreational aids available to residents.
8.1.3 No Effect of Regulation on Some Aspects of Quality
Regulation did not produce positive effects on all the aspects of quality studied. Instead, such factors as home size and whether it was an "apartment-type" board and care home were associated with differences in quality. Measures on which regulation had no effect include:
- Operator requirements on preservice and in-service training for staff
- Staff knowledge of basic care procedures and appropriate monitoring of health conditions, characteristics of normal aging, and medication administration
- Availability of licensed nurses on staff
- Cleanliness and attractiveness of the home
- Availability of physical amenities.
8.2 Implications of Study Findings
8.2.1 General Implications
The study findings have several important implications for key participants in the board and care sector. Study findings point to a board and care population that is considerably older and more frail and disabled than it was a decade ago. Also, the mix of physically frail elderly, cognitively impaired elderly, and residents with mental illness and developmental disabilities, some of whom are nonelderly, presents a complex caregiving challenge. These factors should prompt a reexamination of the health and safety issues that confront the board and care home providers and the States' systems for regulating the industry. Of primary importance are the range of services, staffing patterns, and staff training and knowledge needed to meet the needs of today's residents.
8.2.2 Specific Implications
There are four specific implications from the study.
-
States can improve the quality of care in board and care homes through appropriate regulation.
The findings show that extensive regulation produced changes in several key areas. First, extensive regulatory systems were associated with lower use of psychotropic medications and lower use of medications contraindicated for the elderly. Given the high rates of psychotropic drug use among residents and the potential for adverse effects on their physical and cognitive functioning and risk for falls, this is particularly significant. In addition, given the limited availability of staff who are adequately trained in monitoring residents for adverse effects of medications, regulatory policies that are associated with lower use of potentially harmful or contraindicated medications are especially important.
Second, in licensed homes, extensive regulation was associated with other positive effects on quality of care in terms of operator training, greater availability of supportive devices and social aids, and increased staff knowledge of the ombudsman program. The greater availability of such devices supports the safe daily function of residents with physical disabilities, while social aids offer residents opportunities for more social interaction, activities, and enhanced quality of life. Links to the ombudsman program are also important because the role of ombudsmen in long-term care is to support both providers and residents in improving quality and to complement the activities of the regulatory system.
Third, extensive regulation was associated with lower prevalence of unlicensed homes. Thus, the positive effects of licensure are extended to a greater proportion of places providing board and care services to persons with disabilities.
These positive effects are especially compelling because the differences between States with extensive regulatory systems and those with limited systems are not huge. One key difference is that States with extensive regulatory systems extend licensure requirements to both small homes and facilities that house residents in apartments if they provide protective oversight and supportive services or house residents needing such care. A second key difference is that States with extensive regulatory systems have and use a wider array of enforcement remedies or sanctions compared to States with more limited systems.
-
States can improve other aspects of quality by requiring licensure of board and care homes.
The requirements in licensure laws alone serve to prevent the worst performance among homes along a number of important dimensions of quality. They also appear to encourage greater safety in homes, greater availability of a range of supportive long-term care services, and better performance in other areas. Thus, one clear implication is that States may be well served by the simple extension of licensure requirements to all places providing "board and care."
-
The Federal government can support the efforts of States and providers to improve quality of care by developing and disseminating information.
Although States have traditionally assumed the primary responsibility for the provision of board and care services and for regulating homes, the Federal role remains important. The Federal government can continue to develop and disseminate information about changes in the board and care sector. Information can include the changing role of board and care relative to the rest of the long-term care sector, the characteristics and care needs of residents, and the structure of the industry and its capacity to provide appropriate care. Also, it can provide information about the emergence of new modalities of care, such as assisted living, and the implications for the supply, affordability, and quality of long-term care options. In addition, the Federal government can develop and disseminate information about the States' regulatory and payment policies. Finally, the Federal government can develop and disseminate information about innovative models, such as ombudsman training programs for staff and operators, formal contracts between board and care homes and home health providers for the provision of services to residents, the development and functioning of "teaching" board and care homes that serve as resources to other facilities, and other new and promising arrangements for providing long-term care services in residential settings.
-
The board and care home industry should work closely with State governments to improve quality of care.
This study confirms that there is a well-defined niche or role for board and care homes in the provision of long-term care. Board and care homes fill the niche between residential settings such as congregate apartments and nursing homes. However, the increasing age and disability level among board and care residents raise health and safety concerns that could best be addressed through collaborative efforts between States and the industry. Historically, regulatory reform in long-term care has been opposed by an industry fearful of over-regulation and has come about primarily on the heels of scandals about spectacularly bad care. Such an environment seldom fosters careful consideration of the range of regulatory options available and how policies can be structured to support the efforts of good providers while minimizing the prevalence of bad ones. Those members of the board and care industry who consistently provide good care have much to teach policy-makers about the elements of their structure and care process that contribute to appropriate quality of care and life for residents. By taking a proactive role in helping define standards and regulatory approaches that promote better quality and minimize the prevalence of bad operators, the industry can help improve regulation without creating an unresponsive and overly burdensome process.
SECTION 9: REFERENCES
ABA (American Bar Association). 1983. Board and Care Report: An Analysis of State Laws and Programs Serving Elderly Persons and Disabled Adults. Report to the Department of Health and Human Services. Washington, DC.
Avorn, J., P. Dreyer, K. Connely, and S.B. Soumerai. 1989. Use of psychoactive medication and the quality of care in rest homes. New England Journal of Medicine 320(4):227-232.
Beers, M.H., J.G. Ouslander, I. Rollingher, D.B. Rueben, J. Brooks, and J.C. Beck. 1991. Explicit criteria for determining inappropriate medication use in nursing home residents. Archives of Internal Medicine 151:1825-1832.
Budden, F. 1985. Adverse drug reactions in long-term care facility residents. Journal of the American Geriatrics Society 33:449-450.
Clark, R., J. Turek-Brezina, C. Hawes, and C. Chu. 1994. The supply of board and care homes: Results from the 1990 National Health Provider Inventory. Presentation at the Gerontological Society of America, Atlanta, Georgia. November.
Dittmar, N.D., and G. Smith. 1983. Evaluation of the Board and Care Homes: Summary of Survey Procedures and Findings. Report to the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, Denver Research Institute. University of Denver, Denver, Colorado.
Dobkin, L. 1989. The Board and Care System: A Regulatory Jungle. The American Association of Retired Persons, Washington, DC.
DuNah, R., C. Harrington, and B. Bednew. 1993. Variations and Trends in Licensed Nursing Home Capacity in the States, 1978-1992. Institute on Health and Aging, University of California, San Francisco, CA.
Eckert, J.K., K.H. Namazi, and E. Kahana. 1987. Unlicensed board and care homes: An extra-familial living arrangement for the elderly. Journal of Cross-Cultural Gerontology 2:377-393.
GAO (General Accounting Office, United States Congress). 1989. Insufficient Assurances That Residents' Needs Are Identified and Met. Report to Congressional Requesters.
GAO (General Accounting Office, United States Congress). 1992a. Board and Care Homes: Elderly at Risk from Mishandled Medications. Report to House Subcommittee on Health and Long-Term Care. U.S. Government Printing Office, Washington, DC.
GAO (General Accounting Office, United States Congress). 1992b. Drug Use and Misuse in America's Board and Care Homes: Failure in Public Policy. Report to House Select Committee on Aging. U.S. Government Printing Office, Washington, DC.
Griffith, J. 1995. Personal Communication on the HUD-sponsored evaluation of the Congregate Housing With Services Program evaluation, Research Triangle Institute, Research Triangle Park, NC.
Harrington, C., R. DuNah, B. Bedney, and H. Carillo. 1994. Variations and Trends in Licensed Nursing Home Capacity in the States, 1978-1993. Policy Paper. Institute for Health and Aging, University of California at San Francisco, San Francisco, CA.
Hartzema, A.G., N.P. Godbout, S.D. Lee, T.R. Konrad, and F.M. Eckel. 1986. Evaluation of an Educational Intervention to Reduce Medication Administration Errors in Domiciliary Care Facilities. Unpublished manuscript. School of Pharmacy, University of North Carolina, Chapel Hill, NC.
Hawes, C., J. Wildfire, and L. Lux. 1993. The Regulation of Board and Care Homes: Results of a Survey in the 50 States and District of Columbia--National Summary. American Association of Retired Persons, Washington, DC.
Hawes, C., C.D. Phillips, J.N. Morris, V. Mor, and B.F. Fries. 1994. Design of the Evaluation of the National Nursing Home Resident Assessment Instrument (RAI) and Effects on Process Quality. Presentation at the annual meeting of the Gerontological Society of America, Atlanta, GA. November.
Manard, B. et al. 1990. Methodology for Developing a Comprehensive List of Licensed Board and Care Homes. Unpublished report from Lewin/ICF, Inc., and James Bell Associates to the Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, Fairfax. VA.
Moon, M., G. Gaberlavage, and S.J. Newman. Preserving Independence, Supporting Needs: The Role of Board and Care Homes. American Association of Retired Persons, Washington, DC.
Moos, R.H., and S. Lemke. 1978. Assessing the physical and architectural features of sheltered care setting. Journal of Gerontology 35(4):471-583.
Mor, V., S. Sherwood, and C. Gutkin. 1986. A national study of residential care for the aged. The Gerontologist 26(4):405-417.
Newcomer, R.J., and L.A. Grant. 1988. Residential Care Facilities. Understanding Their Role and Improving Their Effectiveness. Policy Paper No. 21. Institute for Health and Aging, University of California at San Francisco.
Phillips, C.D., J.N. Morris, C. Hawes, V. Mor, and B.F. Fries. 1994. The effects of the national nursing home Resident Assessment Instrument (RAI) on resident outcomes. Presentation at the annual meeting of the Gerontological Society of America, Atlanta, GA, November.
Reichstein, K.J., and L. Bergofsky. 1980. Report on the National Survey of State Administered Domiciliary Care Programs in 50 States and the District of Columbia. Horizon House Institute, New York, NY.
Reichstein, K.J., and L. Bergofsky. 1983. Domiciliary care facilities for adults: An analysis of state regulations. Research on Aging 5(1):25-43.
Reisacher, S. 1985. A Study of Unlicensed Board and Care Homes in Cuyahoga County. Boarding Home Advocacy Program, an affiliate of the Nursing Home Ombudsman Program, Cleveland, Ohio.
Reschovsky, J., and H. Ruchlin. 1993. Quality of board and care homes serving low income elderly: Structural and public policy correlates. The Journal of Applied Gerontology 12(2):225-245.
Sherwood, S., V. Mor, and C. Gutkin. 1981. Volumes 1-3: Domiciliary Care Clients and the Facilities in Which They Reside. Hebrew Rehabilitation Center for Aged, Boston, MA.
Sherwood, S., and M.M. Seltzer. 1981. Task III Report: Board and Care Literature Review. Evaluation of Board and Care Homes. Boston University School of Social Work, Boston, MA.
Spore, D., V. Mor, J. Hiris, E.P. Larrat, and C. Hawes. 1995 (forthcoming). Psychotropic use among elderly residents of board and care facilities. Journal of the American Geriatrics Society.
Stone, R., and R.J. Newcomer. 1985. The state role in board and care housing. In Long Term Care of the Elderly: Public Policy Issues. C. Harrington, R.J. Newcomer, C.L. Estes (eds.). Sage Publications, Beverly Hills, CA.
Stuck, A.E., M.H. Beers, A. Steiner, H.U. Aronow, L.Z. Rubenstein, and J. Beck. 1994. Inappropriate medication use in community-residing older persons. Archives of Internal Medicine 154:2195-2200.
U.S. DHHS Inspector General (U.S. Department of Health and Human Services, Office of theInspector General). 1990. Board and Care. U.S. Department of Health and Human Services, Regional Inspector General for Region II, Office of Evaluation and Inspection, New York, NY.
U.S. House of Representatives, Select Committee on Aging. 1989. Board and Care Homes in America: A National Tragedy. A report by the Chairman of the Subcommittee on Health and Long-Term Care, House of Representatives, Comm. Pub. No. 101-711.
NOTES
-
The Keys Amendments to the Social Security Act (Section 1616[e]) were enacted in 1976 with the goal of preventing Supplemental Security Income (SSI) recipients from being in substandard board and care homes. Under Keys, the States are required to certify to DHHS that all facilities in which significant numbers of SSI recipients reside meet appropriate standards. GAO (1989) found that the oversight exercised by DHHS is limited, and the sanction for substandard care is rarely used.
-
SSI is a Federal income support program for poor persons who are aged, blind, or disabled. SSI can be used to pay for board and care and, as of 1990/91, all but 10 States provided a supplemental payment (SSP) for SSI recipients residing in board and care homes.
-
Approximately one-third of the 3,000 places identified as possible unlicensed homes could not be screened by telephone because they had no telephone or no listed telephone number, did not answer the telephone on more than 10 attempts, or information was insufficient to generate an address or telephone number.
-
Other payers include Medicaid waiver programs and the Department of Veterans' Affairs, but they represent a relatively small proportion of the total.
-
The worst scores overall were on the items associated with normal aging. Most staff believed that memory problems and confusion were "normal" parts of aging, and many believed that sad mood and incontinence were normal.