
Monday, August 1, 2016
Indiana University Dissemination of the Aging Brain Care Program
Malaz Boustani, MD, MPH
Founding Director, Chief Innovation & Implementation Officer,
Sandra Eskenazi Center For Brain Care Innovation
Indiana University Center for Health Innovation and Implementation Science
IU Team
- Mentors & peers
- Chris Callahan
- Greg Sachs
- Mary Austrom
- Siu Hui
- Daniel Clark
- Su Gao
- Lisa Harris
- Patrick Monahan
- Wanzhu Tu
- Anthony Perkins
- Mentees:
- Noll Campbell
- Babar Khan
- Nicole Fowler
- Michael LaMantia
- Richard Holden
- Daniel Bateman
- Sophia Wong
- Ashley Overlay
- Nadia Adams
- Cathy Alder
- Ben Zarzour
- Potential Conflict of Interest in the past 12 months
- Hold equity in a preferred population health management (PPHM), LLC. PPHM is the distributing network for the IU ABC program.
- Member of the Beacon Advisory Board for Astra-Zneca.
- Source of Funding:
- For Brain Care Discovery:
- K23AG026770; R01AG029884; R01AG040220; R01AG034205; P30AG024967; R01HS019818; and R01HS10884.
- For Brain Care Delivery:
- R24MH080827; 1C1CMS331000-01-00; 1L1CMS331444-01-00; and Eskenazi Health Foundation.
- For Brain Care Discovery:
Objectives
- Describe the structure, the tools, the staffing models, and effectiveness of the IU Aging Brain Care model.
Indiana University Reaction
- Developed the Aging Brain Care Model (ABC beta ) (2000-2001).
- Evaluated the model in RCT* (2001-2006).
- Translated the model into a local clinical program (ABC 1.0) (2007).
- Served 1,000 patients in Indianapolis (2012).
- Developed a scalable version (ABC 2.0) (2012).
- Served 5,000 patients in Indiana (2015).
- Active distribution of the ABC 2.0 (2015)
- Developing an advanced scalable version (ABC 3.0) (2016)
*RCT: Randomized Controlled Trial
The Aging Brain Care Model (ABC beta)
- Primary Care Clinician (Hospitalists):
- detect and treat delirium
- detect and treat BPSD
- Enhance cholinergic system by
- Prescribe ChEIs
- Discontinue Anticholinergic
- Caregiver Focus:
- Problem solving skills
- Counseling
- Respite care
- Support group
- Expert Team:
- Geriatrician
- Social Psychologist
- GeroPsychiatrist
- General Environmental Modification:
- Medication adherence support
- Home safety assessment
BPSD: Behavioral and psychological symptoms
ChEIs: Cholinesterase inhibitors
Callahan et al, JAMA 2006; Austrom et al, Gerontologist 2004; Boustani et al, JCIA 2006
Work Force for ABC Model from 1.0 to 3.0
Today ABC 2.0: : M-F 8-5 p.m. about $ 100 p.m.p.m., focusing on dementia / depression
Future ABC 3.0: 24/7 about $ 50 p.m.p.m., almost all brain conditions
- ABC 1.0 -- MD; RN & SW
- ABC 2.0 -- MD; RN & SW; CCA
- ABC 3.0 -- MD; RN & SW; CCA; Patients and informal caregivers
p.m.p.m.=per member per month; MD=medical doctor; RN=registered nurse; SW=social worker; CCA=care coordinator assistant; eMR ABC=electronic medical record ageing brain care (a specialized software application for the model)
IT Support of ABC Model from 1.0 to 3.0
- ABC 1.0 -- MD, eMR-ABC; RN / SW + eMR-ABC
- ABC 2.0 -- MD, eMR-ABC; RN / SW + eMR-ABC; Care Coordinator Assistants + eMR-ABC
- ABC 3.0 -- MD, eMR-ABC; RN / SW + eMR-ABC; Care Coordinator Assistants + eMR-ABC; Informal Caregiver + AVATAR
Standardized Minimum ABC 2.0 Care
- Check Hospital & ER Alerts every day
- Coordinate with Inpatient services
- Alert hospital team of presence of cognitive or mood problems
- Medications conciliation
- Connect with family caregiver
- Request Geriatric consult (If available)
- Coordinate post discharge transition
- Post discharge care
- Home visit within 72 hours of discharge
- Medication reconciliation
- Coordinate Home Care visit
- Coordinate post hospital orders
- Deliver Delirium protocol and handout
- Ongoing Aging Brain Care
- Manage Depression
- Problem Solving Therapy
- Pharmacotherapy
- Cognitive behavioral Therapy
- Manage Cognitive Impairment
- Cholinesterase inhibitors (if needed)
- D/C medications with adverse cognitive effects (Anticholinergics, Histamine 2 antagonists, Benzodiazepines)
- Caregiver problem solving coaching
- Medication adherence support
- Manage Depression
Callahan et al, Aging & Mental Health 2011; Boustani et al, Aging & Mental Health 2011; LaMantia et al, JAGS 2015
The Current Tools of ABC 2.0
- Mobile office
- HABC Monitor for both self and Caregiver report
- eMR-ABC population management software
- Mobile HABC App for Informal Caregiver
- ABC Replication Manual
- ABC Caregiver Booklet
- Anticholinergic Cognitive Burden Scale
LaMantia et al JAGS 2015; Frame et al eGEMS 2013; Monahan et al, JCIA 2010; Monahan et al JCIA 2012; Boustani et al, JCIA 2009
The ABC beta version Efficacy
- NNT = 3.7
- 7 NPI point improvement
- Each 1 point decline in NPI = $250-$400 in health care expenses
- Potential saving 1750-$2800 per patient
- Improvement in family stress
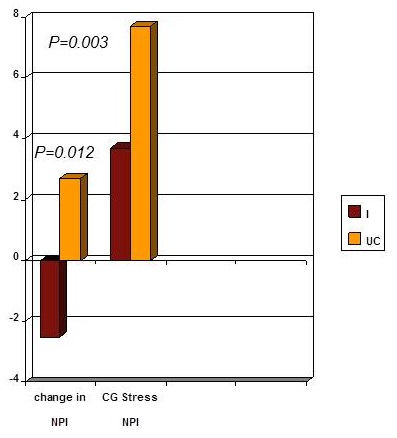 |
| Callahan, Boustani et al, JAMA 2006 |
NNT: Number Need to Treat; NPI: Neuropsychiatric Inventory; CG: Caregiver
ABC 1.0 Performance
| The Acute Care Service Utility Domain | ABC | PCC |
|---|---|---|
| % patients with at least one ER visit | 28% | 49% |
| Total number of ER visits | 124 | 1143 |
| % patients with at least one hospitalization | 13% | 26% |
| Total number of hospitalizations | 45 | 438 |
| Mean/Median length of hospital stay | 5 / 4 | 7 / 4 |
| ABC; Aging Brain Care patients; PCC: primary care center patients Boustani et al, Aging & Mental Health 2011 |
||
| The Quality of Care Indicator Domain | ABC | PCC |
|---|---|---|
| % seen at ER again within one week | 14% | 15% |
| % re-hospitalized within 30 days of discharge | 11% | 20% |
| % with at least one order of definite anticholinergics | 19% | 40% |
| % with at least one order of neuroleptics | 5% | 5% |
| % with at least one order of anti-dementia drugs | 55% | 13% |
| % with at least one order of antidepressant drugs | 68% | 48% |
| % with at least one order of definite anticholinergics and anti-dementia drugs | 16% | 32% |
| % with at least one LDL order | 82% | 72% |
| % of patients with LDL < 130 | 45% | 23% |
| % with at least one HbA1c order | 78% | 62% |
| % of patients with HbA1c < 8 | 78% | 51% |
| % with last systolic BP < 160 | 27% | 24% |
| ABC; Aging Brain Care patients; PCC: primary care center patients Boustani et al, Aging & Mental Health 2011 |
||
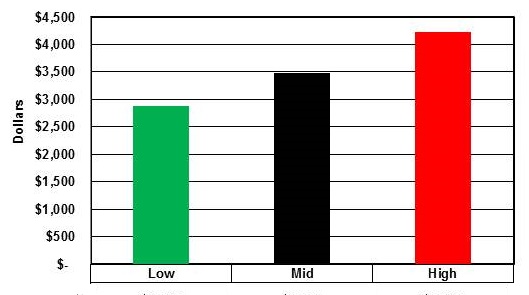
ABC 1.0 Annual Cost Savings Per Patient
 |
|||
| Total Cost Savings Per Patient | Low | Mid | High |
| $2,885 | $3,474 | $4,227 | |
ABC 2.0 Performance
| Health Outcomes | |
|---|---|
| Full Dementia Care Giver Responders at 12 months | 66% |
| Full Major Depression Patients Responders at 12 months | 51% |
| LaMantia et al, JAGS 2015 | |
ABC DistributionPreferred Population Health Management, LLC
- On-boarding of scalable and existing workforce within the AAAs. (multiple Mini Interview)
- Training and ongoing management and support of the scalable workforce (combined experiential adult learning based coaching)
- Ongoing Zoom-in & Zoom-out monitoring of the performance of the entire population to allow both complex case management and comprehensive resource allocation for the entire population at Risk (Population Health Logistic software)
- Evidence-based clinical pathway to mange the complex cognitive, functional, behavioral and psychological needs of both the client (member suffering from the disease) and their family caregiver.