
Friday, April 27, 2018
Printer Friendly Version in PDF Format (17 PDF pages)
DEFINING QUALITY DEMENTIA CARE
Alzheimer's Association
DefiningQuality Care: Dementia Care Practice Recommendations
Quality Care:History
- Guidelines for Dignity
- Key Elements of Dementia Care
- Dementia Care Practice Recommendations
DCPR Review and Development
- Reviewed feedback on DCPR format and structure
- Drafted model for revision
- Conducted focus group with care experts
- Conducted thematic analysis of existing dementia care guidelines
- Revised format/model and shared with care experts for review and feedback
- Worked with expert researchers/authors to develop topic area articles with recommendations
Researchers/Authors
- Person Centered Care Focus
- Fazio, Pace, Flinner & Kallmyer
- Detection and Diagnosis
- Maslow & Fortinsky
- Assessment and Care Planning
- Moloney, Kolanowski, Van Haitsma & Rooney
- Medical Management
- Austrom, Boustani & LaMantia
- Information, Education & Support
- Whitlach & Orsulic-Jeras
- Ongoing Care: ADLs
- Prizer & Zimmerman
- Ongoing Care: BPSD
- Scales, Zimmerman & Miller
- Staffing
- Gilster, Boltz & Dalessandro
- Therapeutic Environment and Safety
- Calkins
- Transitions/Coordination of Services
- Hirschman & Hodgson
Quality Care: Today
- Evidence-based practices
- 56 recommendations by 27 expert authors
- Applicable to various care settings and throughout the disease continuum
- Published as a supplement to Feb 2018 issue of The Gerontologist
- Foundation for quality person-centered care
Dementia Care Practice Recommendations
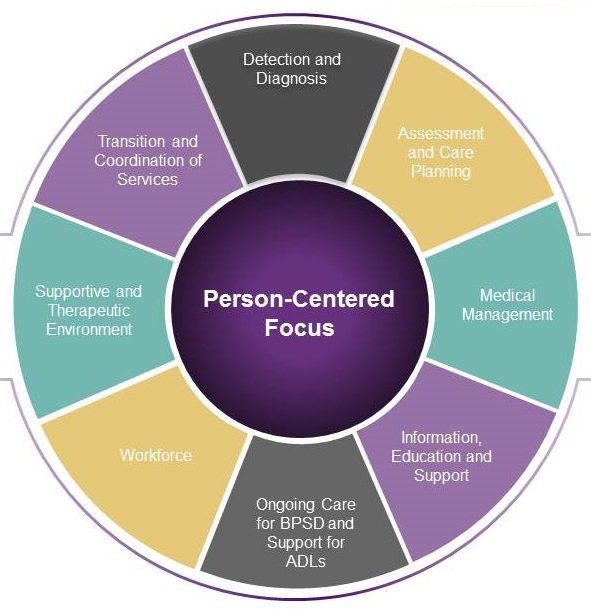 |
PERSON CENTERED FOCUS
- Recommendations:
- Know the person
- Person's reality
- Meaningful engagement
- Authentic, caring relationship
- Supportive community
- Evaluation of care practices
Effects of Person-Centered Care
| Individuals | Li and Porock (2014) | 24 studies--15 culture change and 9 person-lefted practices | Beneficial effects on psychological wellbeing. Significant effects on decreasing behavioral symptoms and psychotropic medication use |
|---|---|---|---|
| Staff | Barbosa, Sousa, Nolan, & Figueiredo (2015) | 7 studies--PCC approaches, including DCM; stimulation-oriented approaches, emotion-oriented approaches; and behavioral-oriented approaches. | Reduction in stress, burnout and job dissatisfaction |
| Individuals and staff | Brownie and Nancarrow (2013) | 9 articles--multi-component person-lefted interventions | Positive influences on staff satisfaction and capacity to provide care; lower rates of boredom and feelings of helplessness and reduced levels of agitation in residents |
DETECTION AND DIAGNOSIS
- Recommendations
- Information about brain health and cognitive aging
- Signs and symptoms of cognitive impairment
- Concerns, observation and changes
- Routine procedures for assessment and referral
- Brief mental status test when appropriate
- Diagnostic evaluation follow-through
- Better understanding of diagnosis
ASSESSMENT AND CARE PLANNING
- Recommendations
- Regular, comprehensive, person-centered assessments and timely interim assessments
- Information gathering, relationship building, education and support
- Collaborative, team approach
- Accessible documentation and communication systems
- Advance planning
Comprehensive PCC Assessment
- Experience of the person/care partner
- Function and Behavior
- Health Status and Risk Reduction
MEDICAL MANAGEMENT
- Recommendations
- Holistic, person-centered approach
- Role of medical providers
- Common comorbidities of aging
- Non-pharmacologic interventions
- Pharmacological interventions when necessary
- Person-centered plan for possible medical and social crises
- End-of-life care discussions
INFORMATION, EDUCATION AND SUPPORT
- Recommendations
- Preparation for the future
- Work together and plan together
- Culturally sensitive programs
- Education, information and support during transition
- Technology to reach more families
Early Stage: Becoming Familiar
- Education and Information
- Disease
- Symptoms
- Treatment
- Prognosis
- Support
- Support groups
- Technology-based
- Care planning for future
- Driving
Middle Stage: Increased Care and Support Needs
- Education and Information
- Family-centered
- Behaviors
- IADLs and PADLs
- Support
- Support groups
- Counseling
- Care coordination
- Technology-based
Late Stage: Relocation and End of Life Care
- Education and Information
- Care needs
- Continue in-home care or relocate to an alternate care setting
- Support
- Support groups or counseling
- End of life and hospice care
- Palliative care approach
ONGOING CARE: ADLs
- Recommendations
- Support for ADL function
- Person-centered care practices
- Dressing -- dignity, respect, choice; process; environment
- Toileting -- also health and biological considerations
- Eating -- also adaptations and functioning; food, beverage and appetite
Themes in Evidence to Provide Support for ADLs
| Dressing | Toileting | Eating and Nutrition |
|---|---|---|
| Dignity/respect/choice | Dignity/respect/choice | Dignity/respect/choice |
| Dressing process | Toileting process | Dining process |
| Dressing environment | Toileting environment | Dining environment |
| Health/biological considerations | Health/biological considerations | |
| Adaptation/functioning | ||
| Food/beverage/appetite |
ONGOING CARE: BPSD
- Recommendations
- Social and physical environmental triggers
- Non-pharmacological practices
- Investment for implementation
- Protocols
- Evaluation of effectiveness
Sensory Practices
| Practice | Evidence | Outcomes |
|---|---|---|
| Aromatherapy | Moderate | Positive effect on agitation |
| Massage | Small | Positive effects on agitation, aggression, anxiety, depression, disruptive vocalizations |
| Multi-sensory stimulation | Large | Positive effects on agitation, anxiety, apathy, depression |
| Bright light therapy | Moderate | Mixed effects |
Psychosocial Practices
| Practice | Evidence | Outcomes |
|---|---|---|
| Validation therapy | Small | Positive effects on agitation, apathy, irritability, night-time disturbance |
| Reminiscence therapy | Moderate | Positive effects on mood, depressive symptoms |
| Music therapy | Moderate | Positive effects on a range of BPSDs, including anxiety, agitation, and apathy, particularly with personalized music practices |
| Pet therapy | Small | Preliminary positive effects on agitation, apathy, disruptive behavior |
| Meaningful activities | Moderate | Mixed--some positive effects on agitation; larger effect sizes for activities that are individually tailored |
Structured Care Protocols
| Practice | Evidence | Outcomes |
|---|---|---|
| Mouth Care | Small | Preliminary: positive effects on care-resistant behaviors |
| Bathing | Small | Positive effects on agitation |
WORKFORCE
- Recommendations
- Orientation and training, and ongoing training
- Person-centered information systems
- Teamwork and interdepartmental/interdisciplinary collaboration
- Caring and supportive leadership team
- Relationships
- Continuous improvement
Long-Term Care Workforce Principles
- Staffing levels should be adequate to allow for proper care at all times--day and night.
- Staff should be sufficiently trained in all aspects of care, including dementia care.
- Staff should be adequately compensated for their valuable work.
- Staff should work in a supportive atmosphere that appreciates their contributions to overall quality care. Improved working environments will result in reduced turnover in all care settings.
- Staff should have the opportunity for career growth.
- Staff should work with families in both residential care settings and home health agencies.
SUPPORTIVE AND THERAPEUTIC ENVIRONMENT
- Recommendations
- Sense of community
- Comfort and dignity
- Courtesy, concern and safety
- Opportunities for choice
- Meaningful engagement
TRANSITION AND COORDINATION OF SERVICES
- Recommendations
- Education about common transitions in care
- Timely communication of information between, across and within settings
- Preferences and goals of the person living with dementia
- Strong inter-professional collaborative team to assist with transitions
- Evidence-based models
Common Transitions
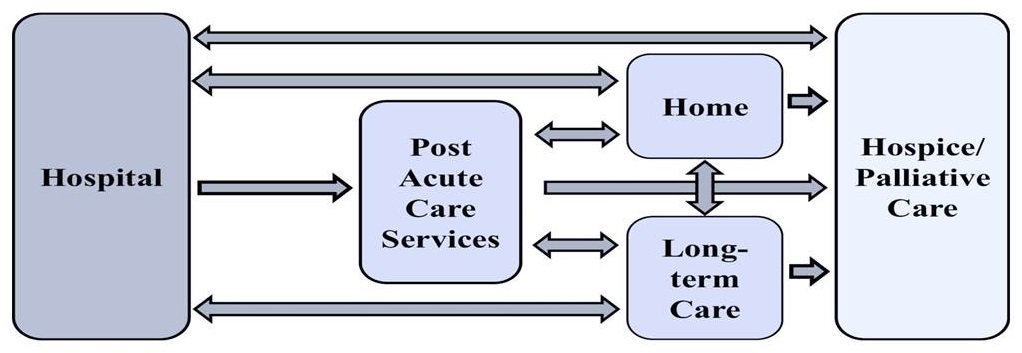 |
Psychosocial/Psychoeducational Interventions
| Author | Setting | Intervention | Description | Outcomes |
|---|---|---|---|---|
| Mittelman et al. (2006) | Home | New York University (NYU) Model | Enhanced counseling and support intervention versus usual care | Time to was over 1.5 years longer than usual care group |
| Brodaty et al. (1997) | Psych hospital | Dementia Caregiver Training (DCT) Program | 10 day intensive psycho-educational program for caregivers. | Time to placement was statistically significantly delayed |
| Hanson et al. (2017 | Nursing home | Goals of Care (GOC) Intervention | OC video with structured care planning discussion versus informational video and standard care planning | Residents had half as many hospitalizations; Family members rated their overall quality of communication with staff higher at three months, and the quality of end-of-life care communication with staff higher at 9 months |
Care Coordination Interventions
| Author | Setting | Intervention | Description | Outcomes |
|---|---|---|---|---|
| Naylor et al. (2014) | Hospital to home | Transitional Care Model (TCM) | Augmented Standard Care versus Resource Nurse Care versus TCM | Time to first rehospitalization was longest for those in the TCM, and rehospitalization or death was accelerated for both other groups |
| Samus et al. (2014) | Home | MIND at Home | Dementia care coordination versus usual care | Significant delay in time to transition from home and remained in home 51 days longer |
| Bass et al. (2014) | Home | Partners in Dementia Care (PDC) | Care coordination program versus usual care | Fewer hospitalizations and fewer emergency department visits |
| Bellantonio et al. (2008) | Assisted living | Geriatrics Team Intervention (GTI) | Four systematic inter professional geriatric team assessments | Reductions in the risk of unanticipated transitions, including hospitalizations, ED visits and nursing home placement, as well as death |
Dementia Care Practice Recommendations
|
Quality Care in Long-Term & Community-Based Care
- Dementia Care Practice Recommendations
- Influencers
- Federal and State Policies
- National Provider Member Organization Partnerships
- Accreditation Bodies
- Programs
- Organization-Wide Consultative Coaching
- Curriculum Review
- essentiALZ® Certification
- Project ECHO
- Dementia Care Provider Roundtable
- Dementia Care In-Person Training
- Impact
- Number of Covered Lives
- Number of Organizations
- Outcomes Research
Questions?
Alzheimer's Association
We're here. All day, every day.
24/7 Helpline: 800.272.3900
April 27, 2018 -- Advisory Council Meeting #28
The meeting was held on Friday, April 27, 2018, in Washington, DC. During the meeting, the Clinical Care Subcommittee took charge of the theme, focusing on advancing consensus on dementia care elements to guide new outcomes measurement. The Council heard speakers in two sessions, one focused on developing consensus about dementia care elements, and the second on models that are informing outcomes measurement. The meeting also included updates on work from the previous meetings, a presentation on the final report from the October 2017 Care Summit, and federal workgroup updates. Material available from this meeting is listed below or at https://aspe.hhs.gov/advisory-council-alzheimers-research-care-and-services-meetings#Apr2018.
Comments and questions, or alerts to broken links, should be sent to napa@hhs.gov.
General Information
-
Agenda -- [HTML Version] [PDF Version]
-
Meeting Announcement -- [HTML Version] [PDF Version]
-
Meeting Summary -- [HTML Version] [PDF Version]
-
Public Comments -- [HTML Version]
Handouts
-
Main Summit Recommendations -- [HTML Version] [PDF Version]
-
National Research Summit on Care, Services, and Supports for Persons with Dementia and Their Caregivers: Report to the National Advisory Council on Alzheimer's Research, Care, and Services -- [HTML Version] [PDF Version]
Presentation Slides
-
Age-Friendly Health Systems -- [HTML Version] [PDF Version]
-
Alzheimer's Disease and Related Dementias Research Update -- [HTML Version] [PDF Version]
-
Care Planning and Health Information Technology: How to Aid Dementia Quality Care -- [HTML Version] [PDF Version]
-
Clinical Care Subcommittee Agenda: Advancing Consensus on Dementia Care Elements to Guide New Outcomes Measurement -- [HTML Version] [PDF Version]
-
Clinical Subcommittee Update -- [HTML Version] [PDF Version]
-
Defining Quality Dementia Care -- [HTML Version] [PDF Version]
-
Final Report to the NAPA Advisory Council -- [HTML Version] [PDF Version]
-
Long-Term Services and Supports Committee Update -- [HTML Version] [PDF Version]
-
Quality Care from the Perspectives of People Living with Dementia -- [HTML Version] [PDF Version]
-
Research Summit on Dementia Care: Building Evidence for Services and Supports Process Report -- [HTML Version] [PDF Version]
-
Testing the Promise of Primary Care: Comprehensive Primary Care Plus (CPC+) -- [HTML Version] [PDF Version]
-
Updates and Follow-Up from January Meeting -- [HTML Version] [PDF Version]