
U.S. Department of Health and Human Services
Considering Children with Disabilities and the State Children's Health Insurance Program
Lynn Elinson, Westat, Inc.
Gavin Kennedy, Office of Disability, Aging and Long-Term Care Policy
Lois Verbrugge, Westat, Inc.
November 1998
PDF Version: http://aspe.hhs.gov/daltcp/reports/1998/kidbroc.pdf (10 PDF pages)
This brochure was prepared under contract #HHS-100-97-0009 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Westat. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The Project Officer was Gavin Kennedy.
This brochure was supported by the Office of Disability, Aging and Long-Term Care Policy (DALTCP) in the Office of the Assistant Secretary for Planning and Evaluation (ASPE) within the U.S. Department of Health and Human Services (DHHS). It was jointly developed by Westat and DALTCP. For inquiries about this brochure, please contact Gavin Kennedy, ASPE/DALTCP, (202) 690-6443. The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
CHIP planning and implementation staff and decisionmakers in States need information about children with disabilities so that their programs are accessible and meaningful for these children.
INTRODUCTION
-
More than 10 million children (14.3 percent) under age 18 in the United States have no form of health insurance.
-
Of those 10 million children, more than 7 million also live in low-income families.1 Some of these children may be eligible for the State Children's Health Insurance Program (CHIP), newly enacted under Title XXI of the Social Security Act.
-
Of the more than 7 million children who may be eligible for CHIP or Medicaid, 7 percent (about 530,000) have a disability.
-
CHIP planning and implementation staff and decisionmakers in States need information about children with disabilities so that their programs are accessible and meaningful for these children.
CHIP provides States the opportunity to expand health care coverage to low-income children. All low-income children, whether they are disabled or not, can benefit from improved access to health care associated with insurance coverage. The majority of children with disabilities have the same health care needs as children without disabilities. However, some children with disabilities require special health care services as well as more of the usual health care services. In addition, the special needs of some children with disabilities have implications for methods of health care delivery and financing that States develop through CHIP insurance expansions.
The purpose of this brochure is to familiarize State decisionmakers with low-income uninsured children with disabilities so that they have essential information about these children as they develop and implement CHIP plans. We describe uninsured children with disabilities, their numbers, their needs, and how opportunities presented by CHIP can help.
WHO ARE UNINSURED CHILDREN WITH DISABILITIES?
Children with disabilities can be defined as those who have persistent difficulty doing ordinary childhood activities.2 These children have physical, behavioral, and emotional problems that can make it difficult for them to participate in strenuous activities, get along with others, communicate and learn, or participate in neighborhood or school activities with their peers.
According to data from the 1994 National Health Interview Survey--Disability Supplement (NHIS-D):
-
More than 5.5 million children (8 percent) in the United States have disabilities.
-
About 700,000 children with disabilities (12 percent) lack health insurance coverage, and most of these children (77 percent or 530,000) live in low-income families.
-
Seventy percent of these low-income families without health insurance report that insurance coverage is too expensive. To a lesser extent these families cite unemployment (2.9 percent) and lack of dependent coverage by employer plans (4.6 percent) as reasons their disabled children do not have insurance.
What are the characteristics of low-income uninsured children with disabilities? We found that (Figure 1):
- 46.5 percent are between the ages of 11 and 17
- 53.2 percent are White/Non-Hispanic
- 40.3 percent are from the South
Among low-income children, there are differences in the percentage of children who are insured. These differences sort out by age, region of the country, and race, both for children with and without disabilities (Figure 2). For example:
-
Among low-income children with and without disabilities, the percentage who are uninsured increases as age increases.
-
Among low-income children with and without disabilities, the South and West had the highest percentage of uninsured children compared to the Northeast and Midwest.
When we looked at the percentage of low-income children who are uninsured by race, we saw few differences among low-income disabled children (Figure 2).
WHAT DO CHILDREN WITH DISABILITIES NEED?
Data from the NHIS Disability Supplement (NHIS-D) help to characterize the health care needs of children with disabilities. When parents with children without disabilities are compared to those of children with disabilities, the latter are more likely to report that their children have fair or poor health, that their children use more health services, and that their children use specialty services.
Children with Long-Term Care Needs. Approximately 387,000 children in the United States have long-term care needs. More than one quarter (27 percent) of parents of these children report their children are in fair or poor health, while 12.7 percent of parents of other children with disabilities report fair or poor health.3 By comparison, only 2 percent of parents of children without disabilities report fair to poor health.
Children with long-term care needs tend to use more health services than other children with disabilities or their non-disabled peers (Figure 3). Nearly one-half (49 percent) of children with LTC needs had six or more visits to a physician within the 12 months prior to the survey, whereas nearly one-third (31.5 percent) of other children with disabilities had six or more visits in the previous year, and only 12.4 percent of children without disabilities had six or more physician visits. Similarly, 16.6 percent of children with LTC needs, stayed in a hospital overnight in the previous year, compared to 8.8 percent of children with disabilities but no LTC needs. The lowest percentage who have hospital stays in the previous year was among children with no disabilities (2.4 percent).
All Children with Disabilities. Whereas less than one-tenth of a percent of children without disabilities received occupational or physical therapy services in the 12 months prior to the survey, more than one-third of children with long-term care needs required therapy services. Fewer than 10 percent of other children with disabilities required such services.
Children with disabilities also have special needs that policymakers should consider in the design of CHIP programs. A few potential considerations include:
- Appropriate and comprehensive coverage
- Appropriate utilization controls with gatekeepers familiar with the needs of children with disabilities
- Access to quality specialty care
- Cost sharing that is sensitive to the frequency of services that some children with disabilities may need
- Program and access standards that comply with the Americans with Disabilities Act (ADA) and Section 504 of the Rehabilitation Act.
What do the recent changes in the SSI definition of disability mean for CHIP?
The Personal Responsibility and Work Opportunity Reconciliation Act of 1996 (PRWORA or "welfare reform") established a more restrictive definition of childhood disability. The new law will redetermine the eligibility of close to 263,000 children for Supplemental Security Income (SSI). The receipt of SSI benefits automatically provides categorical eligibility for Medicaid. Although the Balanced Budget Act of 1997 (BBA) provided that children who were to lose SSI because of the new definition should continue categorical eligibility for Medicaid, this provision does not affect future applicants who are denied SSI for failing to meet the stricter disability thresholds. If denied SSI in the future, they would also be denied categorical eligibility for Medicaid.
It is anticipated that the more restrictive definition of disability will lead to an increase in SSI denials. Nevertheless, medical assistance continues to be critical for many children who may a range of disabilities but are no longer eligible because of the change in definition of childhood disability. Outreach efforts should focus on communication with the families of these children to inform them about their health care options (Medicaid and CHIP).
Since large numbers of children applying for SSI are denied benefits, States will want to ensure that CHIP information is available in SSA field offices and that disability determination workers are aware of the insurance coverage options for low-income children.
WHAT DIFFERENCE DOES INSURANCE MAKE?
Health insurance is an important key to better health. It provides most people with access to many of the health care services they need. And so it is with children with disabilities.
Although sample sizes were small, the data suggest that children with disabilities who are insured and those who are uninsured use health services differently (Table 1). In 1994, for example, 91.7 percent of insured children with disabilities visited a physician at least once in the previous year, compared with 80 percent of uninsured children with disabilities (Table 1). Two percent of uninsured children with disabilities used occupational therapy services, compared to 6.9 percent of their insured peers. Further, uninsured children were less likely to have physical therapy and visited a physician less often. The two groups differ only slightly in the use of hospital services, but those differences go in the same direction of less care for the uninsured.
HOW CAN CHIP WORK FOR CHILDREN WITH DISABILITIES?
The Importance of Flexibility
Not surprisingly, children are able to get the care they need more easily when they are insured. Many uninsured children may be eligible for Medicaid; others can benefit from insurance expansions afforded by CHIP. CHIP provides a variety of opportunities to close the insurance gap for all children, including those with disabilities.
Title XXI gives States remarkable flexibility to expand health insurance coverage for low-income children. States now have the authority to design and implement unique approaches to insuring low-income children through a separate health insurance program (subject to certain coverage and eligibility requirements), through Medicaid, or through a combination of both.
Title XXI also allows the use of up to 10 percent of total expenditures on administration, outreach, and the direct purchase of health services. This means that the implementation of CHIP allows, in part, for the design of cost effective programs that include traditional community-based delivery systems or programs that provide direct or enabling services to children with (or without) disabilities. These services are generally delivered one-on-one between a health professional and a child in an office, clinic, school-based facility, or hospital. Examples may range from basic primary care to specialty and sub-specialty care for children with disabilities and/or special health care needs. In short, 10 percent funds can be used to "beef up" services for children with disabilities and special health care needs by providing services in addition to the basic benefit package offered through CHIP.
Also, in non-Medicaid CHIP programs, a State can offer a separate benefit package (or a supplemental package as part of the basic benefit package offered to all CHIP beneficiaries) tailored for these children so long as the entire package meets all the eligibility and coverage requirements under Title XXI.
Already, States have used the flexibility under Title XXI to address children with disabilities and special health care needs in unique ways:
Connecticut offers a combination plan called "HUSKY Care". HUSKY Care covers children whose family income is less than 185 percent of the Federal poverty level through Medicaid. Children who live in families with incomes that fall between 185 percent and 300 percent of the Federal poverty level are covered under a separate insurance program, contracted with managed care plans. Children in the separate program who are identified as having special health care needs are eligible for an enhanced benefit package (called "HUSKY Plus"). HUSKY Plus provides two supplemental benefit packages -- one for severe physical disabilities -- and another for severe behavioral health needs.
North Carolina offers a separate insurance program to all Title XXI expansion beneficiaries. Children with special health care needs will receive a benefit package equal to the one offered under the State's existing Medicaid program.
Many other States are opting to expand Medicaid. By law, Medicaid provides a rich benefit package through Early, Periodic, Screening, Diagnosis and Treatment (EPSDT). EPSDT requires comprehensive and preventive health screening for all children enrolled in Medicaid in order to identify and treat health problems before they become more complex, more disabling, and more costly.
What about Coordination?
Some children with disabilities have complex needs that require health and support services from a variety of programs (e.g., State Title V programs for children with special health care needs, Special Education, Medicaid, Medicaid that includes school-based services, and State and locally supported service systems). Coordination begins with outreach and extends to service delivery. In order to maximize existing resources and assure continuity of service delivery, it is critical for CHIP programs to ensure that linkages among existing service systems are considered in any comprehensive planning approach.
For example, States can establish managed care contract specifications that accommodate the needs of children with disabilities or those with special health care needs, including coordination of treatment plans among various programs serving these children.4 Also, Medicaid or CHIP managed care plans can contract with other agencies serving children with disabilities to case manage, coordinate, or provide other types of services. State Maternal and Child Health (MCH) programs often interact with families and managed care programs to ensure access to comprehensive care for children with special needs. This may be done through "wrap around" services, such as transportation, case management, coordination, and direct services for children with disabilities and special health care needs.
What about Outreach?
By law, children who are eligible for Medicaid cannot be covered under CHIP, but a significant number of uninsured disabled children may currently be eligible for Medicaid but do not participate. For this reason, Title XXI requires that States identify and enroll children who are eligible, both for Medicaid and CHIP. Effective outreach and enrollment can play a major role in influencing participation in both programs.
While children with disabilities will often be reached by efforts that target other low-income children, outreach efforts can specifically target children with disabilities and special health care needs in a variety of ways. For example, knowledgeable outreach workers can be located in places where disabled and/or low-income children often receive services (e.g., Social Security offices, schools, and Title V program offices). In addition, easy-to-understand information can be made available. Development of outreach strategies might include traditional community-based providers who are often trusted by low-income families with disabilities and special health care needs because they are familiar with their particular needs. Families of children with disabilities have wide community support networks, providing an excellent opportunity to do outreach with those families lacking health insurance who might benefit from CHIP and Medicaid.
WHERE TO GET MORE INFORMATION
The following agencies and organizations have an interest in disability, children, and/or access to health care, and may be able to answer some of your questions about CHIP.
The Office of Assistant Secretary for Planning and Evaluation (OASPE), Office of Disability, Aging, and Long-Term Care Policy (DALTCP)
The Office of Disability, Aging, and Long-Term Care Policy (DALTCP), under the Office of Assistant Secretary for Planning and Evaluation (OASPE) in the Department of Health and Human Services (HHS) is charged with responsibilities for developing, analyzing, evaluating and coordinating policies and programs which support the independence, productivity, health and long-term care needs for persons of all ages with disabilities. This office can be contacted at:
Contact: Gavin Kennedy, DALTCP/ASPE/HHS, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201; (202) 690-6443 Email: DALTCP2@oaspse.dhs.gov Internet: http://aspe.hhs.gov/daltcp/home.htm
Health Care Financing Administration (HCFA)
The Health Care Financing Administration (HCFA) is the Federal agency within the U.S. Department of Health and Human Services that administers Medicare, Medicaid, and the Children's Health Insurance Program.
HCFA, 7500 Security Boulevard, Baltimore, MD 21244; (410) 786-3000 Internet: http://www.hcfa.gov/init/children.htm
Health Resources and Services Administration (HRSA)
The Health Resources and Services Administration (HRSA) directs national health programs which improve the health of the Nation by assuring quality health care to underserved, vulnerable and special-need populations and by promoting appropriate health professions workforce capacity and practice, particularly in primary care and public health.
HRSA/MCHB/Division for Children with Special Health Care Needs, Room 18A27, 5600 Fischers Lane, Rockville, MD 20857; (301) 443-2350 Internet: http://www.hrsa.dhhs.gov/childhealth.html
FOOTNOTES
-
Defined as below 200 percent of the federal poverty level (FPL) -- $32,900 for a family of four in 1998.
-
The information presented here describes children who have specific functional problems as described by the 1994 National Health Interview Survey--Disability Supplement (NHIS-D). Functional disabilities were defined as (1) limitations in or ability to perform a variety of physical activities (e.g., walking, lifting, reaching); (2) serious sensory impairments (e.g., inability to read newsprint even with glasses or contact lenses); (3) use of selected assistive devices (e.g., brace, artificial limb); (4) developmental delays (e.g., physical, learning) identified by a physician; (5) for children under age 5, inability to perform age appropriate functions (e.g., sitting up, walking); and/or (6) long-term care needs. In this analysis, functional disability includes only those conditions that have lasted or are expected to last 12 months or more. This definition was developed by the Office of the Assistant Secretary for Planning and Evaluation (ASPE), HHS. Others using the NHIS-D to analyze childhood disability may define childhood disability differently and arrive at different estimates.
-
Long-term care needs represent the most severe dysfunctions. For children under age 5, LTC was defined as having one or more of the following: (1) needing special equipment to breathe; (2) difficulty with chewing, swallowing, or digesting; (3) needing special medical equipment for eating or toileting; (4) inability to sit up by age 2; and/or (5) walking by age 3 or older. For children ages 5 and older, LTC was defined as needing the help of another person or special equipment in order to perform at least one of the activities of daily living (ADLs). The ADLs including bathing, dressing, eating, getting in and out of bed or chairs, using the toilet (including getting to the toilet) and getting around inside the home.
-
Children with special health care needs (CSHCN) are defined by the Health Resources and Services Administration as "those who have or are at increased risk for chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally." Our analysis focused on children with disabilities, which comprise a subset of CSHCN. Similar analyses examining CSHCN will yield higher estimates.
| FIGURE 1: Demographic Characteristics of Uninsured Children with Low Family Income and Disabilities*, ** | ||
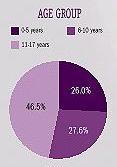 | 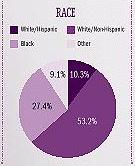 | 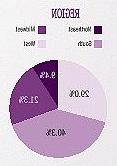 |
| * About 530,000 children are uninsured, have low family income, and have disabilities.** SOURCE: 1994 National Health Interview Survey - Disability and Family Resources Supplements. | ||
| FIGURE 2: Percent Uninsured Among Low-income Children With and Without Disabilities* | ||
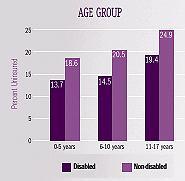 | 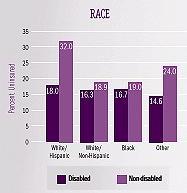 | 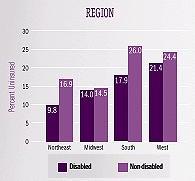 |
| * SOURCE: 1994 National Health Interview Survey - Disability and Family Resources Supplements. | ||
| FIGURE 3: Health Care Utilization of Children with Long Term Care Needs, Other Children with Disabilities, and Children with No Disabilities* | |
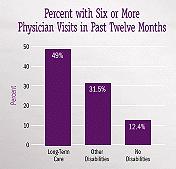 | 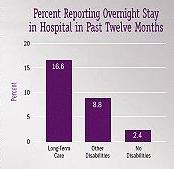 |
| * SOURCE: 1994 National Health Interview Survey - Disability Supplement. | |
| TABLE 1. Health Status and Health Services Use of Children with Disabilities, by Insurance Status, 1994* | ||
| Health Status and Health Services Use | Insured | Uninsured |
| Fair/Poor self-rated health | 13.6%a | 14.4% |
| At least one physician visit in past year | 91.7%b | 80.0% |
| Hospital stays in past year | 9.5%a | 8.4% |
| Occupational therapy in past year | 6.9%c | 2.0% |
| Physical therapy in past year | 8.5%a | 5.2% |
* SOURCE: 1994 National Health Interview Survey--Disability, Family Resource, and Health Insurance Supplements
| ||
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]